Advanced Recomp Stack Quick Start
The Advanced Recomp Stack combines three research peptides in one protocol: retatrutide, CJC-1295 (No DAC), and ipamorelin. The goal is straightforward. Lose fat fast with retatrutide. Hold onto muscle with the CJC-1295 + ipamorelin pairing, which boosts your body's own growth hormone (GH) output.
Retatrutide is dosed once a week in milligrams. CJC-1295 and ipamorelin are dosed once or twice a day in micrograms. That mg-vs-mcg gap is the number one source of dose errors on this stack, so label every vial clearly.
Reconstitute
Separate vials for each compound. Pre-blended CJC/Ipa vials reduce three reconstitutions to two.
Schedule
1 weekly subQ shot for retatrutide. 1-2 daily subQ shots for CJC/Ipa, pre-bed and fasted.
Easy measuring
Use a U-100 insulin syringe. 100 mcg of CJC or ipa from a 2,000 mcg/mL solution = 5 units.
Supplies
U-100 insulin syringes, bacteriostatic water, alcohol swabs, sharps container.
Research status
Not FDA-approved. WADA prohibits CJC-1295 and ipamorelin in tested sport.
Disclaimer
This page is an educational research reference. It is not medical advice. No published human trial has tested retatrutide + CJC-1295 + ipamorelin together. Retatrutide is an investigational Phase 3 compound. CJC-1295 and ipamorelin are not FDA-approved for human use.
Need broader context on combining peptides? See PepPal's stacking safety guide. For supplier and quality-control context, see the PepPal supplier directory.
What Is the Advanced Recomp Stack?
The Advanced Recomp Stack is a 3-compound body recomposition protocol. It pairs the strongest weight-loss peptide in current clinical development with the most established growth-hormone (GH) peptide combination.
What Each Compound Does
Retatrutide (LY3437943) is a triple agonist. It activates three receptors at once: GLP-1, GIP, and glucagon. GLP-1 cuts appetite and slows digestion. GIP improves how your body handles fat and insulin. Glucagon tells your liver to burn stored fat. That triple action is why retatrutide produces stronger weight-loss results than single-receptor drugs like semaglutide.
CJC-1295 (No DAC) is a short-acting GHRH analog. It tells your pituitary gland to release a pulse of growth hormone. The No DAC version produces short, natural-style GH pulses. The with-DAC version keeps GH levels elevated for days, which does not match how your body normally pulses GH.
Ipamorelin is a selective GH secretagogue. It also tells the pituitary to release GH, but through a separate receptor (the ghrelin receptor). Stacking CJC-1295 + ipamorelin amplifies the GH pulse beyond what either peptide does alone.
Why People Stack Them
When you lose weight fast, you lose some muscle alongside the fat. That is true with any aggressive caloric deficit, including the one retatrutide creates. The CJC-1295 + ipamorelin layer is added to push GH and IGF-1 (a downstream growth signal) higher, which supports lean-tissue retention, recovery, sleep quality, and connective-tissue repair during the deficit.
Retatrutide and CJC/Ipa work through different biological systems. Retatrutide hits metabolic receptors (GLP-1R, GIPR, GCGR). CJC-1295 and ipamorelin hit growth-hormone receptors (GHRH-R and GHS-R1a). There is no overlap and no competition between them. That separation is the main reason this combination is pharmacologically rational.
Evidence boundary
No clinical trial has tested retatrutide + CJC-1295 + ipamorelin together. The combination is community-derived from individual-compound research. The strongest direct evidence here is for retatrutide alone (Phase 2 and Phase 3 trial data).
Advanced Recomp Stack Dosing Protocol & Schedule
Evidence-Level Notice
Retatrutide dosing is based on Phase 2 and Phase 3 clinical trial escalation schedules. CJC-1295 and ipamorelin dosing is based on published human PK/PD data and long-running community protocols. No trial has tested all three together.
Advanced Recomp Stack Dosing Guide
Choose the CJC/Ipa format you are using to see the matching schedule. Retatrutide dosing is the same in both versions.
Most common workflow: retatrutide solo vial + separate (or pre-blended combo) CJC-1295 and ipamorelin vials.
Separate-vial workflow
Three vials, two injection cadences
Retatrutide is injected once a week. CJC-1295 + ipamorelin are injected together once or twice a day. Use separate syringes for retatrutide vs CJC/Ipa - the unit math is different.
Injection burden
1 weekly + 1-2 daily injections
Best for
Most users; matches Phase 3 retatrutide cadence
Cycle driver
CJC/Ipa cycled 12 weeks on / 4 weeks off
Retatrutide
- Loading
- 2 mg/week (weeks 1-4)
- Frequency
- 1x weekly
- Maintenance
- 9-12 mg/week (weeks 17-20+)
- Route
- SubQ; titrate +2 mg every 4 weeks
CJC-1295 (No DAC)
- Loading
- 100 mcg (weeks 1-2)
- Frequency
- 1-2x daily
- Maintenance
- 100-200 mcg, 1-2x daily
- Route
- SubQ; pre-bed required, AM optional
Ipamorelin
- Loading
- 100 mcg (weeks 1-2)
- Frequency
- 1-2x daily
- Maintenance
- 100-200 mcg, 1-2x daily
- Route
- SubQ; injected with CJC-1295
Weekly Schedule Example (Maintenance, Weeks 12+)
Monday
Retatrutide 9-12 mg (weekly shot) + CJC-1295 200 mcg + Ipamorelin 200 mcg pre-bed
Tuesday
CJC-1295 200 mcg + Ipamorelin 200 mcg pre-bed
Wednesday
CJC-1295 200 mcg + Ipamorelin 200 mcg pre-bed
Thursday
CJC-1295 200 mcg + Ipamorelin 200 mcg pre-bed
Friday
CJC-1295 200 mcg + Ipamorelin 200 mcg pre-bed
Saturday
Off (5-on / 2-off rhythm)
Sunday
Off (5-on / 2-off rhythm)
Use one syringe for retatrutide and a second syringe for CJC/Ipa. Different unit math, different vials.
Retatrutide Titration Phases
Retatrutide weekly subQ dosing - 5-phase titration
Phase
Initiation
Weeks
1-4
Weekly Dose
2 mg
Notes
Starting dose; assess GI tolerance.
Phase
Early escalation
Weeks
5-8
Weekly Dose
4 mg
Notes
Increase by 2 mg every 4 weeks.
Phase
Mid escalation
Weeks
9-12
Weekly Dose
6 mg
Notes
Watch GI side effects; slow if needed.
Phase
Therapeutic range
Weeks
13-16
Weekly Dose
9 mg
Notes
Skip to 9 mg or hold at 6 mg by tolerance.
Phase
Maximum dose
Weeks
17-20+
Weekly Dose
12 mg
Notes
Highest dose studied; not all users need it.
| Phase | Weeks | Weekly Dose | Notes |
|---|---|---|---|
| Initiation | 1-4 | 2 mg | Starting dose; assess GI tolerance. |
| Early escalation | 5-8 | 4 mg | Increase by 2 mg every 4 weeks. |
| Mid escalation | 9-12 | 6 mg | Watch GI side effects; slow if needed. |
| Therapeutic range | 13-16 | 9 mg | Skip to 9 mg or hold at 6 mg by tolerance. |
| Maximum dose | 17-20+ | 12 mg | Highest dose studied; not all users need it. |
If GI side effects are severe at any step, hold the current dose for an extra 4 weeks before escalating.
CJC-1295 + Ipamorelin Ramp-Up
CJC-1295 (No DAC) + Ipamorelin daily subQ dosing
Phase
Assessment
Weeks
1-2
CJC-1295
100 mcg
Ipamorelin
100 mcg
Frequency
1x daily
Timing
Pre-bed, fasted
Phase
Standard
Weeks
3-12+
CJC-1295
100-200 mcg
Ipamorelin
100-200 mcg
Frequency
1-2x daily
Timing
Pre-bed required; AM optional
Phase
Aggressive
Weeks
8-16+
CJC-1295
200 mcg
Ipamorelin
200 mcg
Frequency
2x daily
Timing
AM fasted + pre-bed
| Phase | Weeks | CJC-1295 | Ipamorelin | Frequency | Timing |
|---|---|---|---|---|---|
| Assessment | 1-2 | 100 mcg | 100 mcg | 1x daily | Pre-bed, fasted |
| Standard | 3-12+ | 100-200 mcg | 100-200 mcg | 1-2x daily | Pre-bed required; AM optional |
| Aggressive | 8-16+ | 200 mcg | 200 mcg | 2x daily | AM fasted + pre-bed |
Stay fasted at least 2 hours before and 30 minutes after each CJC/Ipa shot. Insulin blunts GH release.
Same protocol with one less reconstitution. The CJC-1295 + ipamorelin combo vial is one product. Retatrutide stays as a separate vial.
Blend ratio
5 mg / 5 mg
1:1 CJC-1295 : Ipamorelin
A 10 mg combo vial contains 5 mg CJC-1295 (No DAC) + 5 mg ipamorelin. Reconstituted with 2 mL bacteriostatic water for a 5,000 mcg/mL total-blend concentration (2,500 mcg/mL per peptide).
Reconstitute
2 mL BAC water
Concentration
2,500 mcg/mL per peptide
Daily draw
8 units = 0.08 mL = ~200 mcg of each
Typical cycle
12-16 weeks
Dose selector
Pre-Blended CJC/Ipa Combo Vial
| CJC-1295 (No DAC) | ~100 mcg |
|---|---|
| Ipamorelin | ~100 mcg |
The combo vial removes one reconstitution but locks in a fixed 1:1 ratio. Pick separate vials if you need to run CJC-1295 lower than ipamorelin or vice versa.
Retatrutide is not in the combo vial. It stays as its own weekly subQ injection. The titration table and weekly schedule are the same as the separate-vials tab above.
Retatrutide Titration (Same in Both Formats)
Retatrutide weekly subQ dosing
Phase
Initiation
Weeks
1-4
Weekly Dose
2 mg
Notes
Start; assess GI tolerance.
Phase
Early escalation
Weeks
5-8
Weekly Dose
4 mg
Notes
Step up every 4 weeks.
Phase
Mid escalation
Weeks
9-12
Weekly Dose
6 mg
Notes
Watch GI; slow if needed.
Phase
Therapeutic range
Weeks
13-16
Weekly Dose
9 mg
Notes
Step to 9 mg or hold at 6 mg.
Phase
Maximum dose
Weeks
17-20+
Weekly Dose
12 mg
Notes
Highest dose studied.
| Phase | Weeks | Weekly Dose | Notes |
|---|---|---|---|
| Initiation | 1-4 | 2 mg | Start; assess GI tolerance. |
| Early escalation | 5-8 | 4 mg | Step up every 4 weeks. |
| Mid escalation | 9-12 | 6 mg | Watch GI; slow if needed. |
| Therapeutic range | 13-16 | 9 mg | Step to 9 mg or hold at 6 mg. |
| Maximum dose | 17-20+ | 12 mg | Highest dose studied. |
Cycle Guidelines
Common Advanced Recomp Stack cycle approaches
Approach
Standard cycle
Duration
12-16 weeks
Off Period
4 weeks off CJC/Ipa; retatrutide can continue
Best For
Moderate recomp; first-time users
Approach
Extended cycle
Duration
16-24 weeks
Off Period
4-6 weeks off CJC/Ipa
Best For
Aggressive recomp; experienced users
Approach
Continuous reta + cycled GH
Duration
Retatrutide ongoing; CJC/Ipa 12 on / 4 off
Off Period
4-week CJC/Ipa breaks
Best For
Long-term body composition management
| Approach | Duration | Off Period | Best For |
|---|---|---|---|
| Standard cycle | 12-16 weeks | 4 weeks off CJC/Ipa; retatrutide can continue | Moderate recomp; first-time users |
| Extended cycle | 16-24 weeks | 4-6 weeks off CJC/Ipa | Aggressive recomp; experienced users |
| Continuous reta + cycled GH | Retatrutide ongoing; CJC/Ipa 12 on / 4 off | 4-week CJC/Ipa breaks | Long-term body composition management |
Receptor desensitization (when receptors become less responsive over time) is the main reason CJC/Ipa is cycled. Retatrutide does not desensitize the same way.
Protocol Notes
- One weekly retatrutide shot + 1-2 daily CJC/Ipa shots. All subQ.
- Fasted timing around CJC/Ipa injections. Community protocols typically fast 2 hours before and 30 minutes after CJC/Ipa injections; insulin blunts GH release.
- CJC/Ipa dosing rhythm. Community protocols commonly use a 5-on / 2-off rhythm for CJC/Ipa to reduce receptor desensitization and provide a recovery window.
- Gradual retatrutide escalation. Community protocols start at 2 mg regardless of prior GLP-1 experience, stepping up no faster than every 4 weeks and slowing escalation when gastrointestinal tolerance has not adapted.
- CJC-1295 formulation. This protocol is built around CJC-1295 No DAC rather than the with-DAC version. No DAC matches the body's natural GH pulse pattern. With-DAC keeps GH elevated for days, which is not the intended fit for this protocol.
- Label every vial. Retatrutide is in mg. CJC/Ipa is in mcg. That is a 1,000x gap and the most common dose error on this stack.
Advanced Recomp Stack Supplies Needed
Plan based on the maintenance schedule above: one weekly retatrutide shot + daily CJC/Ipa shots with a 5-on / 2-off rhythm.
Recommended USA Supply
Choose your region
Use discount code SAVE10 at Peptira checkout. See why we love Peptira.
Ipamorelin + CJC Blend

At-Home Blood Test
Research Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Retatrutide Vials
Vial count depends on size and weekly dose. Math below assumes 10 mg vials.
| Cycle length | Planning note |
|---|---|
12 weeks (avg 6 mg/week) 8 vials | 72 mg total needed; 10 mg per vial. |
16 weeks (avg 9 mg/week) 15 vials | 144 mg total needed; 10 mg per vial. |
20 weeks (avg 9-12 mg/week) 20 vials | Approx 200 mg total needed; 10 mg per vial. |
24 weeks (avg 12 mg/week) 29 vials | 288 mg total needed; 10 mg per vial. |
12 weeks (avg 6 mg/week)
8 vials
72 mg total needed; 10 mg per vial.
16 weeks (avg 9 mg/week)
15 vials
144 mg total needed; 10 mg per vial.
20 weeks (avg 9-12 mg/week)
20 vials
Approx 200 mg total needed; 10 mg per vial.
24 weeks (avg 12 mg/week)
29 vials
288 mg total needed; 10 mg per vial.
CJC-1295 + Ipamorelin Combo Vials
Math below assumes 10 mg combo vials (5 mg + 5 mg) reconstituted with 2 mL BAC water. One vial delivers about 25 doses of 200 mcg of each peptide.
| Cycle length | Planning note |
|---|---|
12 weeks (1x daily, 5-on/2-off) 4 vials | 60 doses needed (5x12); 25 doses per vial. |
12 weeks (2x daily, 5-on/2-off) 5 vials | 120 doses needed; 25 doses per vial. |
16 weeks (1x daily, 5-on/2-off) 4 vials | 80 doses needed; refresh every 3-4 weeks. |
16 weeks (2x daily, 5-on/2-off) 7 vials | 160 doses needed; ipamorelin stability limits. |
12 weeks (1x daily, 5-on/2-off)
4 vials
60 doses needed (5x12); 25 doses per vial.
12 weeks (2x daily, 5-on/2-off)
5 vials
120 doses needed; 25 doses per vial.
16 weeks (1x daily, 5-on/2-off)
4 vials
80 doses needed; refresh every 3-4 weeks.
16 weeks (2x daily, 5-on/2-off)
7 vials
160 doses needed; ipamorelin stability limits.
Insulin Syringes (U-100)
Use 0.3 mL syringes for small CJC/Ipa draws. Use 1 mL syringes when retatrutide doses exceed 1.0 mL.
| Cycle length | Planning note |
|---|---|
12 weeks (1 daily CJC/Ipa + 1 weekly reta) 72 syringes | 60 daily + 12 weekly; recommend 1 x 100-count box. |
16 weeks (1 daily + 1 weekly) 96 syringes | 80 daily + 16 weekly; recommend 1 x 100-count box. |
16 weeks (2 daily + 1 weekly) 176 syringes | 160 daily + 16 weekly; recommend 2 x 100-count boxes. |
24 weeks (2 daily + 1 weekly) 264 syringes | 240 daily + 24 weekly; recommend 3 x 100-count boxes. |
12 weeks (1 daily CJC/Ipa + 1 weekly reta)
72 syringes
60 daily + 12 weekly; recommend 1 x 100-count box.
16 weeks (1 daily + 1 weekly)
96 syringes
80 daily + 16 weekly; recommend 1 x 100-count box.
16 weeks (2 daily + 1 weekly)
176 syringes
160 daily + 16 weekly; recommend 2 x 100-count boxes.
24 weeks (2 daily + 1 weekly)
264 syringes
240 daily + 24 weekly; recommend 3 x 100-count boxes.
Bacteriostatic Water
Most retatrutide 10 mg vials use 1 mL BAC water. Combo CJC/Ipa vials use 2 mL.
| Cycle length | Planning note |
|---|---|
12 weeks 1-2 x 10 mL bottles | Approx 8 mL retatrutide + 8 mL CJC/Ipa across the cycle. |
16 weeks 2-3 x 10 mL bottles | Approx 15 mL retatrutide + 8-14 mL CJC/Ipa across the cycle. |
24 weeks 3-4 x 10 mL bottles | Approx 29 mL retatrutide + 10-14 mL CJC/Ipa across the cycle. |
12 weeks
1-2 x 10 mL bottles
Approx 8 mL retatrutide + 8 mL CJC/Ipa across the cycle.
16 weeks
2-3 x 10 mL bottles
Approx 15 mL retatrutide + 8-14 mL CJC/Ipa across the cycle.
24 weeks
3-4 x 10 mL bottles
Approx 29 mL retatrutide + 10-14 mL CJC/Ipa across the cycle.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments. Ipamorelin reconstituted stability (about 3-4 weeks) is the shortest window in this stack - plan vial refresh cycles around it.
Companion Supplies & Routine Support
Advanced Recomp Stack Blood Tests & Monitoring
This stack combines retatrutide with CJC-1295 no DAC and ipamorelin, so monitoring should cover both incretin/metabolic and GH-axis pathways. The practical focus is glucose control, IGF-1, liver/kidney context, lipids, and cardiovascular symptoms.
Blood test markers to discuss with a clinician
Marker
IGF-1
Why it matters
Tracks downstream GH-axis exposure from the CJC-1295 and ipamorelin components.
Timing
Follow-up
Marker
A1c
Why it matters
Shows longer-term glucose control across both incretin and GH-axis pathways.
Timing
Baseline
Marker
Fasting glucose
Why it matters
Provides a current glucose snapshot during appetite, weight, and GH-axis changes.
Timing
Follow-up
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews kidney function, liver enzymes, electrolytes, and glucose in one broad panel.
Timing
Baseline
Marker
Lipid panel
Why it matters
Tracks cardiometabolic changes during recomposition and weight-loss phases.
Timing
Follow-up
Marker
Blood pressure and resting heart rate
Why it matters
Adds cardiovascular context because retatrutide may affect heart rate and weight loss can change blood pressure.
Timing
Follow-up
| Marker | Why it matters | Timing |
|---|---|---|
| IGF-1 | Tracks downstream GH-axis exposure from the CJC-1295 and ipamorelin components. | Follow-up |
| A1c | Shows longer-term glucose control across both incretin and GH-axis pathways. | Baseline |
| Fasting glucose | Provides a current glucose snapshot during appetite, weight, and GH-axis changes. | Follow-up |
| Comprehensive metabolic panel (CMP) | Reviews kidney function, liver enzymes, electrolytes, and glucose in one broad panel. | Baseline |
| Lipid panel | Tracks cardiometabolic changes during recomposition and weight-loss phases. | Follow-up |
| Blood pressure and resting heart rate | Adds cardiovascular context because retatrutide may affect heart rate and weight loss can change blood pressure. | Follow-up |
Monitoring guidance combines incretin-pathway evidence for retatrutide with GH-axis monitoring logic for CJC-1295 no DAC and ipamorelin.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with diabetes, thyroid cancer history, gallbladder history, pancreatitis history, sleep apnea, edema, cancer history, or kidney disease.
Follow-up
Re-check metabolic markers and IGF-1 after 6-8 weeks, with earlier review if GI symptoms, glucose symptoms, or fluid retention occur.
Longer term
For longer protocols, review metabolic, IGF-1, kidney, liver, and cardiovascular trends every 3 months with a clinician.
How to interpret the labs
- This stack combines pathways that can pull glucose interpretation in different directions.
- GI symptoms, dehydration, edema, numbness, sleep apnea symptoms, and severe abdominal pain need symptom-based review.
- Personal or family thyroid cancer history, MEN2 history, diabetes medications, and cancer history are important clinician discussion points.
Do not wait for routine labs
Severe abdominal pain, persistent vomiting, rapid swelling, chest pain, shortness of breath, fainting, or allergic symptoms need medical review. Severe headaches, vision changes, or new neurologic symptoms should not wait for routine labs.
Advanced Recomp Stack Reconstitution Guide
Critical: mg vs mcg
Retatrutide is dosed in milligrams (mg). CJC-1295 and ipamorelin are dosed in micrograms (mcg). That is a 1,000x difference. Label every vial with compound name, concentration, and reconstitution date. A retatrutide-style mg draw on a CJC vial would deliver 1,000x the intended dose.
Choose Your Reconstitution Format
Math is different for retatrutide vs CJC/Ipa, and different again for separate CJC and Ipa vials vs the pre-blended combo.
Each compound reconstituted on its own.
Retatrutide Reconstitution
Retatrutide reconstitution math
Vial Size
5 mg
BAC Water
1 mL
Concentration
5 mg/mL
2 mg dose
0.4 mL (40 U)
4 mg dose
0.8 mL (80 U)
8 mg dose
—
12 mg dose
—
Vial Size
10 mg
BAC Water
2 mL
Concentration
5 mg/mL
2 mg dose
0.4 mL (40 U)
4 mg dose
0.8 mL (80 U)
8 mg dose
1.6 mL (160 U)*
12 mg dose
—
Vial Size
10 mg
BAC Water
1 mL
Concentration
10 mg/mL
2 mg dose
0.2 mL (20 U)
4 mg dose
0.4 mL (40 U)
8 mg dose
0.8 mL (80 U)
12 mg dose
1.2 mL (120 U)*
Vial Size
20 mg
BAC Water
2 mL
Concentration
10 mg/mL
2 mg dose
0.2 mL (20 U)
4 mg dose
0.4 mL (40 U)
8 mg dose
0.8 mL (80 U)
12 mg dose
1.2 mL (120 U)*
| Vial Size | BAC Water | Concentration | 2 mg dose | 4 mg dose | 8 mg dose | 12 mg dose |
|---|---|---|---|---|---|---|
| 5 mg | 1 mL | 5 mg/mL | 0.4 mL (40 U) | 0.8 mL (80 U) | — | — |
| 10 mg | 2 mL | 5 mg/mL | 0.4 mL (40 U) | 0.8 mL (80 U) | 1.6 mL (160 U)* | — |
| 10 mg | 1 mL | 10 mg/mL | 0.2 mL (20 U) | 0.4 mL (40 U) | 0.8 mL (80 U) | 1.2 mL (120 U)* |
| 20 mg | 2 mL | 10 mg/mL | 0.2 mL (20 U) | 0.4 mL (40 U) | 0.8 mL (80 U) | 1.2 mL (120 U)* |
*Volumes over 1.0 mL need a larger syringe or a split injection at two sites.
CJC-1295 (No DAC) Reconstitution
CJC-1295 (No DAC) reconstitution math
Vial Size
2 mg
BAC Water
1 mL
Concentration
2,000 mcg/mL
100 mcg dose
0.05 mL (5 U)
200 mcg dose
0.10 mL (10 U)
300 mcg dose
0.15 mL (15 U)
Vial Size
5 mg
BAC Water
2 mL
Concentration
2,500 mcg/mL
100 mcg dose
0.04 mL (4 U)
200 mcg dose
0.08 mL (8 U)
300 mcg dose
0.12 mL (12 U)
Vial Size
5 mg
BAC Water
2.5 mL
Concentration
2,000 mcg/mL
100 mcg dose
0.05 mL (5 U)
200 mcg dose
0.10 mL (10 U)
300 mcg dose
0.15 mL (15 U)
| Vial Size | BAC Water | Concentration | 100 mcg dose | 200 mcg dose | 300 mcg dose |
|---|---|---|---|---|---|
| 2 mg | 1 mL | 2,000 mcg/mL | 0.05 mL (5 U) | 0.10 mL (10 U) | 0.15 mL (15 U) |
| 5 mg | 2 mL | 2,500 mcg/mL | 0.04 mL (4 U) | 0.08 mL (8 U) | 0.12 mL (12 U) |
| 5 mg | 2.5 mL | 2,000 mcg/mL | 0.05 mL (5 U) | 0.10 mL (10 U) | 0.15 mL (15 U) |
Ipamorelin Reconstitution
Ipamorelin reconstitution math
Vial Size
2 mg
BAC Water
1 mL
Concentration
2,000 mcg/mL
100 mcg dose
0.05 mL (5 U)
200 mcg dose
0.10 mL (10 U)
300 mcg dose
0.15 mL (15 U)
Vial Size
5 mg
BAC Water
2 mL
Concentration
2,500 mcg/mL
100 mcg dose
0.04 mL (4 U)
200 mcg dose
0.08 mL (8 U)
300 mcg dose
0.12 mL (12 U)
Vial Size
5 mg
BAC Water
2.5 mL
Concentration
2,000 mcg/mL
100 mcg dose
0.05 mL (5 U)
200 mcg dose
0.10 mL (10 U)
300 mcg dose
0.15 mL (15 U)
| Vial Size | BAC Water | Concentration | 100 mcg dose | 200 mcg dose | 300 mcg dose |
|---|---|---|---|---|---|
| 2 mg | 1 mL | 2,000 mcg/mL | 0.05 mL (5 U) | 0.10 mL (10 U) | 0.15 mL (15 U) |
| 5 mg | 2 mL | 2,500 mcg/mL | 0.04 mL (4 U) | 0.08 mL (8 U) | 0.12 mL (12 U) |
| 5 mg | 2.5 mL | 2,000 mcg/mL | 0.05 mL (5 U) | 0.10 mL (10 U) | 0.15 mL (15 U) |
Combo vial for CJC + ipa, separate vial for retatrutide.
Retatrutide Reconstitution
Same as the separate-vials tab. The most common setup is a 10 mg retatrutide vial + 2 mL BAC water = 5 mg/mL.
Retatrutide reconstitution (common setup)
Vial Size
10 mg
BAC Water
2 mL
Concentration
5 mg/mL
2 mg
40 U
4 mg
80 U
6 mg
120 U*
9 mg
180 U*
12 mg
240 U*
Vial Size
10 mg
BAC Water
1 mL
Concentration
10 mg/mL
2 mg
20 U
4 mg
40 U
6 mg
60 U
9 mg
90 U
12 mg
120 U*
| Vial Size | BAC Water | Concentration | 2 mg | 4 mg | 6 mg | 9 mg | 12 mg |
|---|---|---|---|---|---|---|---|
| 10 mg | 2 mL | 5 mg/mL | 40 U | 80 U | 120 U* | 180 U* | 240 U* |
| 10 mg | 1 mL | 10 mg/mL | 20 U | 40 U | 60 U | 90 U | 120 U* |
*Volumes over 100 U (1 mL on a U-100 insulin syringe) need a larger syringe or a split injection.
CJC-1295 + Ipamorelin Combo Vial Reconstitution
Pre-blended CJC + Ipa reconstitution math (1:1 ratio)
Vial Size
5 mg + 5 mg (10 mg total)
BAC Water
2 mL
Concentration (per peptide)
2,500 mcg/mL each
100 mcg of each
4 U (0.04 mL)
200 mcg of each
8 U (0.08 mL)
300 mcg of each
12 U (0.12 mL)
Vial Size
5 mg + 5 mg
BAC Water
2.5 mL
Concentration (per peptide)
2,000 mcg/mL each
100 mcg of each
5 U (0.05 mL)
200 mcg of each
10 U (0.10 mL)
300 mcg of each
15 U (0.15 mL)
Vial Size
2 mg + 2 mg
BAC Water
2 mL
Concentration (per peptide)
1,000 mcg/mL each
100 mcg of each
10 U (0.10 mL)
200 mcg of each
20 U (0.20 mL)
300 mcg of each
30 U (0.30 mL)
| Vial Size | BAC Water | Concentration (per peptide) | 100 mcg of each | 200 mcg of each | 300 mcg of each |
|---|---|---|---|---|---|
| 5 mg + 5 mg (10 mg total) | 2 mL | 2,500 mcg/mL each | 4 U (0.04 mL) | 8 U (0.08 mL) | 12 U (0.12 mL) |
| 5 mg + 5 mg | 2.5 mL | 2,000 mcg/mL each | 5 U (0.05 mL) | 10 U (0.10 mL) | 15 U (0.15 mL) |
| 2 mg + 2 mg | 2 mL | 1,000 mcg/mL each | 10 U (0.10 mL) | 20 U (0.20 mL) | 30 U (0.30 mL) |
Combo vials lock in a fixed 1:1 ratio. One draw delivers equal amounts of both peptides.
Math Verification
- Retatrutide (10 mg + 2 mL): 10,000 mcg ÷ 2 mL = 5,000 mcg/mL = 5 mg/mL. A 4 mg dose = 4 ÷ 5 = 0.8 mL = 80 units on a U-100 syringe.
- Retatrutide 8 mg on the same vial: 8 ÷ 5 = 1.6 mL = 160 units. Over 1 mL means a larger syringe or split injection.
- CJC-1295 (2 mg + 1 mL): 2,000 mcg ÷ 1 mL = 2,000 mcg/mL. A 200 mcg dose = 200 ÷ 2,000 = 0.10 mL = 10 units.
- Pre-blended CJC + Ipa (5 + 5 mg, 2 mL): 5,000 mcg per peptide ÷ 2 mL = 2,500 mcg/mL each. A 200 mcg draw of each = 200 ÷ 2,500 = 0.08 mL = 8 units.
Reconstituted Stability
Reconstituted stability at 2-8 °C (35.6-46.4 °F)
Peptide
Retatrutide
Reconstituted Stability
28-60 days
Planning Note
Conservative use window: within 28 days. Discard if cloudy.
Peptide
CJC-1295 (No DAC)
Reconstituted Stability
3-4 weeks
Planning Note
Lyophilized powder stays stable much longer when frozen.
Peptide
Ipamorelin
Reconstituted Stability
3-4 weeks
Planning Note
Limiting factor. Time vial refresh around ipamorelin.
Peptide
Pre-blended CJC + Ipa
Reconstituted Stability
3-4 weeks
Planning Note
Limited by ipamorelin. Plan refresh every 3 weeks.
| Peptide | Reconstituted Stability | Planning Note |
|---|---|---|
| Retatrutide | 28-60 days | Conservative use window: within 28 days. Discard if cloudy. |
| CJC-1295 (No DAC) | 3-4 weeks | Lyophilized powder stays stable much longer when frozen. |
| Ipamorelin | 3-4 weeks | Limiting factor. Time vial refresh around ipamorelin. |
| Pre-blended CJC + Ipa | 3-4 weeks | Limited by ipamorelin. Plan refresh every 3 weeks. |
Standard 7-Step Reconstitution (Per Vial)
- 01
Gather supplies
Sterile U-100 insulin syringe (29-31 gauge), bacteriostatic water, alcohol swabs, and the peptide vial.
- 02
Wipe both stoppers
Swab the rubber stopper of the BAC water vial and the peptide vial with alcohol. Let air-dry.
- 03
Draw BAC water
Pull the calculated BAC water volume into the syringe using the target concentration from the tables above.
- 04
Inject slowly down the inner wall
Insert the needle into the peptide vial and inject BAC water slowly down the glass. Do not spray directly onto the lyophilized powder.
- 05
Roll, do not shake
Let the vial sit for 1-2 minutes. Gently roll between your palms until fully dissolved.
- 06
Label the vial
Write compound name, concentration, and reconstitution date directly on the vial.
- 07
Refrigerate immediately
Store at 2-8 °C right after reconstitution. Never freeze reconstituted peptides.
Calculator
Use the PepPal reconstitution calculator for exact unit math across retatrutide, CJC-1295, and ipamorelin in any vial size.
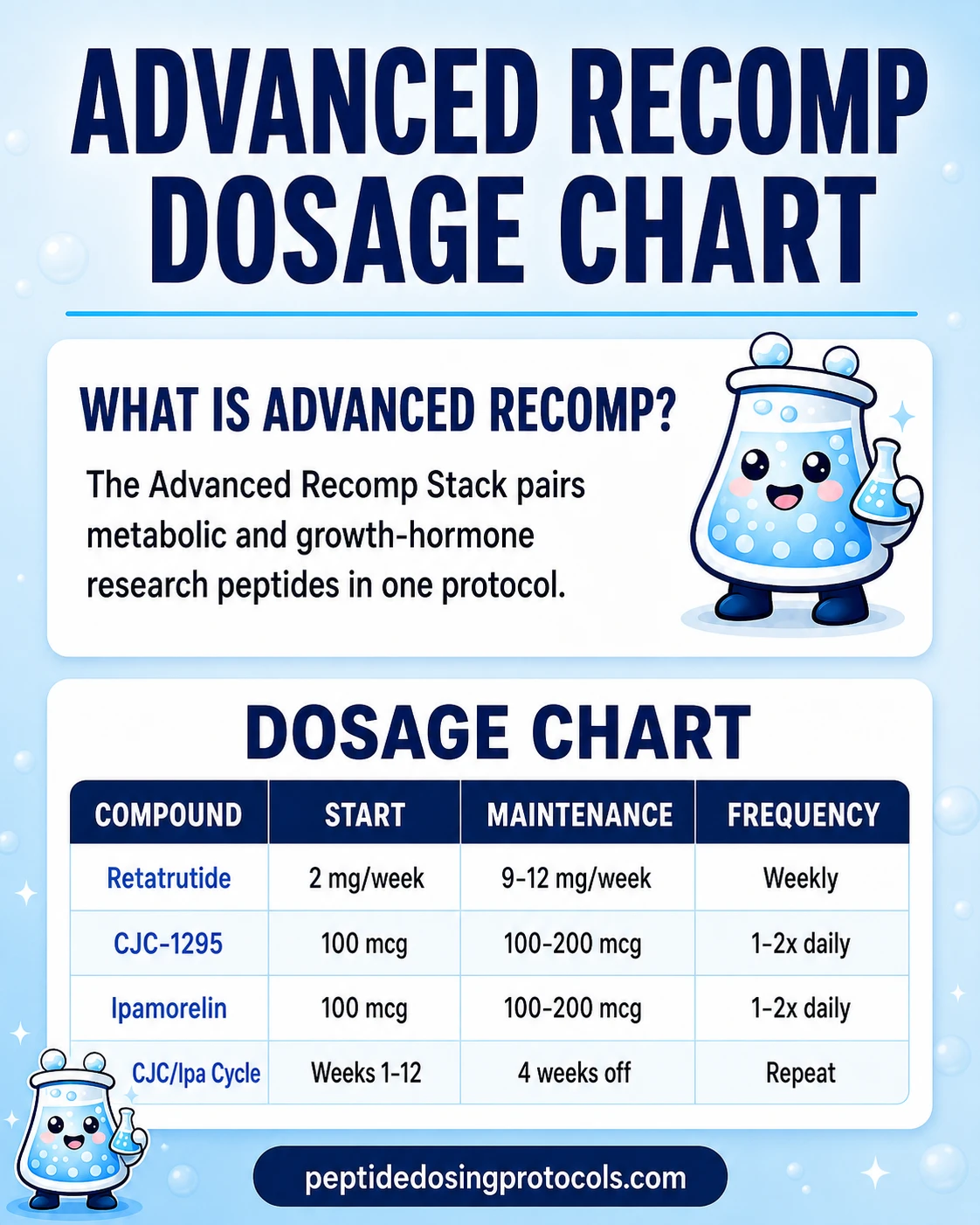
Advanced Recomp Stack Dosage Chart
This Advanced Recomp Stack dosage chart summarizes the retatrutide plus CJC-1295 and ipamorelin research-planning ranges shown in the dosing section above.
Why the Advanced Recomp Stack Adds CJC/Ipa to Retatrutide
Foundation: Retatrutide
Retatrutide alone produced the strongest weight-loss results documented in clinical trials: 24.2% mean body weight reduction at 48 weeks in Phase 2 [NEJM 2023] and 28.7% at 68 weeks in Phase 3 (TRIUMPH-4, December 2025). The triple-receptor action (GLP-1, GIP, glucagon) is the reason it outperforms semaglutide and tirzepatide.
Lean Tissue Protection via Growth Hormone
The problem with fast weight loss - whether from dieting or a peptide - is that you lose muscle alongside fat. CJC-1295 (No DAC) and ipamorelin are added to push GH and IGF-1 (a downstream growth signal) higher, which supports protein retention during a deficit. PepPal's GLP-1 supplement guide covers protein and creatine support during GLP-1 weight loss.
CJC-1295 tells the pituitary to release more GH through the GHRH receptor. Ipamorelin tells the pituitary to release more GH through the ghrelin receptor. Different doors to the same room. Together they produce a bigger GH pulse than either does alone.
Recovery, Sleep, and Training Capacity
CJC-1295 and ipamorelin are typically injected before bed because your body does most of its tissue-repair work overnight. During a deep deficit, you still need to train hard enough to keep your muscle, but you are eating less - so recovery matters more than usual. The CJC/Ipa pair supports collagen production (important for tendons and joints), connective-tissue recovery, and sleep depth.
Two Different Fat-Burning Routes
Retatrutide burns fat mainly by cutting appetite, slowing digestion, and signaling the liver to break down stored fat. Growth hormone burns fat through a different route - it directly signals fat cells to release their stored energy. Stacking the two attacks fat through two independent pathways at the same time.
No Receptor Overlap
Retatrutide hits metabolic receptors (GLP-1R, GIPR, GCGR). CJC-1295 and ipamorelin hit growth-hormone receptors (GHRH-R, GHS-R1a). There is no competition between them. That separation is the pharmacological reason the combination is rational.
Direct stack evidence: none
Every claim above is supported by single-compound research. No published human trial has measured outcomes for the 3-peptide combination together. Treat the stack-level rationale as theoretical, not proven.
Advanced Recomp Stack Side Effects & Safety
Each compound has its own safety profile from clinical or pharmacological studies. No trial has tested all three together. The notes below combine single-compound data and stack-specific considerations.
Retatrutide-Specific Side Effects (TRIUMPH-4, December 2025)
- Nausea: 38-43% (dose-dependent, mostly during step-up).
- Diarrhea: 33-35%.
- Constipation: 22-25%.
- Vomiting: 20-21%.
- Decreased appetite: 18-19%.
- Dysesthesia (an unusual tingling, burning, or prickling sensation in the skin): 8.8% at 9 mg and 20.9% at 12 mg. This is a retatrutide-specific signal tied to glucagon-receptor activity.
- Heart rate increase: about 5-10 bpm above baseline, peaking near week 24, then declining.
- Discontinuation due to adverse events: 12-18%.
CJC-1295 + Ipamorelin Side Effects
- Injection-site reactions (redness, mild swelling).
- Short flushing or warmth after the shot.
- Water retention or mild edema.
- Headache, usually resolving in the first 2 weeks.
- Mild hunger increase from ipamorelin's ghrelin-receptor activity.
- Short fatigue or lightheadedness.
- Tingling or numbness in the hands or feet at higher GH exposure.
Stack-Specific Considerations
- GI side effects come from retatrutide, not CJC/Ipa. Nausea, diarrhea, and vomiting during escalation are retatrutide-driven. Adding daily CJC/Ipa shots adds injection burden, not stomach issues.
- Water retention may stack early on. Both retatrutide and CJC/Ipa can cause mild fluid retention. You may see more puffiness or bloating in the first 4-6 weeks before it levels off.
- Heart-rate tracking during early protocol weeks. Retatrutide raises resting heart rate by about 5-10 bpm. Research-planning notes recommend heart-rate tracking during the first 12 weeks, particularly for those with cardiovascular history — consult a clinician.
- Blood sugar can pull in two directions. Retatrutide improves blood sugar control. Growth hormone can push insulin sensitivity in the other direction. People with pre-diabetes or insulin resistance should monitor blood glucose more often on this stack.
- Three peptides = three quality-control variables. Every additional vial from a grey-market source is another contamination or purity risk. Use COA-verified suppliers for all three compounds.
Need broader stacking-safety context?
See the PepPal side-effects guide.
Advanced Recomp Stack Clinical Evidence Context
Critical note
No published trial has evaluated retatrutide + CJC-1295 (No DAC) + ipamorelin together. The evidence below is per compound, not for the stack.
Retatrutide
Phase 3 TRIUMPH-4 data (December 2025): 28.7% mean weight loss at 68 weeks with 12 mg. Phase 2 NEJM 2023: 24.2% at 48 weeks. MASLD substudy: 82% liver-fat reduction at 24 weeks. The strongest evidence layer in this stack. Reference: Retatrutide Protocol Page.
CJC-1295 (No DAC)
Published human pharmacology data show 2-10x GH elevation and 1.5-3x IGF-1 elevation with preserved natural GH pulse pattern (Teichman et al., 2006; Ionescu et al., 2006). Large body-composition outcome trials are lacking. Reference: CJC-1295 (No DAC) Protocol Page.
Ipamorelin
Selective GH secretagogue. Early studies showed GH release comparable to older GHRPs without cortisol or prolactin elevation (Raun et al., 1998; Gobburu et al., 1999). Human body-composition efficacy trials are lacking. Reference: Ipamorelin Protocol Page.
Stack-level
No clinical trial has measured outcomes for all three together. Stack rationale is built from individual-compound evidence and the mechanistic case for no receptor overlap.
In plain terms: the strongest direct evidence here is for retatrutide alone. The CJC/Ipa layer is supported mainly by human pharmacology data (how the peptides behave in the body) and long-running community practice, not by direct stack outcome trials.
Advanced Recomp Stack Storage & Handling
Storage reference for all three compounds
State
Lyophilized (Powder)
Retatrutide
Room temp or refrigerated; stable 2+ years
CJC-1295 (No DAC)
Freezer preferred; refrigerator acceptable
Ipamorelin
Freezer preferred; refrigerator acceptable
State
Reconstituted (Liquid)
Retatrutide
35.6-46.4 °F (2-8 °C); use within 28 days
CJC-1295 (No DAC)
35.6-46.4 °F (2-8 °C); 3-4 weeks
Ipamorelin
35.6-46.4 °F (2-8 °C); 3-4 weeks
State
Appearance
Retatrutide
Clear, colorless
CJC-1295 (No DAC)
Clear, colorless
Ipamorelin
Clear, colorless
State
Oral viable
Retatrutide
No
CJC-1295 (No DAC)
No
Ipamorelin
No
State
Freeze reconstituted
Retatrutide
No
CJC-1295 (No DAC)
No
Ipamorelin
No
| State | Retatrutide | CJC-1295 (No DAC) | Ipamorelin |
|---|---|---|---|
| Lyophilized (Powder) | Room temp or refrigerated; stable 2+ years | Freezer preferred; refrigerator acceptable | Freezer preferred; refrigerator acceptable |
| Reconstituted (Liquid) | 35.6-46.4 °F (2-8 °C); use within 28 days | 35.6-46.4 °F (2-8 °C); 3-4 weeks | 35.6-46.4 °F (2-8 °C); 3-4 weeks |
| Appearance | Clear, colorless | Clear, colorless | Clear, colorless |
| Oral viable | No | No | No |
| Freeze reconstituted | No | No | No |
Ipamorelin's 3-4 week reconstituted window is the shortest in the stack. Plan vial refresh cycles around ipamorelin.
Do not freeze any reconstituted peptide. Freezing can damage the peptide structure and reduce potency. Lyophilized powder can be stored frozen for long-term storage.
Advanced Recomp Stack vs CagriSema vs Retatrutide Solo vs Reta + MOTS-c
Three common comparisons come up when people search for the best stack to pair with retatrutide. Here is where each one fits.
Advanced Recomp Stack vs common alternatives
Feature
Components
Advanced Recomp Stack
Retatrutide + CJC-1295 (No DAC) + Ipamorelin
CagriSema
Cagrilintide + Semaglutide
Retatrutide Solo
Retatrutide only
Reta + MOTS-c
Retatrutide + MOTS-c
Feature
Receptor targets
Advanced Recomp Stack
GLP-1 + GIP + Glucagon + GHRH + Ghrelin
CagriSema
GLP-1 + Amylin
Retatrutide Solo
GLP-1 + GIP + Glucagon
Reta + MOTS-c
GLP-1 + GIP + Glucagon + mitochondrial
Feature
GH-axis support
Advanced Recomp Stack
Yes
CagriSema
No
Retatrutide Solo
No
Reta + MOTS-c
No
Feature
Peak weight loss
Advanced Recomp Stack
~29% from retatrutide + theoretical lean preservation
CagriSema
~22-24% Phase 3
Retatrutide Solo
~29% Phase 3
Reta + MOTS-c
~29% from reta; mitochondrial support add
Feature
Lean mass preservation
Advanced Recomp Stack
Enhanced via GH + IGF-1
CagriSema
Some amylin signal
Retatrutide Solo
Limited - deficit risk remains
Reta + MOTS-c
Limited
Feature
Injection burden
Advanced Recomp Stack
1 weekly + daily CJC/Ipa
CagriSema
1 weekly combined
Retatrutide Solo
1 weekly
Reta + MOTS-c
1 weekly + 2-3x weekly MOTS-c
Feature
Complexity
Advanced Recomp Stack
High (3 compounds, 3 vials)
CagriSema
Low (single combo)
Retatrutide Solo
Low (single)
Reta + MOTS-c
Moderate
Feature
Cost
Advanced Recomp Stack
High
CagriSema
Moderate
Retatrutide Solo
Moderate
Reta + MOTS-c
Moderate-high
Feature
Evidence level
Advanced Recomp Stack
Phase 3 (reta) + PK (CJC/Ipa); no stack trial
CagriSema
Phase 3 combination data
Retatrutide Solo
Phase 3 monotherapy data
Reta + MOTS-c
Phase 3 (reta); preclinical for MOTS-c
| Feature | Advanced Recomp Stack | CagriSema | Retatrutide Solo | Reta + MOTS-c |
|---|---|---|---|---|
| Components | Retatrutide + CJC-1295 (No DAC) + Ipamorelin | Cagrilintide + Semaglutide | Retatrutide only | Retatrutide + MOTS-c |
| Receptor targets | GLP-1 + GIP + Glucagon + GHRH + Ghrelin | GLP-1 + Amylin | GLP-1 + GIP + Glucagon | GLP-1 + GIP + Glucagon + mitochondrial |
| GH-axis support | Yes | No | No | No |
| Peak weight loss | ~29% from retatrutide + theoretical lean preservation | ~22-24% Phase 3 | ~29% Phase 3 | ~29% from reta; mitochondrial support add |
| Lean mass preservation | Enhanced via GH + IGF-1 | Some amylin signal | Limited - deficit risk remains | Limited |
| Injection burden | 1 weekly + daily CJC/Ipa | 1 weekly combined | 1 weekly | 1 weekly + 2-3x weekly MOTS-c |
| Complexity | High (3 compounds, 3 vials) | Low (single combo) | Low (single) | Moderate |
| Cost | High | Moderate | Moderate | Moderate-high |
| Evidence level | Phase 3 (reta) + PK (CJC/Ipa); no stack trial | Phase 3 combination data | Phase 3 monotherapy data | Phase 3 (reta); preclinical for MOTS-c |
Decision Guidance
- Choose Advanced Recomp Stack when body recomposition (not just weight loss) is the priority and you are comfortable with a more complex daily-plus-weekly injection schedule.
- Choose CagriSema when convenience is the priority. Strong weight loss in a single weekly shot.
- Choose retatrutide solo when maximum fat loss is the only goal and lean-mass protection is handled through diet and resistance training.
- Choose Reta + MOTS-c when mitochondrial support during the deficit matters more than full GH-axis recomp.
FAQ
Q1: What is the Advanced Recomp Stack?
The Advanced Recomp Stack combines retatrutide, CJC-1295 (No DAC), and ipamorelin in a 3-compound body recomposition protocol. Retatrutide drives fat loss. CJC-1295 + ipamorelin boost growth hormone to support lean tissue during the deficit. No published human trial has tested all three together.
Q2: Can you stack retatrutide with CJC-1295 and ipamorelin together?
Yes. Retatrutide and CJC-1295 + ipamorelin work through completely different receptor systems. Retatrutide hits metabolic receptors (GLP-1, GIP, glucagon). CJC and ipamorelin hit growth-hormone receptors (GHRH-R, GHS-R1a). There is no receptor overlap. The combination is community-derived, not from a clinical trial.
Q3: How is the Advanced Recomp Stack dosed?
Retatrutide is dosed once a week via subQ injection, titrated from 2 mg up to 9-12 mg over 16-20 weeks. CJC-1295 (No DAC) and ipamorelin are each dosed at 100-200 mcg per shot, 1-2 times daily, with the main shot before bed in a fasted state. Full titration tables are in the dosing section above.
Q4: What is the best peptide to stack with retatrutide?
The most-asked pairing is CJC-1295 (No DAC) + ipamorelin, which is the basis for this Advanced Recomp Stack. The rationale is that retatrutide is the strongest fat-loss compound currently in clinical development, and CJC/Ipa is the most established GH-support combination for lean-tissue preservation during a deficit. Other options include MOTS-c for mitochondrial support and BPC-157 + TB-500 (the Wolverine Stack) for tissue repair.
Q5: Should I use a pre-blended CJC + ipamorelin vial or separate vials?
Most users pick the pre-blended CJC/Ipa combo vial because it cuts reconstitution from three vials to two and locks in a 1:1 ratio. Separate vials are better if you need to run one peptide higher than the other. Retatrutide always stays as its own separate vial.
Q6: How do you reconstitute the Advanced Recomp Stack?
Each compound is reconstituted on its own. Common setups: retatrutide 10 mg + 2 mL BAC water = 5 mg/mL; CJC-1295 2 mg + 1 mL BAC water = 2,000 mcg/mL; ipamorelin 5 mg + 2.5 mL BAC water = 2,000 mcg/mL. For a pre-blended CJC + ipa combo vial (5 mg + 5 mg) reconstituted with 2 mL BAC water, you get 2,500 mcg/mL of each peptide.
Q7: Why use CJC-1295 without DAC instead of the with-DAC version?
CJC-1295 No DAC produces short GH pulses - your levels spike, then come back down, which matches the body's natural rhythm. The with-DAC version keeps GH elevated for days. This stack is built around natural-style pulses, so the No DAC version is the intended fit. No DAC is also easier to adjust if you need to change your dose.
Q8: How long should you run the Advanced Recomp Stack?
Standard cycles run 12-16 weeks. Extended cycles run 16-24 weeks. CJC-1295 + ipamorelin are usually cycled 12 weeks on and 4 weeks off to reduce receptor desensitization. Retatrutide can continue through the CJC/Ipa off-period when ongoing weight-management support is needed.
Q9: Is the Advanced Recomp Stack safe? What are the main risks?
No clinical trial has tested all three together. The biggest known risks are retatrutide-driven GI side effects (nausea 38-43%, diarrhea 33-35%) and dysesthesia - an unusual skin tingling or burning sensation at higher doses. Adding CJC/Ipa brings injection-site reactions and mild water retention. People with pre-diabetes or insulin resistance should monitor blood glucose more often because retatrutide and GH push insulin sensitivity in opposite directions.
Q10: Can women run retatrutide stacked with CJC-1295 and ipamorelin?
The mechanistic case for the stack is the same regardless of sex. Retatrutide Phase 3 trials included both men and women. CJC-1295 and ipamorelin pharmacology data does not show sex-specific concerns. None of the three compounds have human safety data in pregnancy or breastfeeding, and they are not FDA-approved. Anyone considering this protocol should review the safety section above and consult a qualified clinician.
Q11: What is the best needle size for CJC-1295 + ipamorelin injections?
A 29-31 gauge, half-inch U-100 insulin syringe is standard for CJC/Ipa subQ injections. Daily CJC/Ipa draws are usually 4-15 units (under 0.15 mL), so a 0.3 mL (30-unit) syringe gives the most accurate measurement. For retatrutide, larger draws may need a 1 mL syringe.
Q12: Can retatrutide and CJC-1295 + ipamorelin be injected at different sites?
Yes. Retatrutide is dosed weekly in milligrams. CJC and ipamorelin are dosed daily in micrograms. Use a separate syringe for each (the unit math is different). Rotate injection sites - abdomen, thigh, and the back of the upper arm are common subQ sites for all three compounds.
Q13: Does retatrutide cause excessive muscle loss without CJC + ipamorelin?
Rapid weight loss with any peptide tends to cause some muscle loss alongside fat loss. That is the exact concern this stack is built around. The CJC + ipamorelin layer is added to push GH and IGF-1 higher, which supports protein retention during the deficit. Adequate protein intake and regular resistance training matter just as much.
Q14: Can you swap from retatrutide to CJC-1295 + ipamorelin?
These compounds do not interchange. Retatrutide is a metabolic fat-loss compound. CJC-1295 + ipamorelin is a GH-support combination. Swapping retatrutide for CJC/Ipa removes the fat-loss driver from the protocol. If the goal is to taper off retatrutide, the more common approach is to maintain the CJC/Ipa layer during and after the retatrutide taper to support recomposition.
Q15: What calculator should I use for Advanced Recomp Stack reconstitution math?
Use the PepPal calculator. Calculate each compound separately because retatrutide is dosed in mg while CJC and ipamorelin are dosed in mcg - a 1,000x difference.
Q16: Is this medical advice?
No. This page is an educational research reference. Retatrutide is investigational and not FDA-approved. CJC-1295 (No DAC) and ipamorelin are research peptides not approved for human therapeutic use. No clinical trial has evaluated this specific combination. Consult a qualified clinician before considering any peptide protocol.
Sources & Research
- 1. Jastreboff AM, Kaplan LM, Frias JP, et al. Triple-Hormone-Receptor Agonist Retatrutide for Obesity - A Phase 2 Trial. New England Journal of Medicine (2023)
- 2. Eli Lilly and Company Lilly's triple agonist, retatrutide, delivered weight loss of up to an average of 71.2 lbs along with substantial relief from osteoarthritis pain in first successful Phase 3 trial. Press Release (2025)
- 3. Teichman SL, Neale A, Lawrence B, et al. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. Journal of Clinical Endocrinology & Metabolism (2006)
- 4. Ionescu M, Frohman LA Pulsatile secretion of growth hormone (GH) persists during continuous stimulation by CJC-1295, a long-acting GH-releasing hormone analog. Journal of Clinical Endocrinology & Metabolism (2006)
- 5. Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology (1998)
- 6. Gobburu JV, Agerso H, Jusko WJ, Ynddal L Pharmacokinetic-pharmacodynamic modeling of ipamorelin, a growth hormone releasing peptide, in human volunteers. Pharmaceutical Research (1999)
- 7. Rosenstock J, Frias J, Jastreboff AM, et al. Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo and active-controlled, parallel-group, phase 2 trial. The Lancet (2023)
- 8. Sanyal AJ, Kaplan LM, Frias JP, et al. Triple-Hormone-Receptor Agonist Retatrutide for Metabolic Dysfunction-Associated Steatotic Liver Disease: A Randomized Phase 2a Trial. Nature Medicine (2024)
- 9. Ishida J, Saitoh M, Ebner N, et al. Growth hormone secretagogues: history, mechanism of action, and clinical development. JCSM Rapid Communications (2020)
- 10. Alba M, Fintini D, Sagazio A, et al. Once-daily administration of CJC-1295, a long-acting growth hormone-releasing hormone (GHRH) analog, normalizes growth in the GHRH knockout mouse. American Journal of Physiology - Endocrinology and Metabolism (2006)
- 11. ClinicalTrials.gov A Study of Retatrutide (LY3437943) Once Weekly in Participants With Obesity and Knee Osteoarthritis (TRIUMPH-4). Identifier: NCT05931367. Clinical Trial Registry (2025)
- 12. Urva S, Coskun T, Loh MT, et al. LY3437943, a novel triple GIP, GLP-1, and glucagon receptor agonist in people with type 2 diabetes: a phase 1b, multicentre, double-blind, placebo-controlled, randomised, multiple-ascending dose trial. The Lancet (2022)
- 13. World Anti-Doping Agency The Prohibited List 2026. WADA (2026)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page