CJC-1295 No DAC Quick Start
CJC-1295 No DAC, also called Modified GRF 1-29 or Mod GRF 1-29, is a short-acting copy of the body's own growth-hormone-releasing hormone (GHRH). It tells the pituitary gland to release a short burst of growth hormone, then clears the body in about 30 minutes.
Researchers planning protocols usually pair it with Ipamorelin because the two compounds push the pituitary through different doors at the same time. CJC-1295 No DAC is not FDA-approved and is used only in research-reference contexts.
Half-life
About 30 minutes. Each dose creates one short pulse, then fades.
Common dose range
100–300 mcg per injection, 1–3 times daily in fasted windows.
Default vial setup
10 mg vial with 3 mL bacteriostatic water gives a clean 3,333 mcg/mL working solution.
Route
Subcutaneous (SubQ) with a U-100 insulin syringe.
Status
Not FDA-approved. Educational research reference only.
Disclaimer
This page is an educational research reference and is not medical advice or a treatment plan. CJC-1295 No DAC is not approved by the FDA for human use.
This no-DAC page covers dose timing and setup. Want the bigger CJC view? See the CJC-1295 research overview. It covers effects, studies, safety notes, and legal status.
CJC-1295 No DAC Dosing Protocol & Schedule
Most CJC-1295 No DAC research protocols start low and increase slowly. The short half-life means each dose is mostly independent, so timing the dose around fasted windows usually matters more than chasing a higher number.
Typical Titration Pattern
Common CJC-1295 No DAC titration framework
Phase
Initiation
Window
Weeks 1–2
Dose per injection
100 mcg, once daily
Notes
Pre-bed in a fasted window. Used to check tolerance.
Phase
Early escalation
Window
Weeks 3–4
Dose per injection
150 mcg, once daily
Notes
Increase by 50 mcg only if initiation is tolerated.
Phase
Therapeutic range
Window
Weeks 5–8
Dose per injection
200 mcg, once daily
Notes
Common maintenance level in community protocols.
Phase
Advanced range
Window
Weeks 5–12+
Dose per injection
200–300 mcg, 1–2x daily
Notes
Often split between morning fasted and pre-bed windows.
Phase
Upper community range
Window
Protocol-dependent
Dose per injection
Up to 300 mcg, up to 3x daily
Notes
Higher single doses tend to add side effects without bigger GH gains.
| Phase | Window | Dose per injection | Notes |
|---|---|---|---|
| Initiation | Weeks 1–2 | 100 mcg, once daily | Pre-bed in a fasted window. Used to check tolerance. |
| Early escalation | Weeks 3–4 | 150 mcg, once daily | Increase by 50 mcg only if initiation is tolerated. |
| Therapeutic range | Weeks 5–8 | 200 mcg, once daily | Common maintenance level in community protocols. |
| Advanced range | Weeks 5–12+ | 200–300 mcg, 1–2x daily | Often split between morning fasted and pre-bed windows. |
| Upper community range | Protocol-dependent | Up to 300 mcg, up to 3x daily | Higher single doses tend to add side effects without bigger GH gains. |
Not a dosing recommendation. This is a summary of community protocol structure used for research planning.
Why Frequency Often Beats a Higher Single Dose
Researchers describe a saturation point: roughly 100 mcg seems to fill the available pituitary receptors for a single pulse. Pushing past that with a larger single dose does not usually create a much larger growth hormone burst. That is why most planning frameworks add a second daily injection before they raise the size of one dose.
Timing Rules That Show Up in Most Protocols
- Inject in a fasted window. Food, especially carbs, can dampen the GH pulse because insulin blunts GH signaling.
- A common rule is at least 2 hours after eating and 30 minutes before eating again.
- Pre-bed dosing lines up with the body's largest natural GH pulse during deep sleep.
- Skipping a dose is not a problem because the half-life is short. Do not double up the next day.
- Many planning frameworks use 5-days-on / 2-days-off, or 8–12 week cycles followed by 4–6 weeks off, to manage receptor sensitivity.
Cycle Guidelines
Cycle length patterns in community planning
Approach
Short cycle
Length
4–6 weeks
Off period
2–4 weeks
Common use
Test tolerance and response.
Approach
Standard cycle
Length
8–12 weeks
Off period
4–6 weeks
Common use
Most common maintenance pattern.
Approach
Pulsed week
Length
5 days on / 2 days off
Off period
Built into cycle
Common use
Used to keep pituitary receptors responsive.
| Approach | Length | Off period | Common use |
|---|---|---|---|
| Short cycle | 4–6 weeks | 2–4 weeks | Test tolerance and response. |
| Standard cycle | 8–12 weeks | 4–6 weeks | Most common maintenance pattern. |
| Pulsed week | 5 days on / 2 days off | Built into cycle | Used to keep pituitary receptors responsive. |
These cycle structures come from community-derived planning. No randomized trial defines an ideal cycle length for the No DAC variant.
Evidence boundary
No published human trial has tested the No DAC variant directly at protocol scale. These dosing patterns are extrapolated from parent CJC-1295 research, GHRH pharmacology, and community use.
CJC-1295 No DAC Supplies Needed
These supplies are planned around the 10 mg vial / 3 mL BAC water default and a daily injection schedule.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

CJC-1295 No DAC Supply

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials (10 mg default)
At 200 mcg per daily injection, one 10 mg vial covers roughly 50 doses. At 100 mcg per dose it covers up to 100 doses. Once daily dosing is used in this plan.
| Cycle length | Planning note |
|---|---|
4-6 weeks 1 vial | 4 weeks: 28 daily injections; one 10 mg vial covers the cycle.; 6 weeks: 42 daily injections; still within one 10 mg vial. |
8-12 weeks 2 vials | 8 weeks: 56 daily injections; one vial covers 50 doses, second vial gives margin.; 12 weeks: 84 daily injections; two vials cover 100 doses. |
4-6 weeks
1 vial
4 weeks: 28 daily injections; one 10 mg vial covers the cycle.; 6 weeks: 42 daily injections; still within one 10 mg vial.
8-12 weeks
2 vials
8 weeks: 56 daily injections; one vial covers 50 doses, second vial gives margin.; 12 weeks: 84 daily injections; two vials cover 100 doses.
Insulin Syringes (U-100, 0.3 mL / 30-unit)
Smaller barrels make it easier to read low unit counts like 3 or 6 units at the 10 mg / 3 mL default.
| Cycle length | Planning note |
|---|---|
4 weeks 28 syringes | One syringe per injection. |
6 weeks 42 syringes | One syringe per injection. |
8 weeks 56 syringes | One syringe per injection. |
12 weeks 84 syringes | One syringe per injection. |
4 weeks
28 syringes
One syringe per injection.
6 weeks
42 syringes
One syringe per injection.
8 weeks
56 syringes
One syringe per injection.
12 weeks
84 syringes
One syringe per injection.
Bacteriostatic Water
Each 10 mg vial uses 3 mL BAC water. A 10 mL bottle covers about 3 vials with margin.
| Cycle length | Planning note |
|---|---|
4-12 weeks 1 x 10 mL bottle | 4 weeks: 3 mL used; bottle has plenty of margin.; 8 weeks: 6 mL used across 2 vials; still within one bottle.; 12 weeks: 6–9 mL used across 2 vials; one bottle covers margin. |
4-12 weeks
1 x 10 mL bottle
4 weeks: 3 mL used; bottle has plenty of margin.; 8 weeks: 6 mL used across 2 vials; still within one bottle.; 12 weeks: 6–9 mL used across 2 vials; one bottle covers margin.
Round up for priming losses, dropped syringes, and protocol adjustments. If you split into 1–2x daily dosing, double the syringe and swab counts.
Companion Supplies & Routine Support
CJC-1295 No DAC Reconstitution Guide
The default setup on this page is the 10 mg vial with 3 mL bacteriostatic water. That gives a working solution of about 3,333 mcg/mL, which makes the most common research doses snap to clean unit numbers on a U-100 insulin syringe.
Default: 10 mg Vial + 3 mL BAC Water
10 mg / 3 mL setup → 3,333 mcg/mL. Units shown for a U-100 syringe.
Target dose
100 mcg
Volume to draw
0.03 mL
U-100 syringe units
3 units
Target dose
150 mcg
Volume to draw
0.045 mL
U-100 syringe units
~4.5 units
Target dose
200 mcg
Volume to draw
0.06 mL
U-100 syringe units
6 units
Target dose
300 mcg
Volume to draw
0.09 mL
U-100 syringe units
9 units
| Target dose | Volume to draw | U-100 syringe units |
|---|---|---|
| 100 mcg | 0.03 mL | 3 units |
| 150 mcg | 0.045 mL | ~4.5 units |
| 200 mcg | 0.06 mL | 6 units |
| 300 mcg | 0.09 mL | 9 units |
Use a 0.3 mL / 30-unit syringe for easier reading at these small volumes.
Other Common Vial / BAC Water Combinations
Reconstitution reference for other common formats
Vial
2 mg
BAC water
1.0 mL
Concentration
2,000 mcg/mL
100 mcg
5 units
200 mcg
10 units
300 mcg
15 units
Vial
2 mg
BAC water
2.0 mL
Concentration
1,000 mcg/mL
100 mcg
10 units
200 mcg
20 units
300 mcg
30 units
Vial
5 mg
BAC water
2.0 mL
Concentration
2,500 mcg/mL
100 mcg
4 units
200 mcg
8 units
300 mcg
12 units
Vial
5 mg
BAC water
3.0 mL
Concentration
1,667 mcg/mL
100 mcg
6 units
200 mcg
12 units
300 mcg
18 units
Vial
5 mg
BAC water
5.0 mL
Concentration
1,000 mcg/mL
100 mcg
10 units
200 mcg
20 units
300 mcg
30 units
Vial
10 mg
BAC water
3.0 mL
Concentration
3,333 mcg/mL
100 mcg
3 units
200 mcg
6 units
300 mcg
9 units
Vial
10 mg
BAC water
5.0 mL
Concentration
2,000 mcg/mL
100 mcg
5 units
200 mcg
10 units
300 mcg
15 units
| Vial | BAC water | Concentration | 100 mcg | 200 mcg | 300 mcg |
|---|---|---|---|---|---|
| 2 mg | 1.0 mL | 2,000 mcg/mL | 5 units | 10 units | 15 units |
| 2 mg | 2.0 mL | 1,000 mcg/mL | 10 units | 20 units | 30 units |
| 5 mg | 2.0 mL | 2,500 mcg/mL | 4 units | 8 units | 12 units |
| 5 mg | 3.0 mL | 1,667 mcg/mL | 6 units | 12 units | 18 units |
| 5 mg | 5.0 mL | 1,000 mcg/mL | 10 units | 20 units | 30 units |
| 10 mg | 3.0 mL | 3,333 mcg/mL | 3 units | 6 units | 9 units |
| 10 mg | 5.0 mL | 2,000 mcg/mL | 5 units | 10 units | 15 units |
Pick a setup where your most common dose lands on a whole or half unit so it is easy to draw.
Step-By-Step Reconstitution
- 01
Gather supplies
CJC-1295 No DAC vial, bacteriostatic water, alcohol swabs, and a U-100 insulin syringe.
- 02
Clean both stoppers
Wipe the peptide vial stopper and the BAC water vial stopper with separate alcohol swabs. Let them air dry.
- 03
Draw the BAC water
Draw the planned BAC water volume (3 mL for the default 10 mg setup) into a syringe.
- 04
Add the water slowly
Inject the BAC water slowly down the inside wall of the peptide vial. Do not aim the stream at the powder.
- 05
Mix gently
Roll or gently swirl the vial. Do not shake. Shaking can damage the peptide.
- 06
Inspect the solution
The liquid should be clear and free of visible particles. Discard the vial if it is cloudy or discolored.
- 07
Label and store
Write the concentration and reconstitution date on the vial. Refrigerate at 2–8°C (36–46°F) and use within about 2–4 weeks.
Need a custom setup?
Use the PepPal reconstitution calculator to plug in any vial size and BAC water volume and get exact unit counts.
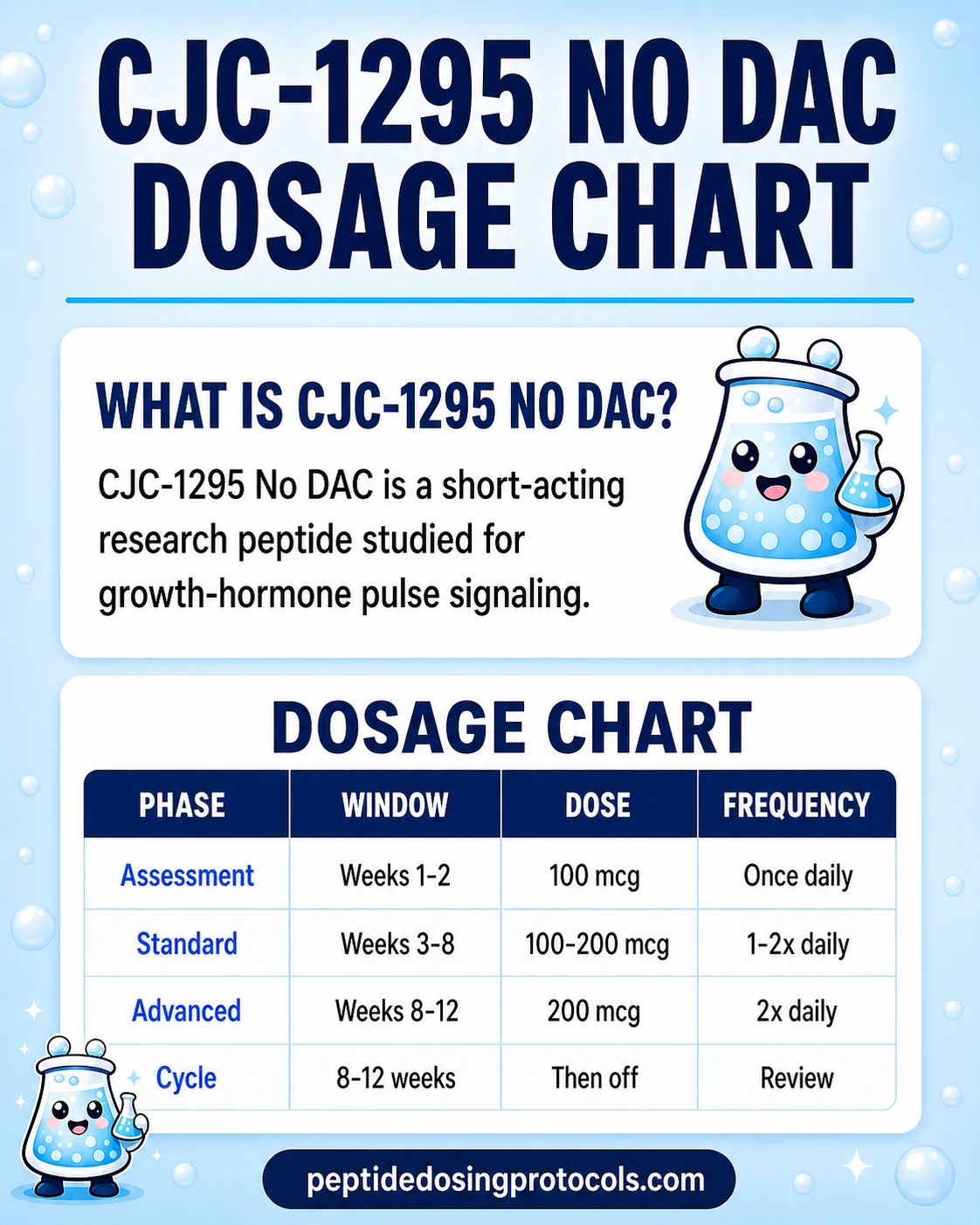
CJC-1295 No DAC Dosage Chart
This CJC-1295 No DAC dosage chart summarizes a common daily titration schedule from 100 mcg up to 200 mcg, with optional advanced dosing shown by week range.
How CJC-1295 No DAC Works
CJC-1295 No DAC is a small change to the body's own growth-hormone-releasing hormone (GHRH). Four edits to the sequence make it last longer than natural GHRH, which only survives a few minutes. The change gives it a half-life of about 30 minutes.
Step One: It Attaches to GHRH Receptors
Once injected, CJC-1295 No DAC travels to the pituitary gland — a small structure at the base of the brain that controls many hormones. It attaches to GHRH receptors on the pituitary and tells the gland to release growth hormone (GH).
Step Two: A Short, Clean GH Pulse
Because the compound clears in about 30 minutes, each dose makes one short GH burst, then fades. That pulsatile pattern is closer to how the body normally releases GH in waves, especially during deep sleep. Many planning frameworks favor it over long-acting compounds because the pulse-and-rest pattern may help keep receptors responsive over time.
Step Three: GH Tells the Liver to Make IGF-1
Each GH pulse signals the liver to produce IGF-1 (insulin-like growth factor 1). IGF-1 is one of the markers researchers track because it carries many of the downstream effects on tissue, muscle, and metabolism.
Why Ipamorelin Often Comes Along
Ipamorelin is a different kind of GH stimulator. It works through the ghrelin receptor, not the GHRH receptor. Pushing both doors at once usually creates a larger GH pulse than either compound alone. That is why CJC-1295 No DAC + Ipamorelin is one of the most discussed GH-related stack patterns in research planning.
Pulsatile signal
Short half-life supports clean, separated GH pulses rather than constant elevation.
GHRH receptor only
Selective for GHRH receptors. Does not directly activate the ghrelin pathway.
Downstream IGF-1
Repeated daily pulses can hold IGF-1 levels higher over time even when each single dose washes out quickly.
Empty-stomach effect
Insulin from a recent meal can blunt the GH pulse, which is why fasted windows are common in planning.
Who CJC-1295 No DAC Is For and Who Should Avoid It
This page is a research-planning reference. The note below covers who research protocols typically exclude, not who can or cannot use the compound personally. There is no human-use approval, and the decision should always involve a licensed clinician.
Groups Most Protocols Exclude
- Active cancer or recent cancer history. GH and IGF-1 can affect cell growth, and most planning frameworks exclude this group by default.
- Meaningful cardiovascular disease, especially uncontrolled heart conditions.
- Pregnancy or breastfeeding.
- Significant glucose dysregulation or uncontrolled diabetes, because GH can raise blood sugar.
- Known hypersensitivity to peptide products or to bacteriostatic water (benzyl alcohol).
Medication Conflicts to Flag
- Glucocorticoids (steroids) can blunt GH response and may complicate planning.
- Insulin and oral diabetes medications may interact with GH-driven glucose changes.
- Thyroid medication adjustments may be relevant because GH affects thyroid hormone conversion.
Clinical oversight
Anything in this section is general research-planning context. Decisions about who should or should not consider any peptide protocol should be made with a licensed clinician who can review individual medical history, labs, and medications.
CJC-1295 No DAC Side Effects & Safety
CJC-1295 No DAC is often described as easier to titrate than the DAC version because side effects fade with the compound itself. Most reported effects pass within 30–60 minutes of a dose.
Commonly Reported Effects
- Mild flushing or warmth shortly after the injection.
- Headache, usually mild and short-lived.
- Injection-site redness or irritation.
- Mild water retention or puffiness.
- Tingling or numbness in the hands, sometimes linked to higher single doses.
Dose-Dependent Pattern
Higher single doses tend to produce more flushing and headache without a proportional GH gain. This is part of why most planning frameworks add a second daily dose before they raise the size of a single dose.
Theoretical Long-Term Concerns
- Long-term effects on insulin sensitivity and blood sugar are not well studied for the No DAC variant.
- Long-term IGF-1 elevation has theoretical implications for cell growth, which is one reason cancer history is treated as an exclusion.
- No multi-year human safety data exists for the No DAC version specifically.
The CJC-1295 with DAC Safety Event
A 2006 Phase 2 trial of CJC-1295 with DAC in HIV patients was halted after a participant had a heart attack. Investigators later said the event was unrelated to the compound, but the program was discontinued. That event is tied to the DAC version, which keeps GH levels elevated for days. No similar signal has been reported for the No DAC variant.
Quality-Control Risk
Because CJC-1295 No DAC is sold as a research compound, purity and identity vary by supplier. Match the certificate of analysis (COA) to the exact product and batch where possible. PepPal tracks COA depth and independent testing on its supplier comparison pages.
CJC-1295 No DAC Timeline & What to Monitor
There is no large outcome trial that maps response timelines for the No DAC variant. The general timing markers below come from parent-compound research, GH/IGF-1 physiology, and community planning.
General timing markers used in planning
Window
Per-dose (0–60 min)
What protocols typically look at
Short flushing, mild headache, or warmth around the injection time. These fade with the compound.
Window
First 1–2 weeks
What protocols typically look at
Tolerance check at 100 mcg before stepping up. Sleep quality is the most commonly reported early marker.
Window
Weeks 4–6
What protocols typically look at
Many planning frameworks treat this as a useful checkpoint for IGF-1 labs and to decide whether to raise dose or frequency.
Window
Weeks 8–12
What protocols typically look at
Most cycles wrap up in this range, followed by 4–6 weeks off.
| Window | What protocols typically look at |
|---|---|
| Per-dose (0–60 min) | Short flushing, mild headache, or warmth around the injection time. These fade with the compound. |
| First 1–2 weeks | Tolerance check at 100 mcg before stepping up. Sleep quality is the most commonly reported early marker. |
| Weeks 4–6 | Many planning frameworks treat this as a useful checkpoint for IGF-1 labs and to decide whether to raise dose or frequency. |
| Weeks 8–12 | Most cycles wrap up in this range, followed by 4–6 weeks off. |
Markers are general planning references. They are not promises of an outcome.
Markers a Clinician May Track
- IGF-1, often before starting and again at 4–6 weeks.
- Fasting glucose and HbA1c, because GH can raise blood sugar over time.
- Sleep quality, sometimes tracked with a simple journal or wearable.
- Body composition, if that is the research focus, usually via consistent body-fat measurement methods.
Stopping rule
Most planning frameworks include a stopping rule: if side effects do not resolve, if IGF-1 rises far above range, or if blood sugar climbs meaningfully, the cycle is paused and reviewed with a clinician.
CJC-1295 No DAC Clinical Evidence Context
Human evidence for the No DAC variant specifically is limited. Most published human data covers the parent CJC-1295 sequence, with several Phase 1 studies and one halted Phase 2 trial.
Teichman et al. 2006 (JCEM, Phase 1)
CJC-1295 produced sustained GH and IGF-1 elevation in healthy adults with short-term tolerability data.
Ionescu and Frohman 2006 (JCEM)
Showed that pulsatile GH secretion was preserved during CJC-1295 stimulation.
Alba et al. 2006 (preclinical)
Daily CJC-1295 in GHRH-knockout mice normalized growth and body-composition markers.
Jette et al. 2005 (Endocrinology)
Identified CJC-1295 as a long-lasting GRF analog and described its albumin-binding chemistry.
ConjuChem Phase 2, 2006 (NCT00267527, DAC version)
Halted in HIV patients after a cardiac event. Investigators said the event was unrelated, but the program was discontinued. This trial used the DAC version, not No DAC.
What This Means for No DAC
No large clinical trial has been run specifically on the No DAC variant. Current dosing patterns rest on the parent CJC-1295 research above, the physiology of GHRH signaling, and the simple fact that the No DAC version uses the same receptor with a much shorter half-life. The cardiac event in the Phase 2 trial is tied to the DAC variant, not the short-acting No DAC version.
CJC-1295 No DAC Storage & Handling
Storage reference for CJC-1295 No DAC
Form
Lyophilized (powder)
Temperature
-4°F (-20°C) or below
Window
12–24+ months
Form
Lyophilized (powder)
Temperature
36–46°F (2–8°C)
Window
Several months
Form
Lyophilized (powder)
Temperature
Room temperature
Window
Short shipping window only
Form
Reconstituted
Temperature
36–46°F (2–8°C)
Window
2–4 weeks
Form
Reconstituted, frozen aliquots
Temperature
-4°F (-20°C)
Window
3–4 months
| Form | Temperature | Window |
|---|---|---|
| Lyophilized (powder) | -4°F (-20°C) or below | 12–24+ months |
| Lyophilized (powder) | 36–46°F (2–8°C) | Several months |
| Lyophilized (powder) | Room temperature | Short shipping window only |
| Reconstituted | 36–46°F (2–8°C) | 2–4 weeks |
| Reconstituted, frozen aliquots | -4°F (-20°C) | 3–4 months |
Protect from light, avoid repeated freeze-thaw cycles, and discard cloudy or discolored solutions.
- Use bacteriostatic water (not plain sterile water) for multi-dose vials. The benzyl alcohol keeps the solution stable for weeks in the fridge.
- Store the vial upright, away from light, on a stable fridge shelf rather than the door.
- If you freeze aliquots, thaw in the fridge rather than at room temperature.
CJC-1295 No DAC Protocol Mistakes & Troubleshooting
Cloudy or Discolored Vial
Discard the vial. Reconstituted CJC-1295 No DAC should be clear and colorless. Cloudiness usually means contamination or peptide degradation.
You Used the Wrong BAC Water Volume
The peptide is not ruined if your concentration is different from the chart. Recalculate the unit count using your real volume. Add the new concentration label to the vial so you do not draw the old dose by mistake. The calculator can handle any vial / volume combo.
Missed Dose
Skip it and resume the schedule. The half-life is short, so each dose is largely independent. Do not double up the next day.
Strong Flushing or Headache
Usually a sign the per-dose number is too high. Most planning frameworks step back to 100 mcg and add frequency before going higher. Effects usually fade within 30–60 minutes.
Vial Sat at Room Temperature
Short shipping windows are normal. Long room-temperature exposure after reconstitution shortens stability. If reconstituted product has been warm for more than a day or two, treat it as suspect.
Confused About Daily vs Twice-Daily
Most plans start once daily pre-bed, then add a morning fasted dose only after the single dose is tolerated. Twice daily is not required.
CJC-1295 No DAC Regulatory Status
As of June 2026, CJC-1295 No DAC (Modified GRF 1-29) is not FDA-approved. It has no active clinical development pathway tied to the No DAC variant. It sits in the same category as many other research-use peptides and is sold for research reference, not human use.
- Not FDA-approved for any indication.
- Not on the FDA's approved drug list as of June 2026.
- Not a dietary supplement and not legal to market as one.
- Banned for athletes under the World Anti-Doping Agency (WADA) S2 category.
- Not interchangeable with FDA-approved GHRH analogs such as Tesamorelin (Egrifta).
Regulatory status changes from time to time. Confirm current FDA status on the FDA website before relying on any planning document.
CJC-1295 No DAC vs CJC-1295 with DAC vs Sermorelin vs Ipamorelin
CJC-1295 No DAC sits in a family of GH-related research compounds. The table below lines up the four most often compared.
GH secretagogue comparison
Property
Class
CJC-1295 No DAC
GHRH analog
CJC-1295 with DAC
GHRH analog (binds albumin)
Sermorelin
GHRH analog
Ipamorelin
GHRP (ghrelin mimetic)
Property
Half-life
CJC-1295 No DAC
~30 minutes
CJC-1295 with DAC
6–8 days
Sermorelin
10–20 minutes
Ipamorelin
~2 hours
Property
Dosing frequency
CJC-1295 No DAC
1–3x daily
CJC-1295 with DAC
1–2x weekly
Sermorelin
1–2x daily
Ipamorelin
1–3x daily
Property
Common dose range
CJC-1295 No DAC
100–300 mcg per injection
CJC-1295 with DAC
1,000–2,000 mcg per week
Sermorelin
100–500 mcg per injection
Ipamorelin
100–300 mcg per injection
Property
GH release shape
CJC-1295 No DAC
Pulsatile, physiological
CJC-1295 with DAC
Sustained elevation
Sermorelin
Pulsatile
Ipamorelin
Brief, selective pulse
Property
FDA status
CJC-1295 No DAC
Not approved
CJC-1295 with DAC
Not approved
Sermorelin
Previously approved; discontinued
Ipamorelin
Not approved
Property
Standout feature
CJC-1295 No DAC
Cleanest pulsatile GHRH signal; easy titration
CJC-1295 with DAC
Convenient weekly dosing
Sermorelin
Longest medical track record
Ipamorelin
GH pulse without cortisol or prolactin rise
| Property | CJC-1295 No DAC | CJC-1295 with DAC | Sermorelin | Ipamorelin |
|---|---|---|---|---|
| Class | GHRH analog | GHRH analog (binds albumin) | GHRH analog | GHRP (ghrelin mimetic) |
| Half-life | ~30 minutes | 6–8 days | 10–20 minutes | ~2 hours |
| Dosing frequency | 1–3x daily | 1–2x weekly | 1–2x daily | 1–3x daily |
| Common dose range | 100–300 mcg per injection | 1,000–2,000 mcg per week | 100–500 mcg per injection | 100–300 mcg per injection |
| GH release shape | Pulsatile, physiological | Sustained elevation | Pulsatile | Brief, selective pulse |
| FDA status | Not approved | Not approved | Previously approved; discontinued | Not approved |
| Standout feature | Cleanest pulsatile GHRH signal; easy titration | Convenient weekly dosing | Longest medical track record | GH pulse without cortisol or prolactin rise |
These compounds are not interchangeable. Each one fits a different planning goal.
- CJC-1295 No DAC and Sermorelin are both GHRH analogs, but CJC-1295 No DAC has a longer per-dose window than Sermorelin.
- CJC-1295 with DAC is more convenient but less physiologically pulsatile.
- Ipamorelin works through a different receptor, which is why it is often stacked with CJC-1295 No DAC rather than compared head-to-head.
- Reconstitution math is different for each one. Use a calculator instead of copying numbers between compounds.
Compound-specific guides: CJC-1295 with DAC, Sermorelin, Ipamorelin, and the GHRP-6 peptide guide.
CJC-1295 No DAC Blood Tests & Monitoring
CJC-1295 without DAC is usually discussed as a shorter GH-pulse support peptide. Monitoring focuses on IGF-1 trends, glucose handling, lipids, and fluid-retention symptoms.
Blood test markers to discuss with a clinician
Marker
IGF-1
Why it matters
Shows the downstream signal after repeated GH pulses and helps track pathway intensity.
Timing
Follow-up
Marker
A1c
Why it matters
Reviews longer-term glucose control because GH-axis stimulation can affect insulin sensitivity.
Timing
Baseline
Marker
Fasting glucose
Why it matters
Provides a current glucose snapshot during GH-axis changes.
Timing
Follow-up
Marker
Lipid panel
Why it matters
Tracks cholesterol and triglyceride trends during body-composition changes.
Timing
Baseline
Marker
TSH and free T4
Why it matters
Helps separate thyroid-related symptoms from GH-axis effects.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| IGF-1 | Shows the downstream signal after repeated GH pulses and helps track pathway intensity. | Follow-up |
| A1c | Reviews longer-term glucose control because GH-axis stimulation can affect insulin sensitivity. | Baseline |
| Fasting glucose | Provides a current glucose snapshot during GH-axis changes. | Follow-up |
| Lipid panel | Tracks cholesterol and triglyceride trends during body-composition changes. | Baseline |
| TSH and free T4 | Helps separate thyroid-related symptoms from GH-axis effects. | Optional |
Monitoring guidance is GH-axis pathway-based and extrapolated from human GHRH analog data and GH/IGF physiology.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with diabetes risk, sleep apnea, edema, cancer history, or thyroid disease.
Follow-up
Re-check IGF-1 and metabolic markers after 6-8 weeks or after meaningful protocol changes.
Longer term
For longer protocols, review trends every 3-6 months with a clinician.
How to interpret the labs
- IGF-1 is useful, but symptoms and metabolic labs still matter.
- Shorter-acting GH-pulse protocols may still affect glucose, appetite, sleep, and fluid balance.
- Avoid assuming a normal IGF-1 means the protocol has no risk.
Do not wait for routine labs
Rapid swelling, severe headaches, vision changes, chest pain, or shortness of breath needs medical review. New numbness, wrist pain, or worsening sleep apnea symptoms should be discussed with a clinician.
FAQ
Q1: What is CJC-1295 No DAC?
CJC-1295 No DAC, also called Modified GRF 1-29 or Mod GRF 1-29, is a short-acting GHRH analog. It tells the pituitary gland to release a single growth hormone pulse, then clears the body in about 30 minutes. It is not FDA-approved and is used only in research-reference contexts.
Q2: What is the common starting dose for CJC-1295 No DAC?
A common starting dose in research planning is 100 mcg once daily pre-bed in a fasted window. Many frameworks step up by 50 mcg every one to two weeks toward a 200 mcg daily maintenance level. This is not a dosing recommendation.
Q3: What is CJC-1295 No DAC's half-life?
About 30 minutes. That short half-life is the main reason the No DAC version supports a pulsatile GH pattern and clears much faster than the DAC version, which lasts 6–8 days.
Q4: How do you reconstitute a 10 mg CJC-1295 No DAC vial?
The default setup is a 10 mg vial with 3 mL bacteriostatic water, which gives 3,333 mcg/mL. At that concentration, 100 mcg is 3 units, 200 mcg is 6 units, and 300 mcg is 9 units on a U-100 insulin syringe. Use the PepPal calculator for any custom setup.
Q5: How is CJC-1295 No DAC different from CJC-1295 with DAC?
The No DAC version is short-acting (about 30 minutes) and is usually dosed daily for pulsatile GH release. The DAC version binds to a blood protein (albumin) and lasts 6–8 days, with weekly dosing and sustained GH elevation. They use the same receptor but produce very different signaling patterns.
Q6: Why is CJC-1295 No DAC paired with Ipamorelin?
CJC-1295 No DAC works through the GHRH receptor. Ipamorelin works through the ghrelin receptor. Pushing both pathways at once usually creates a larger GH pulse than either compound alone, which is why the pairing is one of the most discussed GH-related stack patterns in research planning.
Q7: What are the most common side effects?
Commonly reported effects include short flushing, mild headache, injection-site redness, and mild water retention. Effects are usually dose-dependent and fade within 30–60 minutes as the compound clears.
Q8: Is CJC-1295 No DAC FDA-approved?
No. As of June 2026, CJC-1295 No DAC (Modified GRF 1-29) is not FDA-approved for any use. It is an unregulated research compound and is banned for athletes under the World Anti-Doping Agency S2 category.
Q9: Should the dose or the frequency go up first?
Most planning frameworks raise frequency before raising a single dose. The reason is a saturation effect: roughly 100 mcg seems to fill the available pituitary receptors for one pulse, so a much larger single dose does not usually create a much larger GH burst. Adding a second daily injection is typical before stepping past 200 mcg per dose.
Q10: What vial sizes are available for CJC-1295 No DAC?
Common research-supply vial sizes are 2 mg, 5 mg, and 10 mg. Larger vials cost less per mg and last longer per cycle. This page uses a 10 mg vial as the default because 3 mL of BAC water makes most common doses snap to clean unit numbers.
Q11: How long is a typical CJC-1295 No DAC cycle in research planning?
Most planning frameworks use 8–12 week cycles followed by 4–6 weeks off. Shorter 4–6 week blocks are sometimes used to test tolerance first. Some plans use a 5-days-on / 2-days-off pattern inside the cycle to support receptor sensitivity.
Q12: How should reconstituted CJC-1295 No DAC be stored?
Refrigerate the reconstituted vial at 2–8°C (36–46°F) and use within about 2–4 weeks. Longer storage works as frozen single-use aliquots at -20°C (-4°F) for several months. Discard any vial that turns cloudy or discolored.
Q13: Is this page medical advice?
No. This is an educational research reference. CJC-1295 No DAC is not FDA-approved for any use, and the dosing structures shown here are summaries of community planning, not a personal recommendation. Talk to a licensed clinician before considering any peptide protocol.
Sources & Research
- 1. Teichman SL, Neale A, Lawrence B, et al. Prolonged stimulation of growth hormone and IGF-1 secretion by CJC-1295 in healthy adults. Journal of Clinical Endocrinology and Metabolism (2006)
- 2. Ionescu M, Frohman LA. Pulsatile secretion of growth hormone persists during continuous stimulation by CJC-1295. Journal of Clinical Endocrinology and Metabolism (2006)
- 3. Alba M, Fintini D, Sagazio A, et al. Once-daily administration of CJC-1295, a long-acting GHRH analog, normalizes growth in the GHRH knockout mouse. American Journal of Physiology - Endocrinology and Metabolism (2006)
- 4. Jette L, Leger R, Thibaudeau K, et al. Human growth hormone-releasing factor (hGRF)1-29-albumin bioconjugates activate the GRF receptor on the anterior pituitary in rats: identification of CJC-1295 as a long-lasting GRF analog. Endocrinology (2005)
- 5. Sackmann-Sala L, Ding J, Frohman LA, Kopchick JJ. Activation of the GH/IGF-1 axis by CJC-1295 and serum protein changes in normal adults. Growth Hormone & IGF Research (2009)
- 6. Clemmons DR. Long-acting forms of GHRH and growth hormone: effects in normal volunteers and adults with GHD. Hormone Research (2007)
- 7. Henninge J, Pepaj M, Hullstein I, Hemmersbach P. Identification of CJC-1295, a growth-hormone-releasing peptide, in an unknown pharmaceutical preparation. Drug Testing and Analysis (2010)
- 8. ClinicalTrials.gov Effect of CJC-1295 on weekly growth hormone and daily IGF-1 release in adults with HIV-associated lipodystrophy (NCT00267527). ClinicalTrials.gov registry (2006)
- 9. Aidsmap (NAM). Lipodystrophy study halted after patient death (CJC-1295 with DAC, Phase 2). aidsmap.com (2006)
- 10. U.S. Food and Drug Administration. FDA-approved drugs database (used to confirm absence of an approved CJC-1295 No DAC product). FDA.gov (2026)
- 11. World Anti-Doping Agency. Prohibited list (S2 peptide hormones, growth factors, related substances, and mimetics). WADA (2026)
Related Dosing Protocols
Educational use only
This guide is an educational research reference, not medical advice or a treatment plan. CJC-1295 No DAC is not FDA-approved for any use. Consult a licensed clinician before considering any peptide protocol.
Calculate vial math
Use the calculator for custom vial size, BAC water volume, and syringe-unit math.
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page