Tirzepatide Quick Start
Disclaimer
This page is an educational research and dosing reference. It is not medical advice and does not replace guidance from a licensed clinician. Tirzepatide carries a boxed warning for thyroid C-cell tumors. Do not use it without a qualified prescriber if you have a personal or family history of medullary thyroid carcinoma or MEN 2.
Tirzepatide is a once-weekly injection that activates two appetite and blood-sugar hormones at the same time: GIP and GLP-1. The single-target competitor most people know is semaglutide (Ozempic, Wegovy), which only activates GLP-1. Retatrutide goes one step further by adding glucagon receptor activity, but it remains investigational. Tirzepatide activates both GIP and GLP-1, which is why it is called a dual agonist.
It is sold under two brand names. Mounjaro is approved for type 2 diabetes. Zepbound is approved for chronic weight management and for obstructive sleep apnea in adults with obesity. Both are the same drug, the same molecule, and use the same titration ladder. The difference is the indication on the label.
Route
Subcutaneous (under-the-skin) injection, once per week, on the same day each week.
Dose ladder
2.5 → 5 → 7.5 → 10 → 12.5 → 15 mg weekly, with at least 4 weeks between steps.
Measure
Most research vials reconstitute cleanly to 20 mg/mL, where 1 mg = 5 units on a U-100 insulin syringe.
Supplies
Vial, BAC water, U-100 insulin syringes, and alcohol swabs. Reconstituted solution keeps for ~28 days refrigerated.
Research status
FDA-approved drug as Mounjaro/Zepbound. Lyophilized research-use vials are a separate, non-FDA grey-market supply.
Mounjaro vs Zepbound at a glance
Same drug, two indications
Active drug
Mounjaro
Tirzepatide
Zepbound
Tirzepatide
FDA indication
Mounjaro
Type 2 diabetes
Zepbound
Chronic weight management; OSA + obesity
First approved
Mounjaro
May 2022
Zepbound
November 2023
Form sold by Lilly
Mounjaro
Single-use pen
Zepbound
Single-use pen and vial
Titration ladder
Mounjaro
2.5 → 5 → 7.5 → 10 → 12.5 → 15 mg weekly
Zepbound
2.5 → 5 → 7.5 → 10 → 12.5 → 15 mg weekly
| Mounjaro | Zepbound | |
|---|---|---|
| Active drug | Tirzepatide | Tirzepatide |
| FDA indication | Type 2 diabetes | Chronic weight management; OSA + obesity |
| First approved | May 2022 | November 2023 |
| Form sold by Lilly | Single-use pen | Single-use pen and vial |
| Titration ladder | 2.5 → 5 → 7.5 → 10 → 12.5 → 15 mg weekly | 2.5 → 5 → 7.5 → 10 → 12.5 → 15 mg weekly |
The molecule, the dose ladder, and the side-effect profile are identical. The label is the only thing that differs.
Tirzepatide Dosing Protocol & Schedule
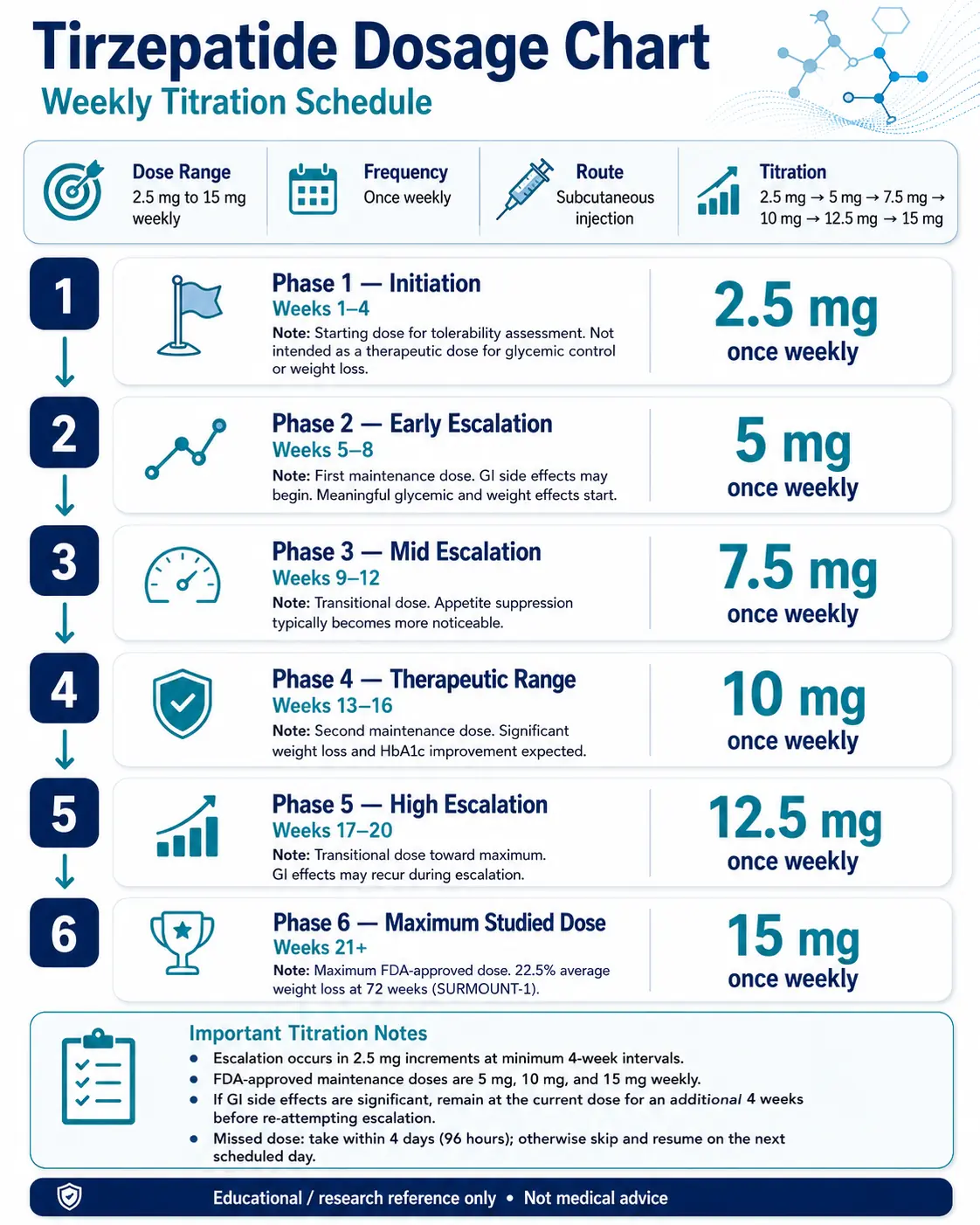
Tirzepatide is dosed once weekly. The dose starts low to let the gut adjust, then steps up every 4 weeks. Each step is a 2.5 mg increment. The minimum-effective dose for weight loss or glycemic control is 5 mg. The maximum studied and approved dose is 15 mg. The 2.5 mg, 7.5 mg, and 12.5 mg doses are transitional steps, not long-term targets.
Tirzepatide Dosing Schedule
Choose the format you are researching. The ladder is the same for Mounjaro and Zepbound; the research-vial tab also shows the matching mg-to-units math.
FDA-approved pen schedule for tirzepatide as Mounjaro (T2D) or Zepbound (obesity / OSA).
Tirzepatide Titration (Mounjaro and Zepbound)
Phase
Phase 1 — Initiation
Weeks
Weeks 1–4
Dose
2.5 mg once weekly
Notes
Tolerability dose. Not a therapeutic dose for weight loss or HbA1c.
Phase
Phase 2 — Early maintenance
Weeks
Weeks 5–8
Dose
5 mg once weekly
Notes
First true maintenance dose. Most users feel reduced appetite here.
Phase
Phase 3 — Mid escalation
Weeks
Weeks 9–12
Dose
7.5 mg once weekly
Notes
Transitional. Hold longer if GI effects flare.
Phase
Phase 4 — Mid maintenance
Weeks
Weeks 13–16
Dose
10 mg once weekly
Notes
Second maintenance dose. Strong weight and HbA1c effects.
Phase
Phase 5 — High escalation
Weeks
Weeks 17–20
Dose
12.5 mg once weekly
Notes
Transitional. GI effects may briefly return.
Phase
Phase 6 — Maximum dose
Weeks
Weeks 21+
Dose
15 mg once weekly
Notes
Maximum FDA-approved dose. ~22.5% weight loss at 72 weeks in SURMOUNT-1.
| Phase | Weeks | Dose | Notes |
|---|---|---|---|
| Phase 1 — Initiation | Weeks 1–4 | 2.5 mg once weekly | Tolerability dose. Not a therapeutic dose for weight loss or HbA1c. |
| Phase 2 — Early maintenance | Weeks 5–8 | 5 mg once weekly | First true maintenance dose. Most users feel reduced appetite here. |
| Phase 3 — Mid escalation | Weeks 9–12 | 7.5 mg once weekly | Transitional. Hold longer if GI effects flare. |
| Phase 4 — Mid maintenance | Weeks 13–16 | 10 mg once weekly | Second maintenance dose. Strong weight and HbA1c effects. |
| Phase 5 — High escalation | Weeks 17–20 | 12.5 mg once weekly | Transitional. GI effects may briefly return. |
| Phase 6 — Maximum dose | Weeks 21+ | 15 mg once weekly | Maximum FDA-approved dose. ~22.5% weight loss at 72 weeks in SURMOUNT-1. |
Three approved maintenance doses: 5 mg, 10 mg, 15 mg. Not everyone needs to climb to 15 mg.
Missed dose
Per the Mounjaro and Zepbound prescribing information, if a dose is missed it should be administered as soon as possible within 4 days (96 hours). After that window, skip the missed dose and resume on the next regularly scheduled day. Do not double up.
Same titration ladder applied to research-grade lyophilized vials, with insulin-syringe units for each step.
Research-grade tirzepatide is supplied as lyophilized powder in 5/10/15/40/60 mg vials. Once reconstituted with BAC water, you draw weekly doses on a U-100 insulin syringe. The cleanest math is a 40 mg vial reconstituted with 2.0 mL of BAC water, which gives 20 mg/mL.
Mg → Units (40 mg vial + 2.0 mL BAC water = 20 mg/mL)
Weekly dose
2.5 mg
Volume
0.125 mL
U-100 syringe units
12.5 units
Weekly dose
5 mg
Volume
0.25 mL
U-100 syringe units
25 units
Weekly dose
7.5 mg
Volume
0.375 mL
U-100 syringe units
37.5 units
Weekly dose
10 mg
Volume
0.50 mL
U-100 syringe units
50 units
Weekly dose
12.5 mg
Volume
0.625 mL
U-100 syringe units
62.5 units
Weekly dose
15 mg
Volume
0.75 mL
U-100 syringe units
75 units
| Weekly dose | Volume | U-100 syringe units |
|---|---|---|
| 2.5 mg | 0.125 mL | 12.5 units |
| 5 mg | 0.25 mL | 25 units |
| 7.5 mg | 0.375 mL | 37.5 units |
| 10 mg | 0.50 mL | 50 units |
| 12.5 mg | 0.625 mL | 62.5 units |
| 15 mg | 0.75 mL | 75 units |
On a 0.5 mL / 50-unit syringe, 12.5 mg and 15 mg need a larger syringe. Use the calculator below for any other vial-and-water pairing.
Calculator
For any vial size or BAC-water volume, use the PepPal reconstitution calculator. Enter vial mg, water volume, and target dose to get exact syringe units.
Research-use only
Research-grade vials are sold for laboratory research, not for human use. Information here is reported for educational reference; nothing on this page is a recommendation to use research-grade tirzepatide outside of an FDA-approved indication.
Tirzepatide weight-loss dose-tier guide
What each dose did in SURMOUNT-1 (obesity, no diabetes, 72 weeks)
Weekly dose
5 mg
Average weight loss
−16.0%
Plain-English read
First real treatment dose. Solid for many.
Weekly dose
10 mg
Average weight loss
−21.4%
Plain-English read
Mid maintenance. Strong weight effect.
Weekly dose
15 mg
Average weight loss
−22.5%
Plain-English read
Maximum dose. Diminishing return vs 10 mg.
| Weekly dose | Average weight loss | Plain-English read |
|---|---|---|
| 5 mg | −16.0% | First real treatment dose. Solid for many. |
| 10 mg | −21.4% | Mid maintenance. Strong weight effect. |
| 15 mg | −22.5% | Maximum dose. Diminishing return vs 10 mg. |
Source: Jastreboff et al., NEJM 2022 (SURMOUNT-1). Most users do not need to escalate to 15 mg to see meaningful results.
Steady state
Tirzepatide has a 5-day half-life. With weekly dosing, blood levels build up over about 4 weeks before stabilizing at roughly 1.6× a single dose. That is why each phase lasts at least 4 weeks — the body needs that time to fully adjust before you can judge the new dose.
Tirzepatide Supplies Needed
Plan supplies based on the titration ladder above: one weekly subcutaneous injection, drawn from a multi-dose vial reconstituted with BAC water. The numbers below assume the most popular setup — a 40 mg vial reconstituted with 2.0 mL BAC water, giving 20 mg/mL.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

Tirzepatide Supply

Compounded Tirzepatide GLP-1/GIP

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Tirzepatide Vials (40 mg, reconstituted to 20 mg/mL)
One injection per week. A 40 mg vial covers 28 days of dosing at most maintenance steps.
| Cycle length | Planning note |
|---|---|
4 weeks (Phase 1, 2.5 mg), 8 weeks (through 5 mg) 1 x 40 mg vial | 4 weeks (Phase 1, 2.5 mg): 4 doses × 2.5 mg = 10 mg total. Vial covers it.; 8 weeks (through 5 mg): Roughly 30 mg used over 8 weeks at the 2.5 → 5 mg ramp. |
12 weeks (through 7.5 mg) 2 x 40 mg vials | Plan a second vial when stepping past 5 mg. |
16 weeks (through 10 mg) 3 x 40 mg vials | 10 mg weekly draws four doses per vial. |
24 weeks (full ladder to 15 mg) 6 x 40 mg vials | Add buffer for any held-dose weeks during GI flares. |
4 weeks (Phase 1, 2.5 mg), 8 weeks (through 5 mg)
1 x 40 mg vial
4 weeks (Phase 1, 2.5 mg): 4 doses × 2.5 mg = 10 mg total. Vial covers it.; 8 weeks (through 5 mg): Roughly 30 mg used over 8 weeks at the 2.5 → 5 mg ramp.
12 weeks (through 7.5 mg)
2 x 40 mg vials
Plan a second vial when stepping past 5 mg.
16 weeks (through 10 mg)
3 x 40 mg vials
10 mg weekly draws four doses per vial.
24 weeks (full ladder to 15 mg)
6 x 40 mg vials
Add buffer for any held-dose weeks during GI flares.
Insulin Syringes (U-100)
One syringe per weekly injection. Use 0.5 mL syringes for ≤50 unit draws and 1 mL syringes for higher doses.
| Cycle length | Planning note |
|---|---|
4 weeks 4 syringes | 1 per weekly injection. |
12 weeks 12 syringes | 1 box of 100 covers a full ladder. |
24 weeks 24 syringes | Add a few extras for dropped or damaged syringes. |
4 weeks
4 syringes
1 per weekly injection.
12 weeks
12 syringes
1 box of 100 covers a full ladder.
24 weeks
24 syringes
Add a few extras for dropped or damaged syringes.
Bacteriostatic Water
2.0 mL per 40 mg vial. Multi-dose 10 mL bottles cover several reconstitutions.
| Cycle length | Planning note |
|---|---|
4 weeks 1 x 10 mL bottle | 1 vial uses 2 mL; bottle covers up to 5 vials. |
24 weeks 2 x 10 mL bottles | 6 vials × 2 mL = 12 mL; second bottle gives margin. |
4 weeks
1 x 10 mL bottle
1 vial uses 2 mL; bottle covers up to 5 vials.
24 weeks
2 x 10 mL bottles
6 vials × 2 mL = 12 mL; second bottle gives margin.
Round up to cover priming losses, dropped syringes, damaged swabs, and dose holds during GI side-effect weeks.
Companion Supplies & Routine Support
Tirzepatide Reconstitution Guide
Reconstitution is the step where you mix lyophilized (freeze-dried) tirzepatide powder with bacteriostatic water (BAC water) so it can be drawn into a syringe. The math is the same for any vial size: total milligrams in the vial divided by milliliters of water added equals the concentration.
Tirzepatide reconstitution by vial size (units assume U-100 insulin syringes)
Vial
5 mg
BAC water
1.0 mL
Concentration
5 mg/mL
2.5 mg
0.50 mL / 50 u
5 mg
1.00 mL / 100 u
7.5 mg
—
10 mg
—
15 mg
—
Vial
10 mg
BAC water
1.0 mL
Concentration
10 mg/mL
2.5 mg
0.25 mL / 25 u
5 mg
0.50 mL / 50 u
7.5 mg
0.75 mL / 75 u
10 mg
1.00 mL / 100 u
15 mg
—
Vial
10 mg
BAC water
2.0 mL
Concentration
5 mg/mL
2.5 mg
0.50 mL / 50 u
5 mg
1.00 mL / 100 u
7.5 mg
—
10 mg
—
15 mg
—
Vial
15 mg
BAC water
1.5 mL
Concentration
10 mg/mL
2.5 mg
0.25 mL / 25 u
5 mg
0.50 mL / 50 u
7.5 mg
0.75 mL / 75 u
10 mg
1.00 mL / 100 u
15 mg
1.50 mL / split
Vial
40 mg
BAC water
2.0 mL
Concentration
20 mg/mL
2.5 mg
0.125 mL / 12.5 u
5 mg
0.25 mL / 25 u
7.5 mg
0.375 mL / 37.5 u
10 mg
0.50 mL / 50 u
15 mg
0.75 mL / 75 u
Vial
40 mg
BAC water
3.0 mL
Concentration
13.33 mg/mL
2.5 mg
0.188 mL / 18.8 u
5 mg
0.375 mL / 37.5 u
7.5 mg
0.563 mL / 56.3 u
10 mg
0.75 mL / 75 u
15 mg
1.125 mL / split
Vial
60 mg
BAC water
3.0 mL
Concentration
20 mg/mL
2.5 mg
0.125 mL / 12.5 u
5 mg
0.25 mL / 25 u
7.5 mg
0.375 mL / 37.5 u
10 mg
0.50 mL / 50 u
15 mg
0.75 mL / 75 u
| Vial | BAC water | Concentration | 2.5 mg | 5 mg | 7.5 mg | 10 mg | 15 mg |
|---|---|---|---|---|---|---|---|
| 5 mg | 1.0 mL | 5 mg/mL | 0.50 mL / 50 u | 1.00 mL / 100 u | — | — | — |
| 10 mg | 1.0 mL | 10 mg/mL | 0.25 mL / 25 u | 0.50 mL / 50 u | 0.75 mL / 75 u | 1.00 mL / 100 u | — |
| 10 mg | 2.0 mL | 5 mg/mL | 0.50 mL / 50 u | 1.00 mL / 100 u | — | — | — |
| 15 mg | 1.5 mL | 10 mg/mL | 0.25 mL / 25 u | 0.50 mL / 50 u | 0.75 mL / 75 u | 1.00 mL / 100 u | 1.50 mL / split |
| 40 mg | 2.0 mL | 20 mg/mL | 0.125 mL / 12.5 u | 0.25 mL / 25 u | 0.375 mL / 37.5 u | 0.50 mL / 50 u | 0.75 mL / 75 u |
| 40 mg | 3.0 mL | 13.33 mg/mL | 0.188 mL / 18.8 u | 0.375 mL / 37.5 u | 0.563 mL / 56.3 u | 0.75 mL / 75 u | 1.125 mL / split |
| 60 mg | 3.0 mL | 20 mg/mL | 0.125 mL / 12.5 u | 0.25 mL / 25 u | 0.375 mL / 37.5 u | 0.50 mL / 50 u | 0.75 mL / 75 u |
20 mg/mL keeps 40 mg and 60 mg vial setups within a 3 mL vial-capacity ceiling while keeping the listed doses compact.
- 01
Warm up
Let the tirzepatide vial and BAC water sit at room temperature for 5–10 minutes.
- 02
Clean the stoppers
Wipe both vial stoppers with alcohol swabs and let them air dry for 10–15 seconds.
- 03
Draw the BAC water
Using a sterile syringe, draw the calculated volume of BAC water (e.g., 2.0 mL for a 40 mg vial → 20 mg/mL).
- 04
Inject down the wall
Push the water slowly down the inside wall of the tirzepatide vial. Do not spray it directly onto the powder.
- 05
Swirl, do not shake
Gently swirl until fully dissolved (1–3 minutes). The solution should be clear, colorless to slightly yellow, with no visible particles.
- 06
Label
Write the peptide name, concentration (mg/mL), and reconstitution date on the vial.
- 07
Refrigerate
Store at 2–8 °C (35.6–46.4 °F) and use within 28 days.
Need a different ratio?
Use the PepPal reconstitution calculator for any vial-and-water pairing. Enter vial mg, water volume, and target dose to get exact syringe units.
Tirzepatide Dosage Chart
This tirzepatide dosage chart summarizes the standard once-weekly titration schedule from 2.5 mg up to 15 mg, with dose escalation shown by week range.
How Tirzepatide Works
Tirzepatide is a 39-amino-acid synthetic peptide with a fatty-acid attachment. The fatty acid is what lets it bind to blood proteins and stay in circulation long enough for once-weekly dosing — its half-life is roughly 5 days. Once in circulation, it activates two receptors that the gut normally talks to after a meal: GIP and GLP-1.
GIP pathway
Tirzepatide activates GIP (glucose-dependent insulinotropic polypeptide) receptors at full strength, comparable to natural GIP. This helps the pancreas release insulin in response to food, improves how the body processes fat, and sends appetite-reducing signals to brain regions that GLP-1-only drugs do not reach.
GLP-1 pathway
Tirzepatide activates GLP-1 (glucagon-like peptide-1) receptors at about one-fifth the potency of natural GLP-1. This slows gastric emptying (so meals feel filling for longer), helps the pancreas tune insulin release, and suppresses appetite through brain signaling.
Why the combination matters
Adding GIP activation is what separates tirzepatide from semaglutide. In the head-to-head SURMOUNT-5 trial (NEJM, 2025), tirzepatide produced −20.2% body weight loss vs −13.7% for semaglutide at 72 weeks, with similar side-effect profiles. The dual approach also improved insulin sensitivity beyond what GLP-1 monotherapy delivered in SURPASS-2.
Who Tirzepatide Is For and Who Should Avoid It
Tirzepatide is FDA-approved for specific patient groups. People who do not match those groups, or who match a contraindication, should not use it without close clinician oversight — and in some cases, should not use it at all.
Approved patient groups
FDA-approved indications (as of June 2026)
Brand
Mounjaro
Indication
Type 2 diabetes
Population
Adults whose blood sugar is not controlled by diet, exercise, or other medications.
Brand
Zepbound
Indication
Chronic weight management
Population
Adults with obesity (BMI ≥30) or overweight (BMI ≥27) plus at least one weight-related condition.
Brand
Zepbound
Indication
Obstructive sleep apnea
Population
Adults with moderate-to-severe OSA who also have obesity.
| Brand | Indication | Population |
|---|---|---|
| Mounjaro | Type 2 diabetes | Adults whose blood sugar is not controlled by diet, exercise, or other medications. |
| Zepbound | Chronic weight management | Adults with obesity (BMI ≥30) or overweight (BMI ≥27) plus at least one weight-related condition. |
| Zepbound | Obstructive sleep apnea | Adults with moderate-to-severe OSA who also have obesity. |
Who should not use tirzepatide
Personal or family history of medullary thyroid carcinoma (MTC) or MEN 2
Boxed warning. Rodent studies showed thyroid C-cell tumors. Tirzepatide is contraindicated in this group.
History of pancreatitis
Pancreatitis has been reported. Patients with prior episodes should avoid tirzepatide unless a clinician decides the benefit clearly outweighs the risk.
Pregnancy
Tirzepatide is not recommended during pregnancy. Animal data show potential fetal harm. Stop tirzepatide at least 2 months before a planned pregnancy because of the long half-life.
Severe gastrointestinal disease (gastroparesis, severe IBD)
Tirzepatide slows gastric emptying. Patients with pre-existing severe motility issues may experience worse symptoms.
Type 1 diabetes
Tirzepatide is not a substitute for insulin. It is not approved for type 1 diabetes or for diabetic ketoacidosis.
Children and adolescents
Safety and effectiveness in patients under 18 have not been established outside of trial settings.
People using oral contraceptives
Slowed gastric emptying can reduce oral contraceptive absorption when starting tirzepatide. Backup contraception is recommended for the first 4 weeks of dosing and after every dose increase.
Tirzepatide Side Effects & Safety
Most tirzepatide side effects are digestive: nausea, diarrhea, vomiting, reduced appetite, and indigestion. They are usually worst during the weeks when the dose goes up and improve once the body adjusts. Below are the rates reported across the SURPASS and SURMOUNT trial programs.
Common side effects (SURPASS meta-analysis and SURMOUNT-1 reporting)
Side effect
Nausea
Approx. rate on tirzepatide
17–22%
Pattern
Worst during dose escalation; improves at stable dose.
Side effect
Diarrhea
Approx. rate on tirzepatide
13–16%
Pattern
Mild to moderate; rarely leads to discontinuation.
Side effect
Vomiting
Approx. rate on tirzepatide
6–10%
Pattern
More common at 10 mg and 15 mg.
Side effect
Decreased appetite
Approx. rate on tirzepatide
7–9%
Pattern
Often reported as a desired effect for weight loss.
Side effect
Indigestion
Approx. rate on tirzepatide
~7%
Pattern
Often paired with slower digestion.
Side effect
Injection-site reactions
Approx. rate on tirzepatide
3–7%
Pattern
Redness, mild itching, or local irritation.
Side effect
Resting heart rate increase
Approx. rate on tirzepatide
+2–4 bpm
Pattern
Modest. Larger increases are uncommon.
| Side effect | Approx. rate on tirzepatide | Pattern |
|---|---|---|
| Nausea | 17–22% | Worst during dose escalation; improves at stable dose. |
| Diarrhea | 13–16% | Mild to moderate; rarely leads to discontinuation. |
| Vomiting | 6–10% | More common at 10 mg and 15 mg. |
| Decreased appetite | 7–9% | Often reported as a desired effect for weight loss. |
| Indigestion | ~7% | Often paired with slower digestion. |
| Injection-site reactions | 3–7% | Redness, mild itching, or local irritation. |
| Resting heart rate increase | +2–4 bpm | Modest. Larger increases are uncommon. |
Source: meta-analyses across SURPASS; SURMOUNT-1 (NEJM 2022). Rates differ by trial and dose.
Side effects by dose
A meta-analysis of 10 trials (6,836 participants) found total GI event rates of 39% at 5 mg, 46% at 10 mg, and 49% at 15 mg. Discontinuation due to side effects ran from about 5% at 5 mg to about 10% at 15 mg.
Serious risks and warnings
Boxed warning: thyroid C-cell tumors
Rodent studies showed dose-dependent C-cell tumors. The clinical relevance in humans is uncertain, but use is contraindicated in patients with MTC history or MEN 2.
Pancreatitis
Acute pancreatitis has been reported. Stop tirzepatide if pancreatitis is suspected (severe abdominal pain that radiates to the back).
Gallbladder disease
Cholelithiasis and cholecystitis have been reported, consistent with rapid weight loss generally.
Hypoglycemia
Tirzepatide alone rarely causes low blood sugar, but the risk rises sharply when combined with insulin or sulfonylureas. Dose adjustments to those drugs are usually needed.
Acute kidney injury
Severe nausea and vomiting can lead to dehydration and AKI. Stay hydrated, especially during dose escalation. For practical support, review hydration, smaller meals, and GLP-1 supplement basics.
Hypersensitivity
Anaphylaxis and angioedema have been reported. Discontinue if a serious allergic reaction occurs.
Tirzepatide Timeline & What to Monitor
Tirzepatide builds up gradually. Because the half-life is about 5 days and you dose weekly, blood levels rise for the first 4 weeks before stabilizing. That is also why each dose step lasts at least 4 weeks — anything sooner is judging the new dose before it has fully accumulated.
What people typically notice across the ladder
Timeframe
Week 1–2 (2.5 mg)
What is reported
Mild appetite reduction; some early nausea.
What the trials measured
Baseline labs; no efficacy endpoint expected.
Timeframe
Week 4–8 (2.5 → 5 mg)
What is reported
Steadier appetite suppression; first weight changes.
What the trials measured
Early HbA1c shift in T2D; modest weight loss in obesity arms.
Timeframe
Week 12–16 (5 → 10 mg)
What is reported
Most pronounced appetite and weight changes.
What the trials measured
Roughly 10–15% weight loss in obesity arms by week 24.
Timeframe
Week 24+ (10 → 15 mg)
What is reported
Weight loss plateaus or continues slowly.
What the trials measured
−21.4% (10 mg) and −22.5% (15 mg) at 72 weeks (SURMOUNT-1).
| Timeframe | What is reported | What the trials measured |
|---|---|---|
| Week 1–2 (2.5 mg) | Mild appetite reduction; some early nausea. | Baseline labs; no efficacy endpoint expected. |
| Week 4–8 (2.5 → 5 mg) | Steadier appetite suppression; first weight changes. | Early HbA1c shift in T2D; modest weight loss in obesity arms. |
| Week 12–16 (5 → 10 mg) | Most pronounced appetite and weight changes. | Roughly 10–15% weight loss in obesity arms by week 24. |
| Week 24+ (10 → 15 mg) | Weight loss plateaus or continues slowly. | −21.4% (10 mg) and −22.5% (15 mg) at 72 weeks (SURMOUNT-1). |
Numbers come from the SURMOUNT-1 trial and are population averages, not promises for any individual.
What is reasonable to monitor
Weight and waist circumference
Trial endpoints. Weekly weight and monthly waist measurements are simple at-home markers.
HbA1c (for T2D users)
Standard glycemic marker. SURPASS-2 showed up to −2.30% from baseline at 40 weeks.
Blood pressure
Tirzepatide modestly lowers systolic BP (~5 mmHg in SUMMIT). Patients on antihypertensives should track BP during escalation.
Resting heart rate
A 2–4 bpm rise is common. Larger sustained increases warrant a clinician check.
Symptoms of pancreatitis or gallbladder problems
Severe abdominal pain, back pain, fever, jaundice — stop and seek medical care.
Hydration and kidney symptoms
Especially during heavy nausea or vomiting.
Tirzepatide Clinical Evidence Context
Tirzepatide has one of the largest clinical trial programs of any incretin drug. The SURPASS program (type 2 diabetes) enrolled more than 19,000 participants across 10 trials. The SURMOUNT program (obesity) added thousands more, including the head-to-head SURMOUNT-5 trial against semaglutide. The summary below pulls the headline numbers from each pivotal study.
Pivotal Phase 3 trials
Trial
SURMOUNT-1 (NEJM 2022)
Population
2,539 adults, obesity, no diabetes; 72 weeks
Headline result
−22.5% body weight at 15 mg; −21.4% at 10 mg; −16.0% at 5 mg.
Trial
SURMOUNT-5 (NEJM 2025)
Population
751 adults, obesity, no diabetes; head-to-head vs semaglutide; 72 weeks
Headline result
Tirzepatide −20.2% vs semaglutide −13.7% (P<0.001).
Trial
SURPASS-2 (NEJM 2021)
Population
1,879 adults with T2D vs semaglutide 1 mg; 40 weeks
Headline result
All tirzepatide doses superior. HbA1c up to −2.30%; up to 92% reached HbA1c <7%.
Trial
SURPASS-1 (Lancet 2021)
Population
478 adults with T2D, monotherapy vs placebo; 40 weeks
Headline result
Up to 52% achieved HbA1c <5.7% (non-diabetic range).
Trial
SURPASS-5 (JAMA 2022)
Population
475 adults with T2D + insulin glargine; 40 weeks
Headline result
HbA1c −2.11% to −2.34%; weight loss 5.4–8.8 kg.
Trial
SUMMIT (NEJM 2024)
Population
731 patients with HFpEF + obesity; 104 weeks median
Headline result
38% reduction in CV death or worsening heart failure (HR 0.62).
Trial
SURMOUNT-OSA (NEJM 2024)
Population
469 adults with moderate-to-severe OSA + obesity; 52 weeks
Headline result
AHI reduced by 25.3–29.3 events/hour; weight loss ~45–50 lbs.
| Trial | Population | Headline result |
|---|---|---|
| SURMOUNT-1 (NEJM 2022) | 2,539 adults, obesity, no diabetes; 72 weeks | −22.5% body weight at 15 mg; −21.4% at 10 mg; −16.0% at 5 mg. |
| SURMOUNT-5 (NEJM 2025) | 751 adults, obesity, no diabetes; head-to-head vs semaglutide; 72 weeks | Tirzepatide −20.2% vs semaglutide −13.7% (P<0.001). |
| SURPASS-2 (NEJM 2021) | 1,879 adults with T2D vs semaglutide 1 mg; 40 weeks | All tirzepatide doses superior. HbA1c up to −2.30%; up to 92% reached HbA1c <7%. |
| SURPASS-1 (Lancet 2021) | 478 adults with T2D, monotherapy vs placebo; 40 weeks | Up to 52% achieved HbA1c <5.7% (non-diabetic range). |
| SURPASS-5 (JAMA 2022) | 475 adults with T2D + insulin glargine; 40 weeks | HbA1c −2.11% to −2.34%; weight loss 5.4–8.8 kg. |
| SUMMIT (NEJM 2024) | 731 patients with HFpEF + obesity; 104 weeks median | 38% reduction in CV death or worsening heart failure (HR 0.62). |
| SURMOUNT-OSA (NEJM 2024) | 469 adults with moderate-to-severe OSA + obesity; 52 weeks | AHI reduced by 25.3–29.3 events/hour; weight loss ~45–50 lbs. |
Cardiovascular outcomes trial SURPASS-CVOT (NCT04255433) is ongoing.
Strongest weight-loss evidence
SURMOUNT-1 and the head-to-head SURMOUNT-5 are the gold-standard data points for tirzepatide weight loss. Both are large, multicenter, randomized, placebo- or semaglutide-controlled.
Strongest glycemic evidence
SURPASS-2 is the most cited head-to-head against semaglutide for HbA1c reduction in type 2 diabetes.
Cardiovascular evidence
SUMMIT showed a 38% reduction in cardiovascular death or worsening heart failure in obese HFpEF patients. SURPASS-CVOT will broaden that picture.
Evidence gaps
Long-term (5+ year) outcomes data is still being collected. Post-discontinuation weight regain has been observed in trial extensions; tirzepatide is treated as a chronic therapy.
Tirzepatide Storage & Handling
Tirzepatide storage
State
Lyophilized (powder, sealed)
Storage
−4 °F (−20 °C) freezer
Duration
Long-term (12+ months).
State
Lyophilized (powder, sealed)
Storage
35.6–46.4 °F (2–8 °C) refrigerator
Duration
Several months.
State
Lyophilized (powder, sealed)
Storage
Room temperature, in transit
Duration
Stable for several weeks during shipping.
State
Reconstituted solution
Storage
35.6–46.4 °F (2–8 °C) refrigerator
Duration
Up to 28 days (conservative).
State
FDA pen (Mounjaro / Zepbound)
Storage
35.6–46.4 °F (2–8 °C); up to 21 days at room temperature
Duration
See the carton — most pens allow a single off-fridge window.
| State | Storage | Duration |
|---|---|---|
| Lyophilized (powder, sealed) | −4 °F (−20 °C) freezer | Long-term (12+ months). |
| Lyophilized (powder, sealed) | 35.6–46.4 °F (2–8 °C) refrigerator | Several months. |
| Lyophilized (powder, sealed) | Room temperature, in transit | Stable for several weeks during shipping. |
| Reconstituted solution | 35.6–46.4 °F (2–8 °C) refrigerator | Up to 28 days (conservative). |
| FDA pen (Mounjaro / Zepbound) | 35.6–46.4 °F (2–8 °C); up to 21 days at room temperature | See the carton — most pens allow a single off-fridge window. |
Do not freeze the reconstituted solution — freezing damages the peptide structure. Protect from light. Bacteriostatic water (0.9% benzyl alcohol) is preferred for multi-dose vials; sterile water only if the vial will be used in one session.
Tirzepatide Protocol Mistakes & Troubleshooting
- 01
Missed a weekly dose
If less than 4 days (96 hours) have passed, take the missed dose now and resume the regular weekly schedule. If more than 4 days have passed, skip it and take the next dose on the regular day. Do not double up.
- 02
Cloudy, particulate, or off-color vial
Reconstituted tirzepatide should be clear, colorless to slightly yellow, and free of visible particles. If the solution is cloudy or has floaters, do not inject. Discard and reconstitute a new vial.
- 03
Wrong BAC water volume
If you added more water than planned (e.g., 3 mL into a 40 mg vial instead of 2 mL), recalculate the new concentration (in this case 13.33 mg/mL) and adjust the syringe units. Use the PepPal calculator. The drug is not ruined; the math just changes.
- 04
Severe nausea on a new dose
Hold at the current dose for an additional 4 weeks before re-attempting escalation. Trial protocols allowed exactly this. Hydration, smaller meals, and avoiding fatty/spicy foods help most users.
- 05
Injection-site lump or redness
Rotate sites between abdomen, thigh, and upper arm. Don't reuse the same spot two weeks in a row. Persistent or worsening reactions warrant a clinician check.
- 06
Vial left at room temperature
Sealed lyophilized vials tolerate short-term room temperature exposure. Reconstituted solution at room temperature for less than 24 hours is generally usable; any longer, discard.
- 07
Confused about Mounjaro vs Zepbound dose
The titration ladder (2.5 → 5 → 7.5 → 10 → 12.5 → 15 mg weekly) is identical between the two brands. The label, indication, and packaging differ; the dose math does not.
- 08
Severe abdominal pain, jaundice, or unrelenting vomiting
Stop the next dose and seek qualified medical care. These symptoms can signal pancreatitis, gallbladder disease, or dehydration-driven kidney injury.
Tirzepatide Regulatory Status
As of June 2026, tirzepatide is FDA-approved under two brand names. Mounjaro received FDA approval in May 2022 for adults with type 2 diabetes. Zepbound received approval in November 2023 for chronic weight management in adults with obesity or overweight plus a weight-related condition, and in December 2024 for moderate-to-severe obstructive sleep apnea in adults with obesity. Tirzepatide is the first and only FDA-approved dual GIP/GLP-1 receptor agonist.
Branded supply
Mounjaro and Zepbound are sold as single-use auto-injector pens (and Zepbound vials) by Eli Lilly. These are FDA-approved finished drug products.
Compounded supply
Compounded tirzepatide was widely available during the FDA-recognized shortage that ended in late 2024. Outside an active shortage, large-scale compounding is restricted; access depends on state pharmacy rules and 503A/503B compounding pathways. Quality and concentration vary by compounder.
Research-grade vials
Lyophilized research-grade tirzepatide is sold by laboratory chemical suppliers in 5/10/15/40/60 mg vials, labeled for research use only and not for human consumption. This is a separate, non-FDA supply chain.
Oral tirzepatide
There is no FDA-approved oral tirzepatide as of June 2026. "Tirzepatide pills" or "tirzepatide tablets" sold online are not FDA-approved formulations and lack established bioavailability data.
International status
Tirzepatide is approved in the EU, UK, Japan, and other markets under the Mounjaro and Zepbound names. The UK BNF lists it for both T2D and weight management.
Tirzepatide vs Semaglutide vs Retatrutide
Three incretin-class compounds dominate the conversation: tirzepatide (dual GIP/GLP-1), semaglutide (GLP-1 only, sold as Ozempic and Wegovy), and retatrutide (triple agonist GLP-1 + GIP + glucagon, still investigational). The table below puts them side by side on the points that matter most to dosing decisions.
Side-by-side compound comparison
Receptor targets
Tirzepatide
GLP-1 + GIP (dual)
Semaglutide
GLP-1 only
Retatrutide
GLP-1 + GIP + Glucagon (triple)
Half-life
Tirzepatide
~5 days
Semaglutide
~7 days
Retatrutide
~6 days
Dosing frequency
Tirzepatide
Once weekly
Semaglutide
Once weekly
Retatrutide
Once weekly
Max studied dose
Tirzepatide
15 mg / week
Semaglutide
2.4 mg / week (Wegovy)
Retatrutide
12 mg / week
Peak weight loss
Tirzepatide
−22.5% (SURMOUNT-1, 72 wk)
Semaglutide
−15.8% (STEP-1, 68 wk)
Retatrutide
−24.2% (Phase 2, 48 wk)
FDA status (June 2026)
Tirzepatide
Approved (T2D, obesity, OSA)
Semaglutide
Approved (T2D, obesity, CV risk)
Retatrutide
Investigational — Phase 3
Head-to-head
Tirzepatide
−20.2% vs semaglutide −13.7% (SURMOUNT-5)
Semaglutide
—
Retatrutide
Not yet head-to-head vs tirzepatide
HFpEF benefit
Tirzepatide
Yes (SUMMIT, HR 0.62)
Semaglutide
Yes (STEP-HFpEF)
Retatrutide
Not yet studied
Unique advantage
Tirzepatide
Best-in-class FDA-approved efficacy; 3 indications
Semaglutide
Longest track record; CV outcomes data
Retatrutide
Highest weight loss in early data
| Tirzepatide | Semaglutide | Retatrutide | |
|---|---|---|---|
| Receptor targets | GLP-1 + GIP (dual) | GLP-1 only | GLP-1 + GIP + Glucagon (triple) |
| Half-life | ~5 days | ~7 days | ~6 days |
| Dosing frequency | Once weekly | Once weekly | Once weekly |
| Max studied dose | 15 mg / week | 2.4 mg / week (Wegovy) | 12 mg / week |
| Peak weight loss | −22.5% (SURMOUNT-1, 72 wk) | −15.8% (STEP-1, 68 wk) | −24.2% (Phase 2, 48 wk) |
| FDA status (June 2026) | Approved (T2D, obesity, OSA) | Approved (T2D, obesity, CV risk) | Investigational — Phase 3 |
| Head-to-head | −20.2% vs semaglutide −13.7% (SURMOUNT-5) | — | Not yet head-to-head vs tirzepatide |
| HFpEF benefit | Yes (SUMMIT, HR 0.62) | Yes (STEP-HFpEF) | Not yet studied |
| Unique advantage | Best-in-class FDA-approved efficacy; 3 indications | Longest track record; CV outcomes data | Highest weight loss in early data |
These compounds are not interchangeable. Reconstitution math, dose ranges, and concentration targets differ.
For an oral, non-incretin alternative, see the tesofensine protocol. For dedicated guides, see the semaglutide protocol and retatrutide protocol.
Tirzepatide Blood Tests & Monitoring
Tirzepatide is an approved GIP/GLP-1 receptor agonist used in diabetes and weight-management contexts. Monitoring focuses on glucose control, kidney context, lipids, GI symptoms, gallbladder/pancreas symptoms, and thyroid-history cautions.
Blood test markers to discuss with a clinician
Marker
A1c
Why it matters
Shows longer-term glucose control and helps track metabolic response over time.
Timing
Baseline
Marker
Fasting glucose
Why it matters
Gives a current glucose snapshot, especially when appetite and diabetes medication needs change.
Timing
Follow-up
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews kidney function, liver enzymes, electrolytes, and glucose, which matter with GI symptoms or dehydration.
Timing
Baseline
Marker
Lipid panel
Why it matters
Tracks cardiometabolic changes during weight-loss or diabetes-management phases.
Timing
Follow-up
Marker
Blood pressure and resting heart rate
Why it matters
Adds cardiovascular context during weight loss, medication changes, and hydration shifts.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| A1c | Shows longer-term glucose control and helps track metabolic response over time. | Baseline |
| Fasting glucose | Gives a current glucose snapshot, especially when appetite and diabetes medication needs change. | Follow-up |
| Comprehensive metabolic panel (CMP) | Reviews kidney function, liver enzymes, electrolytes, and glucose, which matter with GI symptoms or dehydration. | Baseline |
| Lipid panel | Tracks cardiometabolic changes during weight-loss or diabetes-management phases. | Follow-up |
| Blood pressure and resting heart rate | Adds cardiovascular context during weight loss, medication changes, and hydration shifts. | Optional |
Monitoring guidance is label-informed for tirzepatide and supported by incretin-class clinical monitoring considerations.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting or changing dose, especially with diabetes, kidney disease, pancreatitis history, gallbladder history, thyroid cancer history, or major calorie restriction.
Follow-up
Repeat glucose and CMP-related markers after 4-12 weeks or sooner if vomiting, dehydration, or glucose symptoms occur.
Longer term
For ongoing use, review metabolic and kidney trends every 3-6 months with a clinician.
How to interpret the labs
- Diabetes medications may need clinician review if glucose drops with reduced intake.
- Severe abdominal pain, gallbladder symptoms, and persistent vomiting require symptom-based review.
- Personal or family history of medullary thyroid carcinoma or MEN2 is an important label-based caution.
Do not wait for routine labs
Severe abdominal pain, persistent vomiting, signs of dehydration, fainting, allergic symptoms, or severe low-glucose symptoms need medical review. A neck mass, trouble swallowing, or persistent hoarseness should be discussed with a clinician.
FAQ
Q1: What is the starting dose of tirzepatide?
The starting dose is 2.5 mg once weekly via subcutaneous injection for the first 4 weeks. This is a tolerability dose, not a treatment dose for weight loss or HbA1c. After 4 weeks the dose escalates to 5 mg, the first true maintenance dose. Further escalation occurs in 2.5 mg increments at minimum 4-week intervals up to 15 mg weekly, based on individual tolerance.
Q2: What is the highest dose of tirzepatide / Zepbound?
The maximum FDA-approved dose is 15 mg once weekly for both Mounjaro and Zepbound. This is also the highest dose that was studied in the SURPASS and SURMOUNT trials. In SURMOUNT-1 the 15 mg arm averaged −22.5% body weight loss at 72 weeks, only modestly higher than the 10 mg arm at −21.4%. Many users do well at 10 mg without escalating further.
Q3: What is tirzepatide's half-life?
Tirzepatide's half-life is approximately 5 days (about 120 hours). This is what supports once-weekly dosing. With weekly injections, blood levels build up over about 4 weeks before reaching steady state at roughly 1.6× a single dose. That is why each ladder step lasts at least 4 weeks — the body needs that time to fully adjust.
Q4: How do you convert tirzepatide mg to insulin units?
Insulin syringes use U-100 markings, where 1 mL = 100 units. The conversion depends on the concentration after reconstitution. The cleanest setup is a 40 mg vial with 2.0 mL BAC water, giving 20 mg/mL. At that concentration: 2.5 mg = 12.5 units, 5 mg = 25 units, 7.5 mg = 37.5 units, 10 mg = 50 units, 12.5 mg = 62.5 units, 15 mg = 75 units. For any other vial-and-water pairing, use the PepPal calculator.
Q5: How much weight can you lose on tirzepatide?
In SURMOUNT-1 (NEJM 2022, 2,539 adults with obesity), the 15 mg arm averaged −22.5% body weight loss at 72 weeks, the 10 mg arm −21.4%, and the 5 mg arm −16.0%. In the head-to-head SURMOUNT-5 trial (NEJM 2025), tirzepatide produced −20.2% weight loss vs −13.7% for semaglutide. These are population averages over 72 weeks, not promises for any individual.
Q6: How do you reconstitute tirzepatide?
For a 40 mg lyophilized vial, add 2.0 mL of bacteriostatic water for a 20 mg/mL solution. Inject the water slowly down the inside vial wall, swirl gently (do not shake), and refrigerate at 2–8 °C. Use within 28 days. For other vial sizes, see the reconstitution table above or use the PepPal calculator.
Q7: Is tirzepatide FDA-approved?
Yes. Mounjaro was FDA-approved in May 2022 for type 2 diabetes. Zepbound was approved in November 2023 for chronic weight management and in December 2024 for moderate-to-severe obstructive sleep apnea with obesity. Tirzepatide is the first and only FDA-approved dual GIP/GLP-1 receptor agonist.
Q8: What is the difference between Mounjaro and Zepbound?
Mounjaro and Zepbound contain the same active drug, tirzepatide, in the same titration ladder. The only differences are the indication on the label and the packaging. Mounjaro is approved for type 2 diabetes. Zepbound is approved for obesity and for OSA with obesity. The dose schedule (2.5 → 5 → 7.5 → 10 → 12.5 → 15 mg weekly) is identical.
Q9: What are the most common tirzepatide side effects?
Gastrointestinal effects dominate: nausea (17–22%), diarrhea (13–16%), vomiting (6–10%), decreased appetite (7–9%), and indigestion (~7%). Most are mild to moderate, hit hardest during dose escalation, and improve at stable doses. Discontinuation due to side effects ranged from ~5% at 5 mg to ~10% at 15 mg in trials. Tirzepatide also carries a boxed warning for thyroid C-cell tumors and is contraindicated with MTC or MEN 2 history.
Q10: How does tirzepatide compare to semaglutide?
Tirzepatide is a dual GIP/GLP-1 agonist; semaglutide activates GLP-1 only. In the head-to-head SURMOUNT-5 trial (NEJM 2025), tirzepatide produced −20.2% weight loss vs −13.7% for semaglutide at 72 weeks. In SURPASS-2 (T2D), all tirzepatide doses showed superior HbA1c and weight reductions vs semaglutide 1 mg. GI side-effect profiles were broadly similar.
Q11: What if I miss a tirzepatide dose?
Per the Mounjaro and Zepbound prescribing information, take the missed dose as soon as possible if it is within 4 days (96 hours). After that window, skip it and resume on the next regularly scheduled day. Do not double up. The day of the week can be changed as long as the last dose was at least 3 days earlier.
Q12: Who should not take tirzepatide?
Avoid tirzepatide if you have a personal or family history of medullary thyroid carcinoma or MEN 2 (boxed warning), a history of pancreatitis, severe gastrointestinal motility disease, or known hypersensitivity to tirzepatide. It is not recommended in pregnancy and is not a substitute for insulin in type 1 diabetes. Stop at least 2 months before a planned pregnancy because of the long half-life.
Q13: What vial sizes are available for research-grade tirzepatide?
Research-grade lyophilized tirzepatide is commonly sold in 5 mg, 10 mg, 15 mg, 40 mg, and 60 mg vials. The 40 mg vial is the most popular because it covers the full 2.5–10 mg ladder with compact math when reconstituted with 2.0 mL of BAC water (20 mg/mL).
Q14: How is reconstituted tirzepatide stored?
Store the reconstituted solution in the refrigerator at 2–8 °C (35.6–46.4 °F) and use within 28 days. Do not freeze it — freezing damages the peptide. Protect from light. Use bacteriostatic water (0.9% benzyl alcohol) for multi-dose vials; sterile water only if the entire vial will be used in one session.
Q15: Is compounded tirzepatide the same as branded Mounjaro or Zepbound?
Compounded tirzepatide is a tirzepatide product mixed by a compounding pharmacy, not the FDA-approved Lilly pen. During the 2023–2024 shortage, large-scale compounding was permitted; outside that shortage, access is restricted and depends on state and federal compounding rules. Compounded products vary in concentration, formulation, and quality. They are not bioequivalent to Mounjaro or Zepbound by FDA standards.
Q16: Can tirzepatide be taken orally?
Not currently. As of June 2026 there is no FDA-approved oral tirzepatide. Oral incretin therapies do exist for semaglutide (Rybelsus), but tirzepatide is only FDA-approved as a subcutaneous injection. "Tirzepatide tablets" sold online are not FDA-approved formulations.
Sources & Research
- 1. Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity (SURMOUNT-1). New England Journal of Medicine (2022)
- 2. Aronne LJ, Horn DB, le Roux CW, et al. Tirzepatide as Compared with Semaglutide for the Treatment of Obesity (SURMOUNT-5). New England Journal of Medicine (2025)
- 3. Frias JP, Davies MJ, Rosenstock J, et al. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes (SURPASS-2). New England Journal of Medicine (2021)
- 4. Rosenstock J, Wysham C, Frias JP, et al. Efficacy and safety of a novel dual GIP and GLP-1 receptor agonist tirzepatide in patients with type 2 diabetes (SURPASS-1). Lancet (2021)
- 5. Dahl D, Onishi Y, Norwood P, et al. Effect of Subcutaneous Tirzepatide vs Placebo Added to Titrated Insulin Glargine on Glycemic Control in Patients With Type 2 Diabetes (SURPASS-5). JAMA (2022)
- 6. Packer M, Zile MR, Kramer CM, et al. Tirzepatide for Heart Failure with Preserved Ejection Fraction and Obesity (SUMMIT). New England Journal of Medicine (2024)
- 7. Malhotra A, Grunstein RR, Fietze I, et al. Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity (SURMOUNT-OSA). New England Journal of Medicine (2024)
- 8. U.S. Food and Drug Administration Mounjaro (tirzepatide) injection — Prescribing Information and Approval History. FDA Drug Approvals (2022)
- 9. U.S. Food and Drug Administration Zepbound (tirzepatide) injection — Prescribing Information and Approval History. FDA Drug Approvals (2023)
- 10. Sinha R, Papamargaritis D, Sargeant JA, Davies MJ. Efficacy and Safety of Tirzepatide in Type 2 Diabetes and Obesity Management (meta-analysis of SURPASS). Journal of Obesity & Metabolic Syndrome (2023)
- 11. Coskun T, Sloop KW, Loghin C, et al. LY3298176, a novel dual GIP and GLP-1 receptor agonist for the treatment of type 2 diabetes mellitus: From discovery to clinical proof of concept. Molecular Metabolism (2018)
- 12. ClinicalTrials.gov A Study of Tirzepatide (LY3298176) on Cardiovascular Events in Participants With Type 2 Diabetes (SURPASS-CVOT, NCT04255433). ClinicalTrials.gov (2026)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: July 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page