Retatrutide + MOTS-c Quick Start
The retatrutide + MOTS-c stack pairs two research compounds that work on very different parts of fat metabolism. Retatrutide is Eli Lilly's investigational triple-receptor agonist - one weekly injection that acts on GLP-1, GIP, and glucagon receptors at once to cut appetite, improve insulin signaling, and raise energy use. MOTS-c is a small 16-amino-acid peptide encoded inside your own mitochondrial DNA. It is added to support what happens inside your cells while retatrutide drives the calorie deficit.
The community calls this combo a few different names: the Metabolic Super Stack, the Elite Metabolic Stack, or just reta + MOTS-c. They all mean the same two-compound protocol. This page covers what the stack is, how researchers usually schedule it, the reconstitution math for both vials, what to watch for, and how it compares to other retatrutide pairings.
Format
Separate vials only. There is no commercial pre-blended retatrutide + MOTS-c product.
Schedule
Retatrutide once weekly. MOTS-c 2-3x weekly (intermittent) or low-dose daily.
Easy measuring
Both vials use U-100 insulin syringes for typical research doses.
Sequencing
Run retatrutide alone for the first 4 weeks. Add MOTS-c at Week 5 once tolerance is set.
Research status
Reta is Phase 3 investigational. MOTS-c is research-only and WADA-prohibited.
Need broader context on combining peptides? See PepPal's stacking safety guide. For supplier and quality-control sourcing, see the PepPal supplier directory.
Disclaimer
This page is an educational research reference. It is not medical advice. No published human trial has tested retatrutide and MOTS-c together. The dosing structure below is built from each compound's own research and community practitioner reports. Retatrutide is a Phase 3 investigational compound. MOTS-c is an unregulated research compound and WADA-prohibited.
What Is the Retatrutide + MOTS-c Stack?
The retatrutide + MOTS-c stack is a two-compound research protocol. It pairs a top-of-class metabolic peptide with a much smaller peptide that targets the cellular layer of fat burning. The plain-English version: retatrutide tells your body to release fat from storage and to want less food. MOTS-c helps your cells actually burn the fat that retatrutide is releasing.
Researchers reach for this combination when the goal is not just appetite control but metabolic efficiency during a hard fat-loss phase. The simpler comparison is the cagrilintide + retatrutide stack, which adds extra satiety. The more complex one is the Advanced Recomp Stack, which layers in a growth-hormone secretagogue for lean mass.
What Each Compound Does
Retatrutide (LY3437943) is a once-weekly triple agonist. It hits three receptors at once: GLP-1 (cuts appetite, slows stomach), GIP (improves insulin signaling), and glucagon (raises energy expenditure and fat mobilization). In the Phase 3 TRIUMPH-4 trial, retatrutide at 12 mg produced 28.7% body weight loss at 68 weeks vs 2.1% for placebo.
MOTS-c is a 16-amino-acid mitochondrial-derived peptide. It activates AMPK - the cellular energy sensor that flips muscle cells from preferring glucose to preferring fat as fuel. AMPK is the same pathway activated by exercise and metformin. MOTS-c has no completed native-peptide human efficacy trial. The closest human data is from CB4211, an analog that completed Phase 1a/1b safety testing.
Why People Pair Them
Retatrutide is one of the most powerful metabolic compounds ever tested in humans, but it acts on systemic hormones. It does not reach inside your skeletal muscle cells to tell mitochondria what to burn. MOTS-c is added to fill that specific gap. The combined logic is:
- Fat mobilization (retatrutide) → mitochondrial fat oxidation (MOTS-c via AMPK). Released fat actually gets burned instead of re-stored.
- Insulin signaling at the islet (retatrutide GIP) → muscle glucose uptake (MOTS-c). Two different layers of the same insulin pathway.
- Reduced myostatin signaling in preclinical MOTS-c work. The mechanistic case for some lean-mass protection during a deep deficit.
- Exercise-mimetic effects of MOTS-c help with training capacity when retatrutide-driven fatigue is highest.
Evidence boundary
No clinical trial has tested retatrutide and MOTS-c as a combination. The pairing logic above is mechanistic and community-derived. Each compound has its own evidence base; the combination's evidence is theoretical.
Retatrutide + MOTS-c Dosing Protocol & Schedule
Evidence-level notice
No clinical trial has tested retatrutide + MOTS-c together. Retatrutide dosing comes from the Phase 3 TRIUMPH program titration. MOTS-c dosing comes from preclinical work, the CB4211 analog Phase 1 trial, and community practitioner reports.
There is no pre-blended retatrutide + MOTS-c vial on the market as of June 2026. The two compounds have very different stability windows once reconstituted, so they are dosed from separate vials. Both compounds are subcutaneous only - no oral or sublingual options.
Sequencing - Do Not Start Both on Day One
The most consistent recommendation across community protocols is to run retatrutide alone for the first 4 weeks at 1 mg weekly, confirm GI tolerance, then add MOTS-c at Week 5. Retatrutide's glucagon arm produces more nausea than pure GLP-1 compounds, so stabilizing it first makes it much easier to tell where any new symptom is coming from.
Separate-vial workflow
Independent Dose Control - Two Vials, Two Schedules
Retatrutide is titrated up in 4-week steps. MOTS-c is added at Week 5 with two common approaches: intermittent (most common) or low-dose daily.
Injection burden
1-2 injections per day on overlap days
Best for
Metabolic + mitochondrial pairing
Cycle driver
Retatrutide titration sets the pace
Retatrutide
- Loading
- 1 → 2 → 4 → 6 → 9 mg (every 4 weeks)
- Frequency
- Once weekly
- Maintenance
- 9 mg or 12 mg weekly
- Route
- SubQ
MOTS-c (intermittent - most common)
- Loading
- Start Week 5: 5 mg, 2x weekly
- Frequency
- 2-3x weekly
- Maintenance
- 5-10 mg, 2-3x weekly
- Route
- SubQ
MOTS-c (low-dose daily - alternative)
- Loading
- Start Week 5: 200 mcg/day, +200 mcg every 2 weeks
- Frequency
- Daily
- Maintenance
- Up to 1 mg daily
- Route
- SubQ
Weekly Schedule Example - Intermittent MOTS-c (Weeks 5-16)
Monday
Retatrutide 2 mg (morning) + MOTS-c 5 mg (pre-training)
Tuesday
Rest day
Wednesday
MOTS-c 5 mg (pre-training)
Thursday
Rest day
Friday
MOTS-c 5 mg (pre-training)
Saturday
Rest day
Sunday
Rest day
Inject the two compounds at different sites when dosing on the same day. Use separate syringes. Many community protocols dose MOTS-c on Mon/Wed/Fri because it lines up with a typical training split, and MOTS-c is exercise-inducible in animal studies.
Cycle Guidelines
Common Retatrutide + MOTS-c Cycle Approaches
Approach
Conservative starter
Duration
Reta weeks 1-24 (titrate to 4-6 mg max)
MOTS-c Pattern
MOTS-c only weeks 5-12, then off
Best For
First-time stack users, metabolic concerns
Approach
Standard research cycle
Duration
Reta weeks 1-48 (target 9 mg)
MOTS-c Pattern
MOTS-c 8-week pulses with 4-week breaks
Best For
Most community protocols
Approach
Aggressive deficit
Duration
Reta weeks 1-68 (target 12 mg)
MOTS-c Pattern
MOTS-c 6 weeks on / 2 weeks off, repeating
Best For
Advanced subjects with established tolerance
| Approach | Duration | MOTS-c Pattern | Best For |
|---|---|---|---|
| Conservative starter | Reta weeks 1-24 (titrate to 4-6 mg max) | MOTS-c only weeks 5-12, then off | First-time stack users, metabolic concerns |
| Standard research cycle | Reta weeks 1-48 (target 9 mg) | MOTS-c 8-week pulses with 4-week breaks | Most community protocols |
| Aggressive deficit | Reta weeks 1-68 (target 12 mg) | MOTS-c 6 weeks on / 2 weeks off, repeating | Advanced subjects with established tolerance |
Retatrutide is run open-ended in clinical trials (TRIUMPH-4 lasted 68 weeks). Most community protocols pair MOTS-c in pulses inside the reta cycle. Taper retatrutide rather than stopping it abruptly.
Protocol Notes
- Injection sites: Retatrutide is once-weekly so it can take a fixed day. Rotate MOTS-c sites across abdomen, thigh, and flank to avoid local irritation.
- No oral options: Both compounds are subcutaneous only. Do not try oral or sublingual use.
- Why MOTS-c on training days: MOTS-c is exercise-inducible in animal studies, and timing it before training is the most common community pattern. Animal data show enhanced metabolic adaptation when MOTS-c is dosed before exercise.
- AMPK stacking caution: MOTS-c activates AMPK. Metformin and berberine also activate AMPK through different paths. Combining them can lower blood glucose more than expected. Test glucose response carefully in the early weeks if you use any of those.
- GI tolerance first: Retatrutide TRIUMPH-4 reported nausea in 38.1% (9 mg) and 43.2% (12 mg) of participants. Do not push both compounds upward at the same time. Step retatrutide first, stabilize, then add MOTS-c.
- Syringe choice: U-100 insulin syringes work for both. Use 0.3 mL syringes with half-unit gradations for retatrutide doses below 1 mg from concentrated vials.
Retatrutide + MOTS-c Supplies Needed
Plan based on the separate-vial schedule above. Retatrutide is one injection per week. MOTS-c (intermittent) is 2-3 injections per week starting Week 5. Round up to leave a margin for priming losses and dropped syringes.
Recommended USA Supply
Use discount code SAVE10 at Peptira checkout. See why we love Peptira.

Retatrutide

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Retatrutide Vials
Once-weekly dosing, titrated upward. A 10 mg vial typically covers 2-5 weeks depending on the dose step.
| Cycle length | Planning note |
|---|---|
16 weeks (titration phase) 2-3 x 10 mg vials | 1 mg → 2 mg → 4 mg → 6 mg → 9 mg across 16 weeks; ~22 mg total used. |
24 weeks (conservative cycle) 3-4 x 10 mg vials | Adds 8 more weekly doses at the maintenance step. |
48 weeks (standard cycle) 6-8 x 10 mg vials | Maintenance at 9 mg weekly drives most of the total. |
68 weeks (aggressive) 9-12 x 10 mg vials | Maintenance at 12 mg weekly. Consider 20 mg or 30 mg vials for value. |
16 weeks (titration phase)
2-3 x 10 mg vials
1 mg → 2 mg → 4 mg → 6 mg → 9 mg across 16 weeks; ~22 mg total used.
24 weeks (conservative cycle)
3-4 x 10 mg vials
Adds 8 more weekly doses at the maintenance step.
48 weeks (standard cycle)
6-8 x 10 mg vials
Maintenance at 9 mg weekly drives most of the total.
68 weeks (aggressive)
9-12 x 10 mg vials
Maintenance at 12 mg weekly. Consider 20 mg or 30 mg vials for value.
MOTS-c Vials
Intermittent protocol: 5 mg per injection, 2-3x weekly. MOTS-c is reconstituted-stable for only ~7 days at 2-8 °C, so plan vial sizes around use rate.
| Cycle length | Planning note |
|---|---|
8 weeks MOTS-c pulse 2-3 x 10 mg vials | ~16-24 injections of 5 mg; 10 mg vial covers 2 injections. |
12 weeks MOTS-c pulse 3-4 x 10 mg vials | ~24-36 injections of 5 mg. |
Continuous MOTS-c (advanced) 5+ x 10 mg vials per cycle phase | Plan around the 7-day reconstituted window; aliquot or use smaller volumes. |
8 weeks MOTS-c pulse
2-3 x 10 mg vials
~16-24 injections of 5 mg; 10 mg vial covers 2 injections.
12 weeks MOTS-c pulse
3-4 x 10 mg vials
~24-36 injections of 5 mg.
Continuous MOTS-c (advanced)
5+ x 10 mg vials per cycle phase
Plan around the 7-day reconstituted window; aliquot or use smaller volumes.
Insulin Syringes (U-100)
Use 0.3 mL / 30-unit syringes for small draws (low-dose reta, low-dose MOTS-c). Use 1 mL syringes for larger volumes.
| Cycle length | Planning note |
|---|---|
16 weeks (reta only first 4 weeks) ~40 syringes | 1 reta/week + ~2 MOTS-c/week from Week 5 onward. |
24 weeks ~60 syringes | 1 reta/week + intermittent MOTS-c pulses. |
48 weeks ~120 syringes | Buy in bulk; 1 syringe per injection. |
16 weeks (reta only first 4 weeks)
~40 syringes
1 reta/week + ~2 MOTS-c/week from Week 5 onward.
24 weeks
~60 syringes
1 reta/week + intermittent MOTS-c pulses.
48 weeks
~120 syringes
Buy in bulk; 1 syringe per injection.
Bacteriostatic Water
Each compound is reconstituted separately. Plan around MOTS-c's shorter reconstituted window.
| Cycle length | Planning note |
|---|---|
16 weeks 1-2 x 10 mL bottles | ~3-6 mL used across reta + MOTS-c reconstitutions. |
24 weeks 2 x 10 mL bottles | Two bottles give margin for re-reconstituting MOTS-c. |
48 weeks 3-4 x 10 mL bottles | MOTS-c is reconstituted multiple times across the cycle. |
16 weeks
1-2 x 10 mL bottles
~3-6 mL used across reta + MOTS-c reconstitutions.
24 weeks
2 x 10 mL bottles
Two bottles give margin for re-reconstituting MOTS-c.
48 weeks
3-4 x 10 mL bottles
MOTS-c is reconstituted multiple times across the cycle.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments. MOTS-c's 7-day reconstituted window is the limiting factor - plan vial sizes around how much you can use in a week.
Companion Supplies & Routine Support
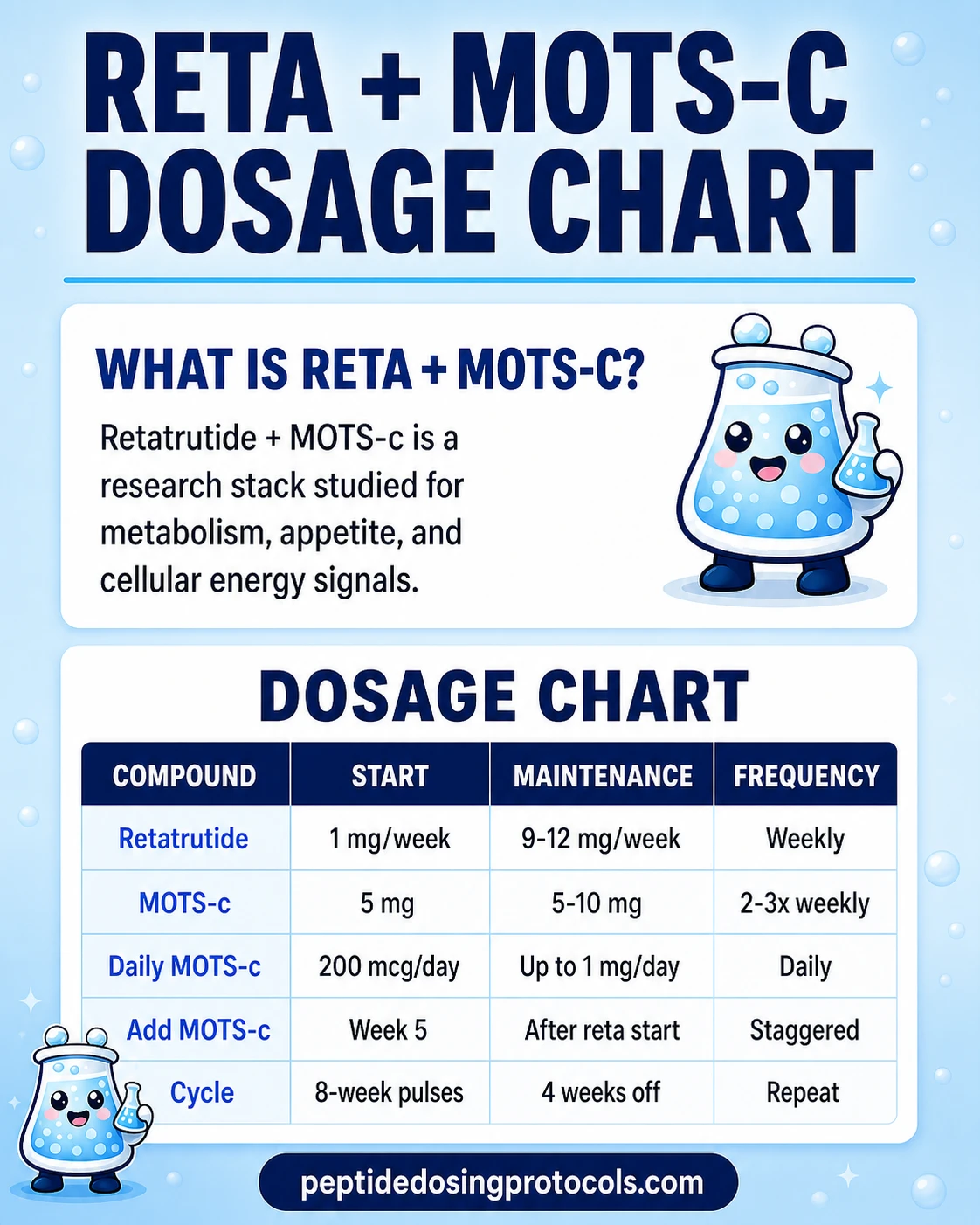
Retatrutide + MOTS-c Dosage Chart
This Retatrutide + MOTS-c dosage chart summarizes the retatrutide weekly titration and MOTS-c pulse dosing patterns shown in the dosing section above.
Retatrutide + MOTS-c Reconstitution Guide
Each compound is reconstituted on its own. The math below mirrors the Retatrutide protocol page and the MOTS-c protocol page so the numbers match across the site.
Label every vial
Both compounds use U-100 insulin syringes. A draw error matters - 0.2 mL at retatrutide 10 mg/mL is 2 mg of retatrutide. The same volume at MOTS-c 10 mg/mL is 2 mg of MOTS-c. Concentration changes everything. Label each vial with the compound name, concentration, and date.
Retatrutide Reconstitution Math
Retatrutide - mg per dose at common vial sizes
Vial Size
5 mg
BAC Water
1.0 mL
Concentration
5 mg/mL
2 mg Dose
0.40 mL (40 units)
4 mg Dose
0.80 mL (80 units)
6 mg Dose
N/A
9 mg Dose
N/A
Vial Size
10 mg
BAC Water
1.0 mL
Concentration
10 mg/mL
2 mg Dose
0.20 mL (20 units)
4 mg Dose
0.40 mL (40 units)
6 mg Dose
0.60 mL (60 units)
9 mg Dose
0.90 mL (90 units)
Vial Size
10 mg
BAC Water
2.0 mL
Concentration
5 mg/mL
2 mg Dose
0.40 mL (40 units)
4 mg Dose
0.80 mL (80 units)
6 mg Dose
1.20 mL (120 units*)
9 mg Dose
1.80 mL (180 units*)
Vial Size
20 mg
BAC Water
2.0 mL
Concentration
10 mg/mL
2 mg Dose
0.20 mL (20 units)
4 mg Dose
0.40 mL (40 units)
6 mg Dose
0.60 mL (60 units)
9 mg Dose
0.90 mL (90 units)
Vial Size
30 mg
BAC Water
3.0 mL
Concentration
10 mg/mL
2 mg Dose
0.20 mL (20 units)
4 mg Dose
0.40 mL (40 units)
6 mg Dose
0.60 mL (60 units)
9 mg Dose
0.90 mL (90 units)
| Vial Size | BAC Water | Concentration | 2 mg Dose | 4 mg Dose | 6 mg Dose | 9 mg Dose |
|---|---|---|---|---|---|---|
| 5 mg | 1.0 mL | 5 mg/mL | 0.40 mL (40 units) | 0.80 mL (80 units) | N/A | N/A |
| 10 mg | 1.0 mL | 10 mg/mL | 0.20 mL (20 units) | 0.40 mL (40 units) | 0.60 mL (60 units) | 0.90 mL (90 units) |
| 10 mg | 2.0 mL | 5 mg/mL | 0.40 mL (40 units) | 0.80 mL (80 units) | 1.20 mL (120 units*) | 1.80 mL (180 units*) |
| 20 mg | 2.0 mL | 10 mg/mL | 0.20 mL (20 units) | 0.40 mL (40 units) | 0.60 mL (60 units) | 0.90 mL (90 units) |
| 30 mg | 3.0 mL | 10 mg/mL | 0.20 mL (20 units) | 0.40 mL (40 units) | 0.60 mL (60 units) | 0.90 mL (90 units) |
* Volume above 100 units exceeds a standard 1 mL insulin syringe - split into two injections or use a larger syringe.
MOTS-c Reconstitution Math
MOTS-c - common doses at common vial sizes
Vial Size
5 mg
BAC Water
1.0 mL
Concentration
5 mg/mL
5 mg Dose
1.0 mL (100 units)
2.5 mg Dose
0.50 mL (50 units)
1 mg Dose
0.20 mL (20 units)
200 mcg Dose
0.04 mL (4 units)
Vial Size
5 mg
BAC Water
2.0 mL
Concentration
2.5 mg/mL
5 mg Dose
2.0 mL (200 units*)
2.5 mg Dose
1.0 mL (100 units)
1 mg Dose
0.40 mL (40 units)
200 mcg Dose
0.08 mL (8 units)
Vial Size
10 mg
BAC Water
1.0 mL
Concentration
10 mg/mL
5 mg Dose
0.50 mL (50 units)
2.5 mg Dose
0.25 mL (25 units)
1 mg Dose
0.10 mL (10 units)
200 mcg Dose
0.02 mL (2 units)
Vial Size
10 mg
BAC Water
2.0 mL
Concentration
5 mg/mL
5 mg Dose
1.0 mL (100 units)
2.5 mg Dose
0.50 mL (50 units)
1 mg Dose
0.20 mL (20 units)
200 mcg Dose
0.04 mL (4 units)
Vial Size
10 mg
BAC Water
3.0 mL
Concentration
3.33 mg/mL
5 mg Dose
1.50 mL (150 units*)
2.5 mg Dose
0.75 mL (75 units)
1 mg Dose
0.30 mL (30 units)
200 mcg Dose
0.06 mL (6 units)
| Vial Size | BAC Water | Concentration | 5 mg Dose | 2.5 mg Dose | 1 mg Dose | 200 mcg Dose |
|---|---|---|---|---|---|---|
| 5 mg | 1.0 mL | 5 mg/mL | 1.0 mL (100 units) | 0.50 mL (50 units) | 0.20 mL (20 units) | 0.04 mL (4 units) |
| 5 mg | 2.0 mL | 2.5 mg/mL | 2.0 mL (200 units*) | 1.0 mL (100 units) | 0.40 mL (40 units) | 0.08 mL (8 units) |
| 10 mg | 1.0 mL | 10 mg/mL | 0.50 mL (50 units) | 0.25 mL (25 units) | 0.10 mL (10 units) | 0.02 mL (2 units) |
| 10 mg | 2.0 mL | 5 mg/mL | 1.0 mL (100 units) | 0.50 mL (50 units) | 0.20 mL (20 units) | 0.04 mL (4 units) |
| 10 mg | 3.0 mL | 3.33 mg/mL | 1.50 mL (150 units*) | 0.75 mL (75 units) | 0.30 mL (30 units) | 0.06 mL (6 units) |
* Volumes above 100 units exceed a standard 1 mL insulin syringe.
Plan around MOTS-c's 7-day window
MOTS-c is reconstituted-stable for about 7 days at 2-8 °C before potency starts to drop. Retatrutide holds for 28-60 days at 2-8 °C. Reconstitute MOTS-c in smaller volumes you can use within a week, or aliquot the reconstituted vial into freezer-safe containers for -20 °C storage (2-3 months).
Reconstituted Stability
Stability windows
Compound
Retatrutide
Lyophilized
12+ months at -20 °C
Reconstituted (2-8 °C)
Up to 28-60 days
Notes
Standard for GLP-class peptides.
Compound
MOTS-c
Lyophilized
12+ months at -20 °C
Reconstituted (2-8 °C)
Up to 7 days
Notes
Limiting factor for the stack. Aliquots at -20 °C: 2-3 months.
| Compound | Lyophilized | Reconstituted (2-8 °C) | Notes |
|---|---|---|---|
| Retatrutide | 12+ months at -20 °C | Up to 28-60 days | Standard for GLP-class peptides. |
| MOTS-c | 12+ months at -20 °C | Up to 7 days | Limiting factor for the stack. Aliquots at -20 °C: 2-3 months. |
Standard 7-Step Reconstitution
- 01
Warm up briefly
Let the lyophilized vial and BAC water reach room temperature before opening.
- 02
Wipe the stoppers
Swab both vial stoppers with alcohol and let them dry.
- 03
Draw BAC water
Pull the planned BAC water volume into a sterile syringe.
- 04
Direct flow against the wall
Inject the BAC water slowly down the inside of the vial. Do not aim it at the powder.
- 05
Roll, do not shake
Swirl or roll gently until fully dissolved. Shaking damages the peptide.
- 06
Label and confirm
Confirm the solution is clear. Label the vial with compound name, concentration, and date.
- 07
Refrigerate
Store at 2-8 °C. Use retatrutide within 28-60 days. Use MOTS-c within 7 days for best potency.
Calculator
Use the Peptide Reconstitution Calculator on PepPal for any custom vial size or BAC water volume across both compounds in this stack.
Why Researchers Combine Retatrutide and MOTS-c
Retatrutide is the workhorse of this stack. It does the heavy lifting on appetite, insulin signaling, and energy expenditure. The case for adding MOTS-c is that retatrutide alone leaves a gap inside the cell. Here is how each pathway is supposed to fit together.
Pathway 1 - Mitochondrial Fat Oxidation (AMPK)
MOTS-c activates AMP-activated protein kinase (AMPK), the energy sensor that flips muscle cells from preferring glucose to preferring fat. Retatrutide releases fatty acids from storage; MOTS-c reprograms the mitochondria to actually burn them. Without that downstream switch, mobilized fat can simply circulate and end up re-stored. This is the single most cited reason community protocols pair the two.
Pathway 2 - Insulin Sensitivity at Two Layers
Both compounds improve insulin signaling, but at different layers. Retatrutide acts on the GIP receptor at the islet cell, where insulin is made. MOTS-c works further downstream by improving glucose uptake into skeletal muscle independent of insulin spikes. In animal models, MOTS-c restored insulin sensitivity in aged and high-fat-fed mice at the muscle level - the same tissue where late-stage GLP-1 protocols often see metabolic slowdown.
Pathway 3 - Lean Mass Through Myostatin
Several preclinical studies link MOTS-c to reduced myostatin signaling. Myostatin is the protein that limits muscle growth. Less myostatin activity makes it easier to hold onto muscle during a deficit. This is the most speculative of the three pathways - direct human evidence is limited - but it is the rationale most often given for pairing MOTS-c with retatrutide specifically rather than with a slower-deficit compound.
Pathway 4 - Exercise-Mimetic Signaling
MOTS-c activates many of the same pathways as exercise: better endurance, better metabolic flexibility, more stress tolerance. In one preclinical study, old mice treated with MOTS-c doubled their treadmill running time and outperformed middle-aged comparators. During a deep retatrutide deficit - when fatigue and lower training capacity are common - this exercise-mimetic effect is the reason MOTS-c dosing usually lines up with training days.
When This Stack Beats Retatrutide Alone
If the goal is purely appetite-driven fat loss, retatrutide alone produced 28.7% body weight loss at the top dose in TRIUMPH-4 - no added compound needed. Researchers add MOTS-c when the goal is what happens to muscle and mitochondrial function during that deficit. That usually means advanced subjects, plateaued protocols, or longer cycles where metabolic adaptation becomes the limiting factor.
Reminder
The pathways above describe compound-level research and mechanism. No published human trial has measured outcomes for retatrutide + MOTS-c as a stack. The combination's synergy is mechanistic, not proven in a trial.
Retatrutide + MOTS-c Side Effects & Safety
Each compound has its own safety profile. Retatrutide has been studied in Phase 3. MOTS-c safety data comes from animals plus one analog (CB4211) human Phase 1 trial. The combination has not been tested in any trial, so the combined safety picture is built from adding each compound's known signals together.
Combined and Amplified Concerns
- Hypoglycemia risk. Retatrutide improves insulin response through GIP signaling. MOTS-c improves muscle glucose uptake through AMPK. Both move blood glucose down. Combining them - especially fasted, with metformin, or with berberine - can produce more hypoglycemia than either compound alone. Test glucose response in the early weeks.
- AMPK stacking with other AMPK activators. MOTS-c, metformin, and berberine all activate AMPK through different paths. Stacking multiple AMPK activators can amplify glucose-lowering unpredictably. If you use metformin or berberine, consider a lower MOTS-c dose and monitor closely. PepPal also explains why berberine is not "nature's Ozempic".
- Multi-source contamination risk. Two grey-market vials means two chances for contamination, label error, or sub-spec material. Verify both compounds against a Finnrick or comparable third-party COA, not just the supplier's documentation. See the PepPal guide to reading COAs.
- GI tolerance and injection burden. Retatrutide alone produced nausea in 38.1-43.2% of TRIUMPH-4 participants and discontinuation in 12.2-18.2% across the 9 mg and 12 mg arms. Adding a second injection-only compound raises injection-site irritation risk and can compound fatigue during the early adaptation weeks.
- Dysesthesia (retatrutide-specific). TRIUMPH-4 reported dysesthesia - unusual sensations like tingling - in 8.8% of 9 mg participants and 20.9% of 12 mg participants vs 0.7% on placebo. This is a retatrutide signal, not amplified by MOTS-c, but worth tracking at high reta doses.
Common Community-Reported Side Effects
- Nausea, diarrhea, constipation, vomiting (retatrutide-driven, dose-dependent).
- Injection-site redness or transient irritation (both compounds).
- Mild fatigue or lightheadedness during the first weeks of MOTS-c (AMPK adaptation).
- Appetite changes - usually suppression from retatrutide. A few MOTS-c users report increased hunger from enhanced fat mobilization.
- Disrupted sleep (occasional MOTS-c report at higher doses).
Contraindication Signals
Standard conservative practice excludes anyone with active gastrointestinal disease, type 1 diabetes, prior pancreatitis, medullary thyroid carcinoma history, or active cancer from any retatrutide protocol. Add caution for anyone using metformin, berberine, or other AMPK-active medications when MOTS-c is in the picture.
When to reassess
If GI symptoms worsen instead of improving over the first 2-3 weeks, if any unusual symptom appears, or if blood glucose readings drop more than expected, pause and consult a qualified clinician. For broader stacking-safety context see the PepPal side-effects guide.
Retatrutide + MOTS-c Clinical Evidence Context
Direct stack evidence
No published human or animal trial has tested retatrutide + MOTS-c together. The evidence summary below is per-compound only, drawn from the Phase 3 retatrutide program and the preclinical-plus-analog MOTS-c literature.
Retatrutide
Phase 3 TRIUMPH-4 (NCT05931367, 445 participants, 68 weeks) reported 28.7% body weight loss at 12 mg, 26.4% at 9 mg, vs 2.1% placebo. Phase 2 (Jastreboff et al., NEJM 2023) reported 24.2% weight loss at 48 weeks at 12 mg. The TRIUMPH program has six more Phase 3 readouts expected through 2026.
See the Retatrutide protocol page for the standalone reference.
MOTS-c
No completed human efficacy trial of the native peptide. Strong preclinical coverage: improved insulin sensitivity in aged and high-fat-fed mice (Lee et al., Cell Metabolism 2015) and roughly doubled treadmill running time in old mice (Reynolds et al., Nature Communications 2021). The closest human data is from CB4211, an analog that completed a Phase 1a/1b safety trial (NCT03998514) with well-tolerated SubQ dosing and favorable liver-enzyme and glucose trends.
See the MOTS-c protocol page for the standalone reference.
Combined Stack
The retatrutide + MOTS-c combination is a coverage model: retatrutide drives the systemic deficit through three hormone receptors, and MOTS-c targets the cellular layer where that deficit either gets converted to fat oxidation or stalls into adaptation. The mechanism map is consistent. The combined human evidence does not yet exist.
Retatrutide + MOTS-c Storage & Handling
Storage Reference (Both Compounds)
State
Lyophilized (long-term)
Retatrutide
-4 °F (-20 °C), 12+ months
MOTS-c
-4 °F (-20 °C), 12+ months
State
Lyophilized (short-term)
Retatrutide
35.6-46.4 °F (2-8 °C), several months
MOTS-c
35.6-46.4 °F (2-8 °C), several months
State
Lyophilized (room temp)
Retatrutide
Weeks (shipping tolerance only)
MOTS-c
Weeks (shipping tolerance only)
State
Reconstituted (liquid)
Retatrutide
35.6-46.4 °F (2-8 °C), up to 28-60 days
MOTS-c
35.6-46.4 °F (2-8 °C), up to 7 days
State
Aliquot frozen reconstituted
Retatrutide
Not standard practice
MOTS-c
-4 °F (-20 °C), 2-3 months
State
Color when reconstituted
Retatrutide
Clear
MOTS-c
Clear
State
Light protection
Retatrutide
Yes
MOTS-c
Yes
State
Oral viable
Retatrutide
No
MOTS-c
No
| State | Retatrutide | MOTS-c |
|---|---|---|
| Lyophilized (long-term) | -4 °F (-20 °C), 12+ months | -4 °F (-20 °C), 12+ months |
| Lyophilized (short-term) | 35.6-46.4 °F (2-8 °C), several months | 35.6-46.4 °F (2-8 °C), several months |
| Lyophilized (room temp) | Weeks (shipping tolerance only) | Weeks (shipping tolerance only) |
| Reconstituted (liquid) | 35.6-46.4 °F (2-8 °C), up to 28-60 days | 35.6-46.4 °F (2-8 °C), up to 7 days |
| Aliquot frozen reconstituted | Not standard practice | -4 °F (-20 °C), 2-3 months |
| Color when reconstituted | Clear | Clear |
| Light protection | Yes | Yes |
| Oral viable | No | No |
MOTS-c's 7-day reconstituted window is the limiting factor for storage planning. Use smaller MOTS-c reconstitutions or aliquot for freezer storage.
Retatrutide + MOTS-c vs Cagrilintide + Retatrutide vs Advanced Recomp Stack
How the retatrutide + MOTS-c stack compares
Feature
Components
Retatrutide + MOTS-c
Retatrutide + MOTS-c
Cagrilintide + Retatrutide
Retatrutide + Cagrilintide
Advanced Recomp Stack
Reta or tirz + tesamorelin or CJC/Ipa + MOTS-c (3+)
Feature
Pathway coverage
Retatrutide + MOTS-c
Triple agonist + AMPK / mitochondrial
Cagrilintide + Retatrutide
Triple agonist + amylin (extra satiety)
Advanced Recomp Stack
Triple agonist + GH axis + AMPK
Feature
Lean mass focus
Retatrutide + MOTS-c
Moderate (MOTS-c myostatin signal)
Cagrilintide + Retatrutide
Low (no dedicated lean-mass mechanism)
Advanced Recomp Stack
High (dedicated GH secretagogue)
Feature
Mitochondrial focus
Retatrutide + MOTS-c
High (MOTS-c is mitochondrial-derived)
Cagrilintide + Retatrutide
None
Advanced Recomp Stack
High (MOTS-c usually included)
Feature
Injections per week
Retatrutide + MOTS-c
2 compounds, 4-5 injections
Cagrilintide + Retatrutide
2 compounds, 2 injections
Advanced Recomp Stack
3+ compounds, 7+ injections
Feature
Cost (research-grade, monthly)
Retatrutide + MOTS-c
Moderate ($150-$300 combined)
Cagrilintide + Retatrutide
Moderate ($200-$400 combined)
Advanced Recomp Stack
High ($350-$600+ combined)
| Feature | Retatrutide + MOTS-c | Cagrilintide + Retatrutide | Advanced Recomp Stack |
|---|---|---|---|
| Components | Retatrutide + MOTS-c | Retatrutide + Cagrilintide | Reta or tirz + tesamorelin or CJC/Ipa + MOTS-c (3+) |
| Pathway coverage | Triple agonist + AMPK / mitochondrial | Triple agonist + amylin (extra satiety) | Triple agonist + GH axis + AMPK |
| Lean mass focus | Moderate (MOTS-c myostatin signal) | Low (no dedicated lean-mass mechanism) | High (dedicated GH secretagogue) |
| Mitochondrial focus | High (MOTS-c is mitochondrial-derived) | None | High (MOTS-c usually included) |
| Injections per week | 2 compounds, 4-5 injections | 2 compounds, 2 injections | 3+ compounds, 7+ injections |
| Cost (research-grade, monthly) | Moderate ($150-$300 combined) | Moderate ($200-$400 combined) | High ($350-$600+ combined) |
Cost ranges reflect typical research-grade pricing across COA-verified suppliers as of June 2026 - verify supplier pricing before ordering.
Decision Guidance
- Choose retatrutide + MOTS-c if your priority is fat oxidation efficiency and metabolic resilience during a deep deficit - especially if you think mitochondrial adaptation is the limiting factor.
- Choose cagrilintide + retatrutide if hunger and satiety are the main barrier, not fat oxidation. Cagrilintide adds appetite control through the amylin pathway.
- Choose the Advanced Recomp Stack if you want dedicated muscle preservation through a GH-axis compound, not just AMPK-mediated lean-mass support.
- Choose the klow stack dosage when the research context is tissue repair, skin quality, and inflammation control rather than metabolic weight-management signaling.
FAQ
Q1: Can you take MOTS-c with retatrutide?
Yes, but do not start both on the same day. Standard community protocols run retatrutide alone for the first 4 weeks at 1 mg weekly to confirm GI tolerance, then add MOTS-c at Week 5. The compounds use different mechanisms, so there are no known direct interactions, but both lower blood glucose, so monitor carefully if you also use metformin, berberine, or train fasted. See the dosing protocol for the specific weekly schedule.
Q2: How much MOTS-c should I take with retatrutide?
Two common approaches. The intermittent approach uses 5-10 mg of MOTS-c, 2-3 times per week, usually on training days. The low-dose daily approach starts at 200 mcg per day and steps up to about 1 mg per day. Most community protocols use the intermittent approach because MOTS-c stays active in the AMPK pathway for roughly 72 hours per injection.
Q3: What is the recommended dose when taking MOTS-c with retatrutide?
Retatrutide is titrated from 1 mg up by 4-week steps (1 → 2 → 4 → 6 → 9 mg), with 12 mg as the maximum tested dose. MOTS-c is added at Week 5 at 5 mg, 2-3 times per week. The full per-compound table and weekly schedule are in the dosing section.
Q4: Is there a pre-blended retatrutide + MOTS-c vial?
No. As of June 2026, no commercial supplier offers retatrutide and MOTS-c in a single pre-blended vial. The two compounds have very different reconstituted-stability windows - MOTS-c is only stable for about 7 days at 2-8 °C, while retatrutide stays stable for 28-60 days - which makes a pre-blend impractical. Use separate vials.
Q5: How do you reconstitute the retatrutide + MOTS-c stack?
Reconstitute each compound separately with bacteriostatic water. A 10 mg retatrutide vial with 1 mL BAC water gives 10 mg/mL (a 4 mg dose = 40 units on a U-100 syringe). A 10 mg MOTS-c vial with 1 mL BAC water gives 10 mg/mL (a 5 mg dose = 50 units). Inject the BAC water slowly down the inside of the glass, roll gently, never shake. Refrigerate both vials right after reconstitution. Use the PepPal calculator for any custom vial size.
Q6: Does MOTS-c help with muscle loss on retatrutide?
This is the main reason researchers pair them. Preclinical evidence links MOTS-c to reduced myostatin signaling - myostatin is the protein that limits muscle growth, so less of it makes it easier to keep muscle during a deficit. MOTS-c also activates AMPK in muscle and improves mitochondrial function, which supports training capacity when calories are low. No human trial has confirmed this for retatrutide protocols specifically - the case is mechanistic plus community observation. If lean mass is your top priority, the Advanced Recomp Stack adds a dedicated GH secretagogue.
Q7: Is the retatrutide + MOTS-c stack safe?
Each compound has been studied on its own, but the combination has not been tested in any trial. Retatrutide's TRIUMPH-4 trial reported nausea in 38.1-43.2% of participants, dysesthesia in 8.8-20.9% (dose-dependent), and discontinuation rates of 12.2-18.2%. MOTS-c safety data is limited to animal studies and the CB4211 analog Phase 1 trial. The main combined concerns are amplified hypoglycemia risk, GI tolerance, and the standard contamination risk of using two grey-market compounds. Verify both vials with a third-party COA. See the side effects section for the full breakdown.
Q8: How long should I run the retatrutide + MOTS-c stack?
Retatrutide is run open-ended in clinical trials - TRIUMPH-4 lasted 68 weeks, and post-trial expectation is indefinite maintenance once approved. MOTS-c is usually cycled: 4-8 weeks on, 2-4 weeks off, repeated through the retatrutide cycle. Most community protocols run the combined stack for 16-24 weeks before evaluating results and either continuing, tapering, or moving to maintenance. See the cycle guidelines for conservative, standard, and aggressive templates.
Q9: When during the day should you inject each compound?
Both are commonly dosed in the morning. Retatrutide is once-weekly and can be done any day at any time, but most users pick a fixed weekly day for consistency. MOTS-c is usually dosed in the morning on training days, ideally 30-60 minutes before exercise - that lines up with the peptide's natural exercise-induced expression pattern and is supported by animal-study timing data. Inject the two compounds at different sites if dosing on the same day.
Q10: Can you stack MOTS-c with metformin or berberine?
Use caution. MOTS-c, metformin, and berberine all activate AMPK through different paths. Combining multiple AMPK activators can amplify glucose-lowering unpredictably. If you already use metformin or berberine and want to add MOTS-c to a retatrutide protocol, consider lowering the MOTS-c dose, monitor blood glucose in the first weeks, and talk to a qualified clinician. The amplified AMPK effect is a theoretical concern that has not been formally characterized in humans.
Q11: How does retatrutide + MOTS-c compare to cagrilintide + retatrutide?
Both stacks pair retatrutide with a second compound that addresses a different limit. Cagrilintide + retatrutide adds the amylin analog cagrilintide to reinforce satiety - useful when hunger is the main barrier. Retatrutide + MOTS-c adds a mitochondrial-derived peptide to support cellular fat oxidation and lean mass through AMPK - useful when the limit is metabolic adaptation, fatigue, or lean-mass concerns rather than appetite. See the comparison table for the full side-by-side.
Q12: Can I add tesamorelin to retatrutide + MOTS-c?
That moves you out of the two-compound stack and into a three-compound protocol. Tesamorelin is a GH-releasing-hormone analog often added for visceral-fat and lean-mass support. The combined three-compound version is closer to the Advanced Recomp Stack, which formalizes that pairing. Adding tesamorelin without overhauling the schedule increases injection burden and complicates safety monitoring.
Q13: Can I take retatrutide and tirzepatide together?
Generally no. Retatrutide and tirzepatide both act on GLP-1 and GIP receptors - they overlap heavily on the same pathways. Stacking them adds redundant signaling, raises side-effect risk, and is not a pattern used in clinical trials. Most researchers switch from one to the other rather than running both.
Q14: What calculator should I use for retatrutide + MOTS-c math?
Use the free Peptide Reconstitution Calculator at PepPal for both compounds. It handles any vial size and BAC water volume, converts mg or mcg doses into syringe units automatically, and works for U-100 and U-50 syringes. Run it twice - once for each compound - and label each reconstituted vial with concentration and date.
Q15: Is this medical advice?
No. Everything on this page is for educational and research-reference purposes only. Retatrutide is a Phase 3 investigational compound not yet approved by any regulatory agency as of June 2026. MOTS-c is an unregulated research compound, FDA-ineligible for compounding, and prohibited by WADA under S4.4.1 (AMPK activators). Neither compound is approved for human therapeutic use in this combination. Consult a qualified healthcare provider before pursuing any peptide protocol.
Sources & Research
- 1. Eli Lilly and Company Lilly's triple agonist, retatrutide, delivered weight loss of up to an average of 71.2 lbs along with substantial relief from osteoarthritis pain in first successful Phase 3 trial. PRNewswire / Investor Release (2025)
- 2. Giblin K, Kaplan LM, Somers VK, Le Roux CW, Hunter DJ, et al. Retatrutide for the treatment of obesity, obstructive sleep apnea and knee osteoarthritis: Rationale and design of the TRIUMPH registrational clinical trials. Diabetes, Obesity and Metabolism (2026)
- 3. Lee C, Zeng J, Drew BG, Sallam T, Martin-Montalvo A, Wan J, Kim SJ, Mehta H, Hevener AL, de Cabo R, Cohen P. The Mitochondrial-Derived Peptide MOTS-c Promotes Metabolic Homeostasis and Reduces Obesity and Insulin Resistance. Cell Metabolism (2015)
- 4. Jastreboff AM, Kaplan LM, Frias JP, Wu Q, Du Y, Gurbuz S, Coskun T, Haupt A, Milicevic Z, Hartman ML. Triple-Hormone-Receptor Agonist Retatrutide for Obesity - A Phase 2 Trial. New England Journal of Medicine (2023)
- 5. Reynolds JC, Lai RW, Woodhead JST, Joly JH, Mitchell CJ, Cameron-Smith D, Lu R, Cohen P, Graham NA, Benayoun BA, Merry TL, Lee C. MOTS-c is an exercise-induced mitochondrial-encoded regulator of age-dependent physical decline and muscle homeostasis. Nature Communications (2021)
- 6. Kim J, Yang G, Kim Y, Kim J, Ha J. AMPK activators: mechanisms of action and physiological activities. Experimental & Molecular Medicine (2016)
- 7. BioSpace / Annalee Armstrong Lilly's Retatrutide Scores Triple Trial Triumph With 26% Weight Loss, But New Safety Signal Emerges. BioSpace (2025)
- 8. Patient Care Online Retatrutide Achieves Up to 28.7% Weight Loss and Marked Knee Pain Reduction in Phase 3 TRIUMPH-4 Trial. Patient Care Online (2025)
- 9. ClinicalTrials.gov A Study of Retatrutide (LY3437943) Once Weekly in Adults With Obesity and Knee Osteoarthritis (TRIUMPH-4). NCT05931367. ClinicalTrials.gov (2025)
- 10. ClinicalTrials.gov A Multiple-Ascending-Dose Study of CB4211 in Healthy Subjects and Subjects With Obesity and NAFLD. NCT03998514. ClinicalTrials.gov (2022)
- 11. World Anti-Doping Agency The Prohibited List 2026. WADA (2026)
- 12. California Trim Clinic Retatrutide + MOTS-c: The Elite Metabolic Stack Redefining Fat Loss. Press release via WFMJ.com (2026)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page