Wolverine Stack Quick Start
The Wolverine Stack is a community shorthand for pairing two research peptides — BPC-157 and TB-500 — into one tissue-repair-focused protocol. The name is borrowed from the comic-book character known for fast healing; it is not a clinical designation and not an FDA-approved treatment.
BPC-157 is studied for local tissue effects: angiogenesis at the injury site, growth-factor signaling, and tendon-bone interface healing in animal models. TB-500 is a fragment of Thymosin Beta-4 and is studied for systemic effects: cell migration, anti-inflammatory signaling, and progenitor-cell mobilization. The stack rationale is that the two compounds cover non-overlapping pieces of the same problem.
Two formats dominate research planning: a pre-blended 1:1 vial (most common is 20 mg total, 10 mg of each compound) dosed daily, or two separate vials dosed on different schedules — daily BPC-157 with twice-weekly TB-500 loading. This guide covers both. For unit math, see the PepPal reconstitution calculator.
Compounds
BPC-157 + TB-500, often as a 1:1 pre-blended 20 mg vial.
Schedule
Daily blend draws, or daily BPC-157 + 2x/week TB-500 separate-vial loading.
Reconstitute
2.0 mL BAC water in a 20 mg blend → 10 mg/mL total (5 mg/mL each).
Measuring
On a U-100 syringe, 10 units = 0.10 mL = 1.0 mg total blend.
Cycle
Most community protocols run 6–12 weeks total, often loading + maintenance.
Status
Not FDA-approved. Removed from Category 2 on Apr 22, 2026; PCAC review Jul 23, 2026.
Disclaimer
This page is an educational research reference. It is not medical advice, not a treatment plan, and not a recommendation to use these compounds. Neither BPC-157 nor TB-500 is FDA-approved. Both are prohibited by WADA. Use of unregulated research-chemical peptides carries quality-control and contamination risk, and there is no long-term human safety data for either compound.
This page is for Wolverine Stack steps, timing, and supplies. Want the wider research view? Visit the Wolverine Stack research guide. It covers each peptide, studies, safety notes, and legal status.
Wolverine Stack Dosing Protocol & Schedule
Two dosing models dominate Wolverine Stack research planning. The Pre-blended Vial is typically a 1:1 BPC-157 + TB-500 mixture, drawn as a single daily dose. Separate Vials lets BPC-157 and TB-500 run on independent schedules — daily BPC-157 with twice-weekly TB-500 loading. The choice usually comes down to whether independent dose control matters more than convenience.
Evidence boundary
No published clinical trial has tested BPC-157 + TB-500 together. Every dose range below is community-derived from individual-compound research. Numbers are reported as research planning context, not a dosing recommendation.
Wolverine Stack Dosing Guide
Choose the vial format you are using to see the matching schedule and math.
Convenience-first format. Most common is a 20 mg total vial containing 10 mg BPC-157 + 10 mg TB-500, reconstituted with 2.0 mL BAC water and dosed daily.
Blend ratio
1 : 1
BPC-157 and TB-500 delivered equally
20 mg total per vial: 10 mg BPC-157 + 10 mg TB-500, reconstituted with 2.0 mL bacteriostatic water for a final concentration of 10 mg/mL total blend (5 mg/mL each component).
Reconstitute
2.0 mL BAC water
Concentration
10 mg/mL total (5 mg/mL each)
Common daily draw
10 units = 1.0 mg total blend
Typical cycle
6–12 weeks
Dose selector
Component Delivery
| BPC-157 | 250 mcg |
|---|---|
| TB-500 | 250 mcg |
Pre-blended dosing typically delivers a steadier daily TB-500 exposure than the classic separate-vial 2x/week loading schedule.
Weekly exposure (5–7 days/week)
Weekly Exposure From the 1:1 Pre-blended Vial
Daily blend dose
0.5 mg/day
Weekly total blend
2.5–3.5 mg
Weekly BPC-157
1.25–1.75 mg
Weekly TB-500
1.25–1.75 mg
Daily blend dose
1.0 mg/day
Weekly total blend
5.0–7.0 mg
Weekly BPC-157
2.5–3.5 mg
Weekly TB-500
2.5–3.5 mg
Daily blend dose
1.5 mg/day
Weekly total blend
7.5–10.5 mg
Weekly BPC-157
3.75–5.25 mg
Weekly TB-500
3.75–5.25 mg
Daily blend dose
2.0 mg/day
Weekly total blend
10.0–14.0 mg
Weekly BPC-157
5.0–7.0 mg
Weekly TB-500
5.0–7.0 mg
| Daily blend dose | Weekly total blend | Weekly BPC-157 | Weekly TB-500 |
|---|---|---|---|
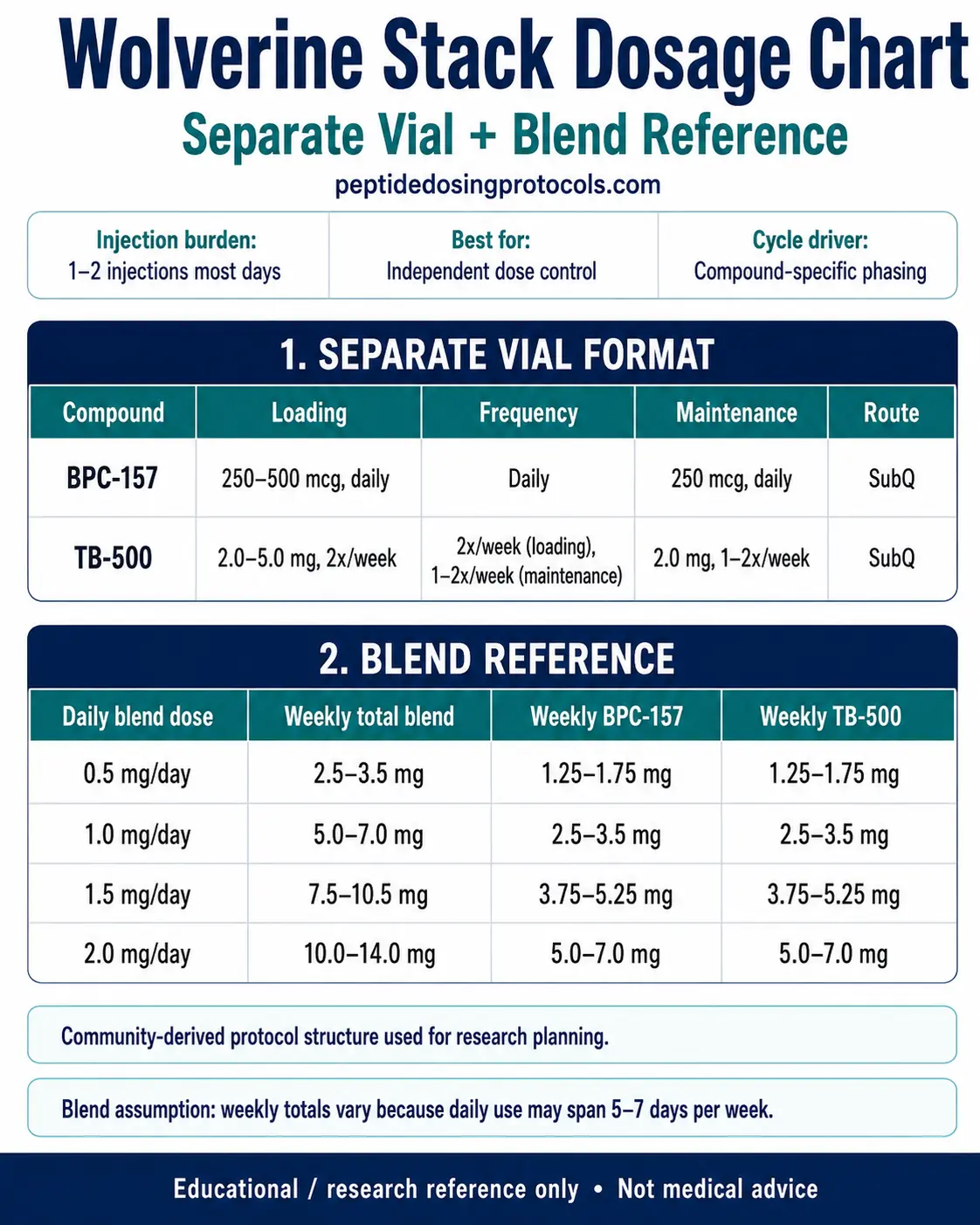
| 0.5 mg/day | 2.5–3.5 mg | 1.25–1.75 mg | 1.25–1.75 mg |
| 1.0 mg/day | 5.0–7.0 mg | 2.5–3.5 mg | 2.5–3.5 mg |
| 1.5 mg/day | 7.5–10.5 mg | 3.75–5.25 mg | 3.75–5.25 mg |
| 2.0 mg/day | 10.0–14.0 mg | 5.0–7.0 mg | 5.0–7.0 mg |
Use this to compare a blend schedule against the separate-vial weekly totals in the next tab.
Independent-control format. Best when BPC-157 and TB-500 doses need to be adjusted on different schedules — most often daily BPC-157 with twice-weekly TB-500 loading.
Separate-vial workflow
Independent dose control
Use separate vials when BPC-157 and TB-500 need different schedules. The most common pattern is daily BPC-157 paired with twice-weekly TB-500 during a loading phase, then a tapered maintenance phase.
Injection burden
1–2 injections most days
Best for
Independent dose control
Cycle driver
Compound-specific phasing
BPC-157
- Loading
- 250–500 mcg, daily
- Frequency
- Daily
- Maintenance
- 250 mcg, daily
- Route
- SubQ
TB-500
- Loading
- 2.0–5.0 mg, 2x/week
- Frequency
- 2x/week (loading), 1–2x/week (maintenance)
- Maintenance
- 2.0 mg, 1–2x/week
- Route
- SubQ
Example Weekly Schedule (Loading Phase)
Monday
BPC-157 500 mcg SubQ + TB-500 2.5 mg SubQ
Tuesday
BPC-157 500 mcg SubQ
Wednesday
BPC-157 500 mcg SubQ
Thursday
BPC-157 500 mcg SubQ + TB-500 2.5 mg SubQ
Friday
BPC-157 500 mcg SubQ
Saturday
BPC-157 500 mcg SubQ
Sunday
BPC-157 500 mcg SubQ
Use separate sterile syringes for separate-vial draws. Some protocols co-locate BPC-157 and TB-500 in the same SubQ region on shared days to reduce injection-site complexity.
Cycle structure
Cycle Guidelines (community-derived from compound-level data)
Approach
Pre-blended daily
Loading
—
Maintenance
0.5–2.0 mg total blend daily
Total cycle
6–12 weeks
Common context
Convenience-first, steady exposure
Approach
Separate vials standard
Loading
Weeks 1–4
Maintenance
Weeks 5–8
Total cycle
8–12 weeks
Common context
Loading-then-taper for injury planning
Approach
Separate vials extended
Loading
Weeks 1–4
Maintenance
Weeks 5–12
Total cycle
12 weeks
Common context
Slower-healing tissue research planning
| Approach | Loading | Maintenance | Total cycle | Common context |
|---|---|---|---|---|
| Pre-blended daily | — | 0.5–2.0 mg total blend daily | 6–12 weeks | Convenience-first, steady exposure |
| Separate vials standard | Weeks 1–4 | Weeks 5–8 | 8–12 weeks | Loading-then-taper for injury planning |
| Separate vials extended | Weeks 1–4 | Weeks 5–12 | 12 weeks | Slower-healing tissue research planning |
These are research-planning structures, not treatment plans. Off-cycle gaps of 2–4 weeks are commonly described in community protocols, but no formal cycling rule exists in the published literature.
Wolverine Stack Supplies Needed
These supply estimates assume a pre-blended 20 mg Wolverine vial containing 10 mg BPC-157 plus 10 mg TB-500. The planning dose is 1.0 mg total blend daily (0.5 mg of each compound), so one vial covers about 20 daily draws. Before checkout, compare current peptide discount codes for eligible research suppliers.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

Wolverine Stack Supplies

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Pre-blended Wolverine Vials (20 mg total, 1:1)
One 20 mg blend vial contains 10 mg BPC-157 plus 10 mg TB-500. At 1.0 mg total blend per day, each vial covers about 20 daily draws.
| Cycle length | Planning note |
|---|---|
4 weeks 2 vials | 28 daily draws; 40 mg total supply leaves about 12 mg residual. |
6-8 weeks 3 vials | 6 weeks: 42 daily draws; 60 mg total supply leaves about 18 mg residual.; 8 weeks: 56 daily draws; 60 mg total supply leaves about 4 mg residual. |
12 weeks 5 vials | 84 daily draws; 100 mg total supply leaves about 16 mg residual. |
4 weeks
2 vials
28 daily draws; 40 mg total supply leaves about 12 mg residual.
6-8 weeks
3 vials
6 weeks: 42 daily draws; 60 mg total supply leaves about 18 mg residual.; 8 weeks: 56 daily draws; 60 mg total supply leaves about 4 mg residual.
12 weeks
5 vials
84 daily draws; 100 mg total supply leaves about 16 mg residual.
Insulin Syringes (U-100, 0.3 mL or 0.5 mL)
One syringe per daily pre-blended injection.
| Cycle length | Planning note |
|---|---|
4 weeks 28 syringes | One daily pre-blended draw. |
6 weeks 42 syringes | One daily pre-blended draw. |
8 weeks 56 syringes | One daily pre-blended draw. |
12 weeks 84 syringes | One daily pre-blended draw; recommend 1 x 100-count box. |
4 weeks
28 syringes
One daily pre-blended draw.
6 weeks
42 syringes
One daily pre-blended draw.
8 weeks
56 syringes
One daily pre-blended draw.
12 weeks
84 syringes
One daily pre-blended draw; recommend 1 x 100-count box.
Bacteriostatic Water
Use 2 mL BAC water per pre-blended 20 mg vial.
| Cycle length | Planning note |
|---|---|
4-12 weeks 1 x 10 mL bottle | 4 weeks: 2 vials use 4 mL total; one bottle gives margin.; 6 weeks: 3 vials use 6 mL total.; 8 weeks: 3 vials use 6 mL total.; 12 weeks: 5 vials use 10 mL total; add margin if desired. |
4-12 weeks
1 x 10 mL bottle
4 weeks: 2 vials use 4 mL total; one bottle gives margin.; 6 weeks: 3 vials use 6 mL total.; 8 weeks: 3 vials use 6 mL total.; 12 weeks: 5 vials use 10 mL total; add margin if desired.
Round up for priming losses, dropped syringes, damaged swabs, and cycle adjustments. Separate-vial protocols require separate math because injection count and vial coverage change.
Companion Supplies & Routine Support
Pre-blended Vial vs Separate Vials: Which Format Fits the Plan
Both formats deliver the same two compounds. The choice changes how much control there is over each compound's dose and schedule, and how much injection-site management is needed.
Format Comparison
Factor
Daily injection burden
Pre-blended 1:1 vial
1 injection (combined)
Separate vials
1–2 injections (depending on day)
Factor
Dose control
Pre-blended 1:1 vial
Locked at 1:1 BPC-157 : TB-500
Separate vials
Independent BPC-157 and TB-500 doses
Factor
Schedule control
Pre-blended 1:1 vial
Both compounds on the same schedule
Separate vials
BPC-157 daily + TB-500 2x/week, etc.
Factor
TB-500 weekly exposure (typical)
Pre-blended 1:1 vial
1.25–7.0 mg/week (steady, daily)
Separate vials
4.0–10.0 mg/week (pulsed, 2x/week loading)
Factor
Reconstitution complexity
Pre-blended 1:1 vial
One vial
Separate vials
Two vials, two reconstitution steps
Factor
Best for
Pre-blended 1:1 vial
Simplicity, steady exposure
Separate vials
Injury-focused planning, dose tuning
| Factor | Pre-blended 1:1 vial | Separate vials |
|---|---|---|
| Daily injection burden | 1 injection (combined) | 1–2 injections (depending on day) |
| Dose control | Locked at 1:1 BPC-157 : TB-500 | Independent BPC-157 and TB-500 doses |
| Schedule control | Both compounds on the same schedule | BPC-157 daily + TB-500 2x/week, etc. |
| TB-500 weekly exposure (typical) | 1.25–7.0 mg/week (steady, daily) | 4.0–10.0 mg/week (pulsed, 2x/week loading) |
| Reconstitution complexity | One vial | Two vials, two reconstitution steps |
| Best for | Simplicity, steady exposure | Injury-focused planning, dose tuning |
Both formats cover the same total compounds; they differ in flexibility, not biology.
Wolverine Stack Reconstitution Guide
The featured math assumes a pre-blended 20 mg vial containing 10 mg BPC-157 plus 10 mg TB-500. Separate-vial planning can still use 10 mg of each compound, but those vials must be tracked independently. The PepPal reconstitution calculator handles unit math for any vial size.
Reconstitution by Format
Pick the vial format to see the matching math.
One 20 mg blend vial reconstituted with 2.0 mL BAC water.
Pre-blended Reconstitution
Spec
Vial size
Value
20 mg total (10 mg BPC-157 + 10 mg TB-500)
Spec
BAC water added
Value
2.0 mL
Spec
Total concentration
Value
10 mg/mL (5 mg/mL each compound)
Spec
10 units (0.10 mL) delivers
Value
0.5 mg BPC-157 + 0.5 mg TB-500
Spec
20 units (0.20 mL) delivers
Value
1.0 mg BPC-157 + 1.0 mg TB-500
Spec
Doses per vial (1.0 mg/day)
Value
~20 days
| Spec | Value |
|---|---|
| Vial size | 20 mg total (10 mg BPC-157 + 10 mg TB-500) |
| BAC water added | 2.0 mL |
| Total concentration | 10 mg/mL (5 mg/mL each compound) |
| 10 units (0.10 mL) delivers | 0.5 mg BPC-157 + 0.5 mg TB-500 |
| 20 units (0.20 mL) delivers | 1.0 mg BPC-157 + 1.0 mg TB-500 |
| Doses per vial (1.0 mg/day) | ~20 days |
Concentration scales linearly with BAC water volume — 3.0 mL gives ~6.7 mg/mL total (3.33 mg/mL each).
Reconstitute BPC-157 and TB-500 independently.
Separate-Vial Reconstitution
Spec
BAC water added
BPC-157 (10 mg vial)
2.0 mL
TB-500 (10 mg vial)
2.0 mL
Spec
Final concentration
BPC-157 (10 mg vial)
5.0 mg/mL
TB-500 (10 mg vial)
5.0 mg/mL
Spec
10 units (0.10 mL) delivers
BPC-157 (10 mg vial)
500 mcg
TB-500 (10 mg vial)
500 mcg
Spec
20 units (0.20 mL) delivers
BPC-157 (10 mg vial)
1.0 mg
TB-500 (10 mg vial)
1.0 mg
Spec
Doses per vial (typical)
BPC-157 (10 mg vial)
~20–40 days
TB-500 (10 mg vial)
~4–5 loading doses
| Spec | BPC-157 (10 mg vial) | TB-500 (10 mg vial) |
|---|---|---|
| BAC water added | 2.0 mL | 2.0 mL |
| Final concentration | 5.0 mg/mL | 5.0 mg/mL |
| 10 units (0.10 mL) delivers | 500 mcg | 500 mcg |
| 20 units (0.20 mL) delivers | 1.0 mg | 1.0 mg |
| Doses per vial (typical) | ~20–40 days | ~4–5 loading doses |
This separate-vial row keeps the same 10 mg-per-compound assumption as the 20 mg pre-blend, but the compounds are reconstituted and drawn independently.
Standard reconstitution steps
1. Allow lyophilized peptide to reach room temperature. 2. Wipe both vial stoppers (peptide and BAC water) with alcohol swabs. 3. Draw the planned volume of BAC water into a sterile syringe. 4. Inject the BAC water against the inside wall of the peptide vial — slowly, never directly onto the powder. 5. Swirl gently until fully dissolved; do not shake. 6. Verify the solution is clear (TB-500 may appear very faintly tinted). 7. Refrigerate (35.6–46.4°F / 2–8°C) and use within the supplier's stated beyond-use window.
Calculator
Use the PepPal reconstitution calculator for any vial size or BAC water volume not shown above.
Wolverine Stack Dosage Chart
This Wolverine Stack dosage chart summarizes the common pre-blended 20 mg vial schedule, including the 1:1 BPC-157 and TB-500 ratio, the 2 mL reconstitution setup, and the daily reference dose range.
Why the Wolverine Stack Pairs BPC-157 and TB-500
The stack rationale is mechanistic complementarity. BPC-157 and TB-500 both promote tissue repair, but through largely non-overlapping pathways. Pairing them is hypothesized — not proven — to give broader coverage than either alone.
BPC-157: local repair signaling
BPC-157 is a 15-amino-acid synthetic peptide derived from a sequence found in human gastric juice. Animal-model evidence consistently shows local effects: angiogenesis at the injury site (VEGF upregulation), growth-factor signaling (EGF, FGF), nitric oxide pathway modulation, and accelerated tendon-to-bone interface healing in rat Achilles transection studies.
TB-500: systemic cell migration
TB-500 is a synthetic fragment of Thymosin Beta-4, a 43-amino-acid actin-binding protein. The parent molecule has Phase 2 human data in cardiac and ocular contexts. Mechanistically, it acts systemically: it sequesters G-actin, promotes endothelial cell migration in scratch-wound assays, and has shown progenitor-cell mobilization signals in preclinical cardiac models.
Where they overlap and where they don't
Complementary Mechanism Targets
Target
Origin
BPC-157
Gastric juice protein fragment (15 amino acids)
TB-500
Thymosin Beta-4 fragment (LKKTETQ region)
Target
Primary action
BPC-157
Local tissue repair signaling
TB-500
Systemic cell migration and mobilization
Target
Angiogenesis
BPC-157
VEGF upregulation, NO pathway
TB-500
Endothelial migration, VEGF crosstalk
Target
Cell migration
BPC-157
Indirect, via growth factors
TB-500
Direct (G-actin sequestering)
Target
Best-evidence tissue
BPC-157
Tendon, gut, gastric mucosa (preclinical)
TB-500
Cardiac, corneal, skin (preclinical + early human Tβ4)
Target
Reported in vivo half-life
BPC-157
~4 hours (animal estimates)
TB-500
~2–3 days (animal estimates)
| Target | BPC-157 | TB-500 |
|---|---|---|
| Origin | Gastric juice protein fragment (15 amino acids) | Thymosin Beta-4 fragment (LKKTETQ region) |
| Primary action | Local tissue repair signaling | Systemic cell migration and mobilization |
| Angiogenesis | VEGF upregulation, NO pathway | Endothelial migration, VEGF crosstalk |
| Cell migration | Indirect, via growth factors | Direct (G-actin sequestering) |
| Best-evidence tissue | Tendon, gut, gastric mucosa (preclinical) | Cardiac, corneal, skin (preclinical + early human Tβ4) |
| Reported in vivo half-life | ~4 hours (animal estimates) | ~2–3 days (animal estimates) |
Half-life figures are pharmacokinetic estimates from animal studies; no published human PK data exists for either fragment.
Synergy is theoretical
No controlled study has tested whether the BPC-157 + TB-500 combination outperforms either compound alone. The rationale is mechanistic, not empirical.
Wolverine Stack Side Effects & Safety
There is no published human safety data for the Wolverine Stack as a combination. Compound-level data is summarized below, separated from theoretical and quality-control concerns.
Compound-level reported effects
BPC-157. Animal studies have reported low acute toxicity. The Vasireddi et al. 2025 systematic review notes the most-cited human exposure as a small open-label knee-pain case series in which 7 of 12 subjects reported pain relief lasting more than 6 months after one intra-articular BPC-157 injection; no serious adverse events were reported. There is no published RCT and no long-term human safety data.
TB-500 (Thymosin Beta-4 fragment). Phase 2 human trials of full-length Thymosin Beta-4 in pressure ulcers and venous stasis ulcers reported no significant adverse events distinguishable from placebo. The TB-500 fragment specifically has not completed a published RCT. Anecdotal reports include mild lethargy or head-pressure during loading phases, but these are not RCT-verified.
Theoretical and stack-level concerns
Both compounds promote angiogenesis, which is the intended mechanism for repair but is also a relevant pathway in tumor growth. A 2003 J Natl Cancer Inst paper by Cha et al. reported that Thymosin Beta-4 expression increased lung-tumor metastasis in a B16-F10 mouse model. The translational meaning for an exogenous TB-500 fragment in humans is unknown, but it is the most-cited theoretical risk in clinician reviews of this stack and is one reason researchers exclude individuals with active or undiagnosed cancer from any informal protocol.
Injection-site and quality-control risk
Reported injection-site issues include redness, mild swelling, transient bruising, and occasional sterile abscess. Most are attributable to technique rather than the peptide. Quality control is the larger practical risk. Independent third-party testing (e.g., Finnrick reports referenced on PepPal supplier pages) has shown variable purity, residual solvents, and endotoxin contamination across grey-market suppliers. Use COA-verified sources.
Sport and competition
Both BPC-157 and TB-500 are prohibited under WADA's S0 Unapproved Substances category, in and out of competition. Athletes subject to WADA, USADA, or any sport-governing-body testing program should not assume a clearance window — the substances are detectable and prohibited regardless of timing.
Wolverine Stack Clinical Evidence Context
There is no direct clinical evidence for the Wolverine Stack as a combination. No published trial — preclinical or human — has tested BPC-157 + TB-500 together. All clinical context comes from compound-level research.
BPC-157 evidence
The Vasireddi et al. 2025 systematic review in HSS Journal screened the full BPC-157 musculoskeletal literature through June 2024 and found a large preclinical base — tendon, ligament, muscle, bone, and nerve injury models — but only one published human exposure dataset, the small open-label knee-pain case series. Foundational tendon-bone work includes Krivic et al. 2006 (Achilles detachment in rat, J Orthop Res) and Chang et al. 2011 (tendon outgrowth and migration, J Appl Physiol). Wound-healing and gut work is reviewed in Seiwerth et al. 2021 (Front Vet Sci).
TB-500 / Thymosin Beta-4 evidence
Most TB-500 mechanism work is on the parent molecule Thymosin Beta-4. Foundational studies include Malinda et al. 1997 (FASEB J) showing endothelial cell migration in scratch-wound assays, and Smart et al. 2007 (Angiogenesis) reviewing angiogenic mechanism. The Tβ4 parent molecule has Phase 2 trial data in pressure-ulcer and venous-ulcer indications. The TB-500 fragment specifically has not completed a published RCT.
What this means for the stack
Compound-level evidence does not validate the combination. A coherent mechanistic rationale is not the same as demonstrated synergy, and animal-model effect sizes do not translate cleanly to human dosing. Treat any community-derived Wolverine schedule as a research-planning structure, not as evidence of effect.
Wolverine Stack Storage & Handling
Storage Conditions
State
Lyophilized (powder)
BPC-157
-4°F (-20°C) long-term; cool, dry, dark
TB-500
-4°F (-20°C) long-term; cool, dry, dark
State
Reconstituted (liquid)
BPC-157
35.6–46.4°F (2–8°C); use within ~30 days
TB-500
35.6–46.4°F (2–8°C); use within ~30 days
State
Light exposure
BPC-157
Protect from direct light
TB-500
Protect from direct light
State
Appearance
BPC-157
Clear post-reconstitution
TB-500
Clear or very faintly tinted
| State | BPC-157 | TB-500 |
|---|---|---|
| Lyophilized (powder) | -4°F (-20°C) long-term; cool, dry, dark | -4°F (-20°C) long-term; cool, dry, dark |
| Reconstituted (liquid) | 35.6–46.4°F (2–8°C); use within ~30 days | 35.6–46.4°F (2–8°C); use within ~30 days |
| Light exposure | Protect from direct light | Protect from direct light |
| Appearance | Clear post-reconstitution | Clear or very faintly tinted |
Beyond-use windows depend on supplier stability data and BAC water (vs. sterile water) reconstitution. Always defer to the supplier's stated stability window when available.
Wolverine Stack Regulatory Status (June 2026)
Neither BPC-157 nor TB-500 is FDA-approved as of June 2026. Both compounds were on the FDA's 503A Category 2 list — substances raising significant safety concerns and effectively blocked from compounding pharmacies — until April 22, 2026.
April 22, 2026: Removed from Category 2
On April 15, 2026, the FDA published a 503A category revision removing 12 peptides from Category 2 effective seven calendar days later (April 22). BPC-157 and TB-500 were both included. The removal happened because the original nominators voluntarily withdrew their nominations — it is not an FDA determination that these compounds are safe or approved for compounding.
July 23, 2026: Pharmacy Compounding Advisory Committee meeting
The FDA has scheduled a Pharmacy Compounding Advisory Committee (PCAC) meeting for July 23, 2026 to evaluate BPC-157 and TB-500 (free base and acetate forms), along with KPV and MOTs-C. PCAC will discuss inclusion on the 503A Bulks List. A vote at PCAC is a recommendation to FDA, not a final determination — a final 503A bulks-list decision typically follows weeks-to-months later.
What this means for access
Until PCAC recommends and FDA acts, neither compound is approved for compounding under 503A as a Category 1 substance. Research-chemical channels remain unregulated; compounding pharmacies may not yet legally compound these substances without further FDA action. WADA's S0 prohibition is unaffected by the FDA timeline.
Status changes
Regulatory status as written reflects June 2026. Outcomes from the July 23, 2026 PCAC meeting will materially change this section. Always verify the current 503A list at the FDA's bulk drug substances page.
Wolverine Stack vs Single Compounds vs Other Healing Stacks
Stack Comparison
Stack / compound
Wolverine Stack
Compounds
BPC-157 + TB-500
Primary research focus
Soft-tissue / tendon / systemic repair
Format note
1:1 pre-blend or separate vials
Stack / compound
BPC-157 alone
Compounds
BPC-157
Primary research focus
Local injury site, gut
Format note
Single 5 mg vial typical
Stack / compound
TB-500 alone
Compounds
TB-500 (Tβ4 fragment)
Primary research focus
Systemic mobility, cardiac (preclinical)
Format note
Single 10 mg vial typical
Stack / compound
GLOW Stack
Compounds
BPC-157 + TB-500 + GHK-Cu
Primary research focus
Adds skin/connective-tissue layer
Format note
Often blended vial
Stack / compound
KLOW Stack
Compounds
BPC-157 + TB-500 + GHK-Cu + KPV
Primary research focus
Adds inflammation/gut layer
Format note
Usually separate or part-blended
| Stack / compound | Compounds | Primary research focus | Format note |
|---|---|---|---|
| Wolverine Stack | BPC-157 + TB-500 | Soft-tissue / tendon / systemic repair | 1:1 pre-blend or separate vials |
| BPC-157 alone | BPC-157 | Local injury site, gut | Single 5 mg vial typical |
| TB-500 alone | TB-500 (Tβ4 fragment) | Systemic mobility, cardiac (preclinical) | Single 10 mg vial typical |
| GLOW Stack | BPC-157 + TB-500 + GHK-Cu | Adds skin/connective-tissue layer | Often blended vial |
| KLOW Stack | BPC-157 + TB-500 + GHK-Cu + KPV | Adds inflammation/gut layer | Usually separate or part-blended |
Stacks are not interchangeable. Adding compounds adds variables and quality-control risk; GLOW and KLOW have even less direct combination evidence than the Wolverine Stack.
BPC-157 + TB-500 Blood Tests & Monitoring
This stack is usually discussed around tissue repair and connective-tissue stress, but labs may not capture local tendon, ligament, or joint response. Monitoring is mainly a broad safety screen plus inflammation context when symptoms suggest it.
Blood test markers to discuss with a clinician
Marker
CBC with differential
Why it matters
Screens blood-cell patterns that can help flag infection, anemia, or immune changes before interpreting recovery symptoms.
Timing
Baseline
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver enzymes, kidney markers, electrolytes, and glucose in one broad safety panel.
Timing
Baseline
Marker
CRP
Why it matters
Can provide a general inflammation trend, although it does not show whether a local tendon or ligament is healing.
Timing
Optional
Marker
ESR
Why it matters
Adds another broad inflammation marker when symptoms, autoimmune history, or persistent swelling are part of the picture.
Timing
Optional
Marker
Creatine kinase (CK)
Why it matters
May be useful when muscle injury, hard training, or unusual muscle pain is present during a recovery-focused protocol.
Timing
Optional
Marker
Urinalysis
Why it matters
Can add kidney and hydration context when systemic symptoms, high training stress, or abnormal CMP kidney markers appear.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| CBC with differential | Screens blood-cell patterns that can help flag infection, anemia, or immune changes before interpreting recovery symptoms. | Baseline |
| Comprehensive metabolic panel (CMP) | Reviews liver enzymes, kidney markers, electrolytes, and glucose in one broad safety panel. | Baseline |
| CRP | Can provide a general inflammation trend, although it does not show whether a local tendon or ligament is healing. | Optional |
| ESR | Adds another broad inflammation marker when symptoms, autoimmune history, or persistent swelling are part of the picture. | Optional |
| Creatine kinase (CK) | May be useful when muscle injury, hard training, or unusual muscle pain is present during a recovery-focused protocol. | Optional |
| Urinalysis | Can add kidney and hydration context when systemic symptoms, high training stress, or abnormal CMP kidney markers appear. | Optional |
Monitoring is pathway-based because BPC-157 and TB-500 have limited human safety data and no established clinical lab-monitoring protocol.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with autoimmune disease, infection risk, cancer history, liver or kidney issues, anticoagulant use, or a recent major injury.
Follow-up
Repeat broad markers after 6-12 weeks if the protocol continues, symptoms change, or there are concerns about inflammation, infection, bruising, swelling, or recovery quality.
Longer term
For longer or repeated cycles, review trends every 3-6 months with a clinician because long-term human safety data are limited.
How to interpret the labs
- BPC-157 and TB-500 are not FDA-approved drugs, and human monitoring standards are not established.
- Normal labs do not prove that a tendon, ligament, muscle, or joint is healing correctly.
- Imaging, physical exam findings, pain pattern, strength, range of motion, and function may matter more than bloodwork for local injuries.
- Medication review is relevant with anticoagulants, immune-modulating drugs, cancer history, or planned procedures.
Do not wait for routine labs
Rapidly worsening swelling, warmth, redness, fever, or drainage near an injury or injection site needs medical review. New chest pain, shortness of breath, one-sided leg swelling, or fainting should be treated as urgent symptoms. Unusual bruising, bleeding, or severe allergic symptoms should not wait for routine lab follow-up. A sudden loss of strength, deformity, or inability to bear weight may need imaging or urgent injury evaluation.
FAQ
Q1: What is the Wolverine Stack?
The Wolverine Stack is a community shorthand for pairing two research peptides — BPC-157 and TB-500 — into one tissue-repair-focused protocol. It is not an FDA-approved treatment and not a clinical designation. The name comes from the comic-book character known for fast healing.
Q2: What is the typical Wolverine Stack dosage?
Two community-derived dosing models dominate. Pre-blended vial: 0.5–2.0 mg total of a 1:1 BPC-157 + TB-500 blend daily for 6–12 weeks. Separate vials: BPC-157 250–500 mcg daily plus TB-500 2–5 mg twice weekly during loading, with a tapered 8–12 week cycle. These are research-planning structures, not dosing recommendations.
Q3: What is the BPC-157 + TB-500 blend dosage chart?
From a 20 mg pre-blended vial reconstituted with 2.0 mL BAC water (10 mg/mL total, 5 mg/mL each compound): 5 units delivers 250 mcg of each, 10 units delivers 500 mcg of each, 15 units delivers 750 mcg of each, and 20 units delivers 1.0 mg of each compound. Use the PepPal calculator for other vial sizes.
Q4: Should I use a pre-blended vial or separate vials?
Pre-blended is simpler — one vial, one daily injection, locked 1:1 ratio. Separate vials let BPC-157 and TB-500 run on independent schedules (most often daily BPC-157 + twice-weekly TB-500 loading) and allow independent dose tuning. Both formats deliver the same compounds; the trade-off is convenience versus control.
Q5: What are the Wolverine Stack side effects?
There is no published human safety dataset for the combination. Compound-level reports from animal studies and small human exposure data describe low acute toxicity; the most common reported issue is injection-site reaction (redness, mild swelling, transient bruising). The most-cited theoretical concern is angiogenesis: both compounds promote new blood vessel formation, which is the intended repair mechanism but also a pathway relevant to tumor growth.
Q6: Is BPC-157 dangerous?
Animal studies and a small open-label human knee-pain case series (Vasireddi et al. 2025 systematic review, HSS Journal) reported no serious adverse events. There is no published long-term human safety data, no completed RCT, and the most-cited theoretical concern remains angiogenesis in the context of undiagnosed cancer. Quality of unregulated supply is also a real, separate risk.
Q7: Why is BPC-157 banned?
BPC-157 was prohibited under WADA's S0 Unapproved Substances category in 2022, restricting use in competition and training. The FDA placed BPC-157 in 503A Category 2 in 2023, which blocked compounding pharmacies from preparing it. On April 22, 2026, BPC-157 was removed from Category 2 because the original nominator withdrew. The FDA's PCAC meeting on July 23, 2026 will evaluate BPC-157 (free base and acetate) for inclusion on the 503A Bulks List.
Q8: Are BPC-157 and TB-500 FDA-approved?
No. As of June 2026, neither compound is FDA-approved. Both were removed from FDA 503A Category 2 on April 22, 2026, but neither is on Category 1 either. PCAC will evaluate both compounds on July 23, 2026, after which FDA will issue a 503A bulks-list determination. Both remain WADA-prohibited.
Q9: How long is a typical Wolverine Stack cycle?
Most community-derived protocols run 6–12 weeks total. A common separate-vial structure is 4 weeks of loading followed by 4–8 weeks of maintenance dosing. Pre-blended protocols often run a steady daily dose for the full cycle without a distinct loading phase. Off-cycle gaps of 2–4 weeks are commonly described but not formalized in any published trial.
Q10: What supplies do I need for a Wolverine Stack cycle?
A typical 8-week pre-blended cycle at 1.0 mg total blend daily uses 3 pre-blended 20 mg vials, 56 U-100 insulin syringes, one 10 mL bacteriostatic water bottle, and 112 alcohol swabs. Cycle-by-cycle math is in the supplies section above.
Q11: Is there any direct evidence the Wolverine Stack works better than either peptide alone?
No published trial — preclinical or human — has tested the combination. The synergy argument is mechanistic, based on non-overlapping pathways for local repair (BPC-157) and systemic cell migration (TB-500). Compound-level evidence does not validate the combination.
Q12: Is this medical advice?
No. This page is an educational research reference. It is not a treatment plan, not a recommendation to use these compounds, and not a substitute for evaluation by a qualified clinician.
Sources & Research
- 1. Vasireddi N, Hahamyan H, Salata MJ, et al. Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. HSS Journal (2025)
- 2. Krivic A, Anic T, Seiwerth S, Huljev D, Sikiric P. Achilles detachment in rat and stable gastric pentadecapeptide BPC 157: Promoted tendon-to-bone healing and opposed corticosteroid aggravation. Journal of Orthopaedic Research (2006)
- 3. Chang CH, Tsai WC, Lin MS, Hsu YH, Pang JHS. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. Journal of Applied Physiology (2011)
- 4. Seiwerth S, Milavic M, Vukojevic J, et al. Stable Gastric Pentadecapeptide BPC 157 and Wound Healing. Frontiers in Veterinary Science (PMC) (2021)
- 5. Sikiric P, Seiwerth S, Rucman R, et al. Multifunctionality and Possible Medical Application of the BPC 157 Peptide — Literature and Patent Review. Pharmaceuticals (MDPI) (2025)
- 6. Malinda KM, Goldstein AL, Kleinman HK. Thymosin beta 4 stimulates directional migration of human umbilical vein endothelial cells. FASEB Journal (1997)
- 7. Smart N, Risau W, Stanier P, Riley PR. Thymosin beta-4 and angiogenesis: modes of action and therapeutic potential. Angiogenesis (2007)
- 8. Malinda KM, Sidhu GS, Mani H, et al. Thymosin beta4 promotes angiogenesis, wound healing, and hair follicle development. Mechanisms of Ageing and Development (PubMed) (2004)
- 9. Xue B, Robinson RC. Progress on the Function and Application of Thymosin β4. Frontiers in Endocrinology (PMC) (2022)
- 10. Cha HJ, Jeong MJ, Kleinman HK. Role of thymosin beta4 in tumor metastasis and angiogenesis. Journal of the National Cancer Institute (2003)
- 11. U.S. Food and Drug Administration. July 23-24, 2026: Meeting of the Pharmacy Compounding Advisory Committee — BPC-157, KPV, TB-500, and MOTs-C bulk drug substances. FDA.gov (2026)
- 12. World Anti-Doping Agency. 2025 World Anti-Doping Code International Standard Prohibited List — Section S0 (Unapproved Substances). WADA (2025)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page