Cagrilintide + Tirzepatide Quick Start
The cagrilintide + tirzepatide stack pairs two once-weekly weight-loss peptides. Tirzepatide is a dual GLP-1 / GIP agonist - one weekly injection that hits two gut-hormone receptors. It is FDA-approved as Mounjaro (type 2 diabetes, 2022) and Zepbound (obesity, 2023). Cagrilintide is a long-acting amylin peptide that mimics the natural fullness hormone your pancreas releases after meals. It is investigational (not FDA-approved on its own).
Pairing them adds a third receptor pathway (amylin) on top of tirzepatide's GLP-1 and GIP coverage. The community calls this combo a few names: cag + tirz, tirz/cagri blend, amylin + dual incretin stack, or the 3-receptor stack. This page covers what the stack does, how researchers schedule it, the reconstitution math, injection logistics, side effects, and how it compares to CagriSema.
Format
Two separate vials is the standard. A few suppliers sell pre-blended versions (e.g. 5 mg / 5 mg cag/tirz).
Schedule
Both compounds are once weekly. Same day, different injection sites is the standard pattern.
Titration
Start tirzepatide alone for 8 weeks, then add cagrilintide at 0.25 mg/week.
Easy measuring
Both vials use U-100 insulin syringes for most doses.
Sourcing note
Tirzepatide can be prescription (Mounjaro/Zepbound) or research-use. Cagrilintide is research-use only.
Need broader context on combining peptides? See PepPal's stacking safety guide. For supplier and quality-control sourcing, see the PepPal supplier directory.
Disclaimer
This page is an educational research reference. It is not medical advice. No clinical trial has tested cagrilintide + tirzepatide together in humans. One preclinical study (Valdecantos et al. ADA 2024) showed combination benefit in obese rats. Tirzepatide is FDA-approved, but this combination is not. Cagrilintide is investigational only.
What Is the Cagrilintide + Tirzepatide Stack?
The cagrilintide + tirzepatide stack is a two-compound research protocol that combines an FDA-approved obesity drug with an investigational fullness peptide. The plain-English version: tirzepatide already does a lot - it cuts appetite and improves insulin signaling through two receptors. Cagrilintide adds a separate fullness signal that tirzepatide does not hit on its own.
This stack sits between two related stacks. CagriSema (cagrilintide + semaglutide) has Phase 3 trial data but uses a weaker incretin backbone (just GLP-1). The cagrilintide + retatrutide stack covers four receptors but uses an investigational triple agonist instead of an approved drug. Cag + tirz is the middle option: stronger incretin coverage than CagriSema, plus one approved component.
What Each Compound Does
Tirzepatide is a dual agonist: GLP-1 (cuts appetite, slows the stomach) and GIP (improves insulin signaling). In SURMOUNT-1 (Phase 3), tirzepatide at 15 mg produced 22.5% body weight loss at 72 weeks. In REDEFINE-4 (head-to-head vs CagriSema), tirzepatide reached about 25.5% at 84 weeks. It is sold as Mounjaro for type 2 diabetes and Zepbound for obesity.
Cagrilintide is a long-acting amylin analog. Amylin is a hormone your pancreas releases with insulin after meals. It works in the hindbrain (a different part of the brain than where GLP-1 acts) to tell you that you have had enough food. Cagrilintide alone produced about 10.8% weight loss at 26 weeks in monotherapy (Lau et al., 2021). Combined with semaglutide as CagriSema, it pushed weight loss to about 22.7% at 68 weeks (REDEFINE-1).
Why People Pair Them
Tirzepatide hits two receptors. Cagrilintide hits a third one (amylin) that tirzepatide does not reach. The combined logic is:
- Three receptor pathways at once. Appetite (GLP-1) + insulin signaling (GIP) + fullness (amylin). No other current two-compound stack covers all three with an FDA-approved base.
- Two separate satiety channels. GLP-1 tells your gut to slow down. Amylin tells your hindbrain you are full. Different brain regions, different pathways.
- Preclinical combination data exists. One animal study (Valdecantos et al., ADA 2024) showed obese rats given both compounds at sub-maximal doses lost more weight than either compound alone.
- Approved base, lower sourcing risk. Half the stack (tirzepatide) is an FDA-approved drug. This makes quality verification easier than running two investigational compounds.
Evidence boundary
No human clinical trial has tested cagrilintide + tirzepatide together. One preclinical rat study supports synergy. Beyond that, the pairing rationale is built from each compound's own data plus the CagriSema (cag + sema) Phase 3 results.
Why Researchers Combine Cagrilintide and Tirzepatide
Adding a second compound to tirzepatide only makes sense if it covers something tirzepatide misses. Here is how each piece fits together.
Foundation - What Tirzepatide Already Provides
Tirzepatide is the strongest FDA-approved single drug for obesity, outperforming semaglutide in head-to-head trials. It works through two receptors: GLP-1 suppresses appetite and slows digestion, and GIP supports insulin sensitivity and metabolic efficiency. Together these are called dual incretin signaling. For monotherapy details, see the tirzepatide protocol page.
The Missing Pathway - Amylin Satiety
Tirzepatide does not activate amylin receptors. Amylin signals in the hindbrain - a separate part of the brain from where GLP-1 acts. The simplest way to picture it: GLP-1 tells your gut to slow down, while amylin tells your brain you have had enough food - through a different channel. Adding cagrilintide gives you appetite suppression from two different brain regions instead of one.
Preclinical Synergy Data
The one direct combination study comes from an animal trial. Valdecantos et al. (ADA 2024) gave cagrilintide and tirzepatide together to obese rats. At sub-maximal doses, the combination produced greater weight loss than either compound alone. Some metabolic markers also improved. This is encouraging but limited - animal results do not always carry over to humans, and this is one study, not a body of evidence.
Stacked Digestion Slowdown
Both compounds slow gastric emptying through different mechanisms. Combining them stretches fullness even longer after meals, but it also stacks the risk of nausea, vomiting, and constipation. This overlap is the main reason for staggered titration - start one compound first, build tolerance, then add the second.
Reminder
The pathways above describe compound-level research and one preclinical combination study. No human trial has measured outcomes for cagrilintide + tirzepatide as a stack. CagriSema (cag + sema) is the closest analog with human trial data.
Cagrilintide + Tirzepatide Dosing Protocol & Schedule
Evidence-level notice
No human clinical trial has tested cagrilintide + tirzepatide together. The dosing structure below is community-derived from each compound's Phase 2/3 data plus the Valdecantos 2024 preclinical synergy paper. Treat this as conservative protocol planning.
Separate vials is the standard format. A few suppliers sell pre-blended cag/tirz vials (most often at a 5 mg / 5 mg ratio or similar), but the dose math is more flexible with separate vials. The schedule below assumes the separate-vial approach, which is also what the staggered titration is built around.
Separate-vial workflow
Staggered Co-Titration - Two Vials, Two Schedules
Run tirzepatide alone for 8 weeks first. Add cagrilintide at Week 9 at the lowest dose. Step both compounds up slowly over the next 16 weeks to reach maintenance.
Injection burden
2 injections per week from Week 9 on
Best for
First-time stack users; staggered titration
Cycle driver
GI tolerance sets the pace
Tirzepatide
- Loading
- 2.5 → 5 → 7.5 → 10 → 12.5 mg (every 4 weeks)
- Frequency
- Once weekly
- Maintenance
- 15 mg weekly
- Route
- SubQ
Cagrilintide
- Loading
- Start Week 9: 0.25 → 0.5 → 1.0 → 1.7 mg
- Frequency
- Once weekly
- Maintenance
- 2.4 mg weekly
- Route
- SubQ
Weekly Schedule Example (Maintenance Phase)
Monday
Tirzepatide 15 mg (one site) + Cagrilintide 2.4 mg (different site)
Tuesday
No injections
Wednesday
No injections
Thursday
No injections
Friday
No injections
Saturday
No injections
Sunday
No injections
Both compounds are once weekly. Use separate syringes - do not mix them. Pick the same day each week for consistency. Rotate sites across abdomen, thigh, and flank to prevent local irritation.
Full Staggered Titration Schedule
Recommended staggered co-titration across 24 weeks
Phase
Tirz initiation
Weeks
1-4
Tirzepatide
2.5 mg/week
Cagrilintide
Not started
Notes
Confirm tirzepatide GI tolerance first.
Phase
Tirz escalation 1
Weeks
5-8
Tirzepatide
5.0 mg/week
Cagrilintide
Not started
Notes
Continue tirzepatide alone.
Phase
Cag introduction
Weeks
9-12
Tirzepatide
5.0 mg/week (hold)
Cagrilintide
0.25 mg/week
Notes
Add cagrilintide at the lowest dose. Hold tirz steady.
Phase
Dual escalation 1
Weeks
13-16
Tirzepatide
7.5 mg/week
Cagrilintide
0.5 mg/week
Notes
GI side effects often peak here.
Phase
Dual escalation 2
Weeks
17-20
Tirzepatide
10.0 mg/week
Cagrilintide
1.0 mg/week
Notes
Both compounds step up.
Phase
Dual escalation 3
Weeks
21-24
Tirzepatide
12.5 mg/week
Cagrilintide
1.7 mg/week
Notes
Approach maintenance.
Phase
Maintenance
Weeks
25+
Tirzepatide
15.0 mg/week
Cagrilintide
2.4 mg/week
Notes
Full 3-receptor coverage if tolerated.
| Phase | Weeks | Tirzepatide | Cagrilintide | Notes |
|---|---|---|---|---|
| Tirz initiation | 1-4 | 2.5 mg/week | Not started | Confirm tirzepatide GI tolerance first. |
| Tirz escalation 1 | 5-8 | 5.0 mg/week | Not started | Continue tirzepatide alone. |
| Cag introduction | 9-12 | 5.0 mg/week (hold) | 0.25 mg/week | Add cagrilintide at the lowest dose. Hold tirz steady. |
| Dual escalation 1 | 13-16 | 7.5 mg/week | 0.5 mg/week | GI side effects often peak here. |
| Dual escalation 2 | 17-20 | 10.0 mg/week | 1.0 mg/week | Both compounds step up. |
| Dual escalation 3 | 21-24 | 12.5 mg/week | 1.7 mg/week | Approach maintenance. |
| Maintenance | 25+ | 15.0 mg/week | 2.4 mg/week | Full 3-receptor coverage if tolerated. |
Step back if GI side effects become intense. Holding a step longer is always better than pushing through.
Cycle Guidelines
Common Cagrilintide + Tirzepatide Cycle Approaches
Approach
Full staggered titration
Duration
24-week ramp + open-ended maintenance
Off Period
No standardized off period
Best For
Primary weight-loss strategy with full pathway coverage
Approach
Tirz-first, cag add-on
Duration
Stabilize tirzepatide at 10-15 mg, then add cag for 12+ weeks
Off Period
Cag can be cycled on its own
Best For
Users already on tirzepatide who want more satiety
Approach
Sub-maximal combination
Duration
Lower doses of each (e.g. tirz 10 mg + cag 1.2 mg)
Off Period
As needed
Best For
Tolerability-focused; based on Valdecantos 2024 sub-max data
| Approach | Duration | Off Period | Best For |
|---|---|---|---|
| Full staggered titration | 24-week ramp + open-ended maintenance | No standardized off period | Primary weight-loss strategy with full pathway coverage |
| Tirz-first, cag add-on | Stabilize tirzepatide at 10-15 mg, then add cag for 12+ weeks | Cag can be cycled on its own | Users already on tirzepatide who want more satiety |
| Sub-maximal combination | Lower doses of each (e.g. tirz 10 mg + cag 1.2 mg) | As needed | Tolerability-focused; based on Valdecantos 2024 sub-max data |
Taper tirzepatide at the end of a cycle rather than stopping suddenly. Cagrilintide can be stopped or kept at maintenance.
Injection Logistics - Same Day, Same Time, Same Site?
This is the most-asked question about this stack. The short answer: same day is fine, different injection sites are required, same syringe is not allowed.
- Same day, same time: Yes. Both compounds are once weekly. Most users dose both at the same time on the same day. This is simpler than splitting them across the week.
- Different sites: Yes, required. Use one site for tirzepatide (e.g. abdomen) and a different site for cagrilintide (e.g. thigh). This reduces local irritation and helps you tell if one compound is causing site reactions.
- Same port / same syringe: No. Do not mix the two compounds in one syringe or inject through the same skin puncture. The compounds have different stability profiles and pH characteristics.
- Split across the week: Optional. Some users split the doses - tirzepatide Monday, cagrilintide Thursday - to spread out the GI burden, especially during titration. This is fine but not required.
- Adding cagrilintide mid-cycle: Start cagrilintide on a tirzepatide injection day so they line up going forward. The first cagrilintide dose can be the same day as a regular tirzepatide dose, just at a different site.
Protocol Notes
- No oral options. Neither compound is orally bioavailable in these formulations. Both must be injected.
- Slow GI escalation matters more than speed. Pushing doses up too fast is the single biggest cause of dropping out. Hold each step at least 4 weeks. Drop back a step if you cannot eat.
- Do not combine with semaglutide. Tirzepatide already covers GLP-1 receptors. Adding semaglutide adds redundancy without new pathway coverage.
- Do not combine with retatrutide. Retatrutide already covers GLP-1 and GIP (the same receptors tirzepatide hits). Stacking them adds redundant signaling and side-effect risk.
- Do not combine with pramlintide. Cagrilintide already covers amylin signaling. Pramlintide is a short-acting amylin analog and adds nothing new.
- When does cagrilintide kick in? Cagrilintide is long-acting (half-life ~7-8 days). Most users report noticeable appetite suppression by Week 2-3 after starting it. Tirzepatide effects often appear within the first 1-2 weeks.
Cagrilintide + Tirzepatide Supplies Needed
Plan based on the staggered schedule. Tirzepatide runs for the full cycle. Cagrilintide starts at Week 9 in the staggered approach. Round up to leave a margin for priming losses and dropped syringes.
Recommended USA Supply
Use discount code SAVE10 at Peptira checkout. See why we love Peptira.
Cagrilintide

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Tirzepatide Vials
Once-weekly dosing, titrated upward. A 10 mg vial covers 1-4 weekly doses depending on the dose step. 30 mg vials are common at maintenance.
| Cycle length | Planning note |
|---|---|
16 weeks (titration phase) 2-3 x 10 mg vials | 2.5 → 5 → 7.5 mg weekly through Week 16; ~80 mg total used. |
24 weeks (full titration) 2 x 30 mg vials (or 5-6 x 10 mg) | Maintenance at 15 mg/week uses one 30 mg vial every 2 weeks. |
48 weeks (titration + maintenance) 12-15 x 10 mg or 4-5 x 30 mg vials | Maintenance at 15 mg weekly drives most of the total. |
16 weeks (titration phase)
2-3 x 10 mg vials
2.5 → 5 → 7.5 mg weekly through Week 16; ~80 mg total used.
24 weeks (full titration)
2 x 30 mg vials (or 5-6 x 10 mg)
Maintenance at 15 mg/week uses one 30 mg vial every 2 weeks.
48 weeks (titration + maintenance)
12-15 x 10 mg or 4-5 x 30 mg vials
Maintenance at 15 mg weekly drives most of the total.
Cagrilintide Vials
Cagrilintide starts at Week 9 in the staggered approach. A 10 mg vial covers ~4 weeks at maintenance dose (2.4 mg/week).
| Cycle length | Planning note |
|---|---|
16 weeks (cag from Week 9) 1 x 5 mg vial | Only 8 weeks of cagrilintide at low doses; minimal use. |
24 weeks 1 x 10 mg vial | Doses are still well under 2 mg/week through Week 20. |
48 weeks 3-4 x 10 mg vials | Maintenance at 2.4 mg/week drives most use. |
16 weeks (cag from Week 9)
1 x 5 mg vial
Only 8 weeks of cagrilintide at low doses; minimal use.
24 weeks
1 x 10 mg vial
Doses are still well under 2 mg/week through Week 20.
48 weeks
3-4 x 10 mg vials
Maintenance at 2.4 mg/week drives most use.
Insulin Syringes (U-100)
Use 1 mL syringes for higher tirzepatide doses (15 mg = 150 units at 10 mg/mL). 0.3 mL syringes work for cagrilintide doses.
| Cycle length | Planning note |
|---|---|
16 weeks ~20 syringes | 1 tirz/week from Week 1; 2 injections/week from Week 9. |
24 weeks ~40 syringes | Two injections per week from Week 9 onward. |
48 weeks ~80 syringes | Buy in bulk; one syringe per injection. |
16 weeks
~20 syringes
1 tirz/week from Week 1; 2 injections/week from Week 9.
24 weeks
~40 syringes
Two injections per week from Week 9 onward.
48 weeks
~80 syringes
Buy in bulk; one syringe per injection.
Bacteriostatic Water
Each vial is reconstituted separately. Plan around the 28-30 day stability window for both compounds.
| Cycle length | Planning note |
|---|---|
16 weeks 1 x 10 mL bottle | Covers 2-4 reconstitutions with margin. |
24 weeks 1-2 x 10 mL bottles | Second bottle gives margin for fresh reconstitutions. |
48 weeks 2-3 x 10 mL bottles | New vials need fresh BAC water each time. |
16 weeks
1 x 10 mL bottle
Covers 2-4 reconstitutions with margin.
24 weeks
1-2 x 10 mL bottles
Second bottle gives margin for fresh reconstitutions.
48 weeks
2-3 x 10 mL bottles
New vials need fresh BAC water each time.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments. Both vials are stable for 28-30 days at 2-8 °C once reconstituted, so plan vial sizes around 4-week use.
Companion Supplies & Routine Support
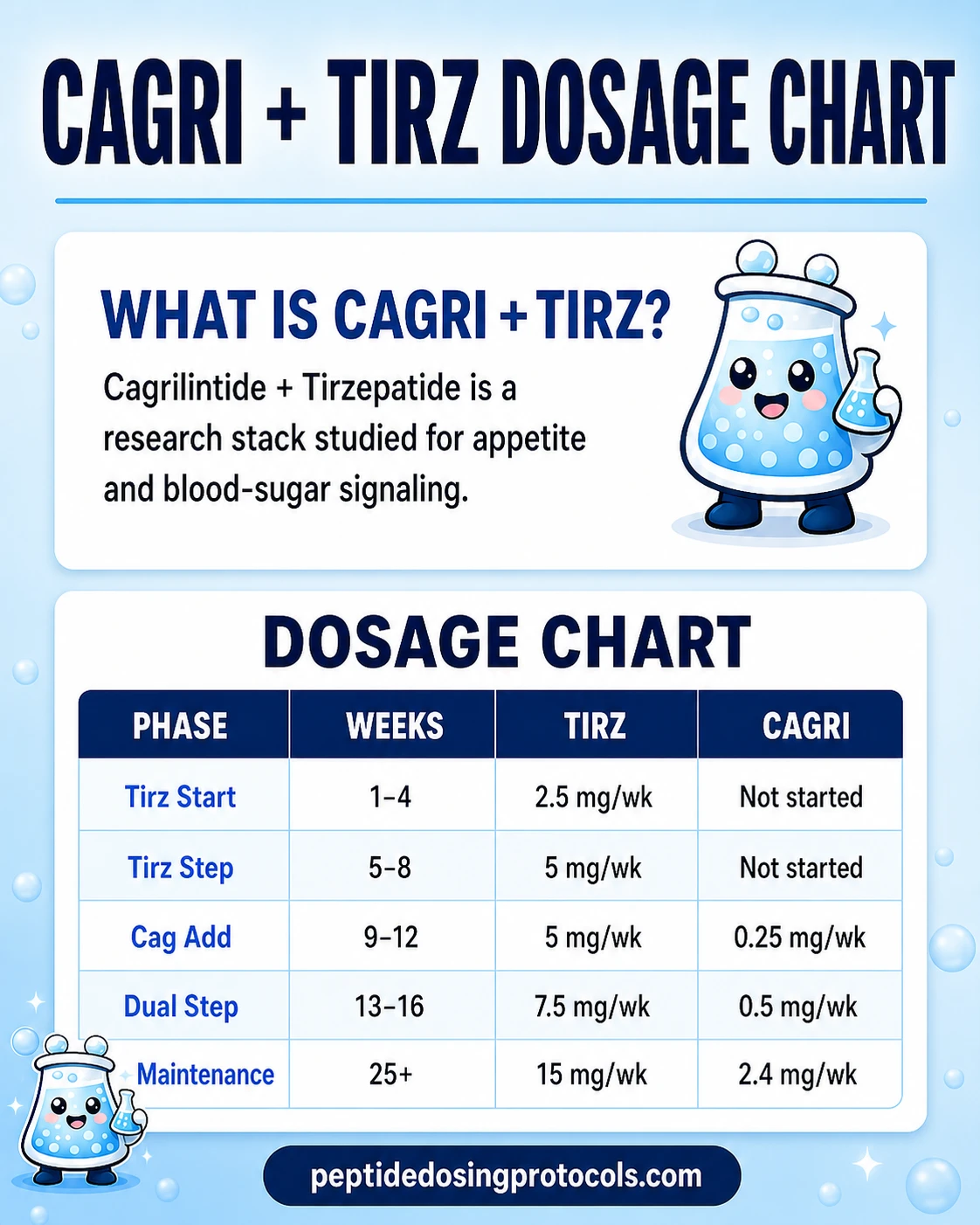
Cagrilintide + Tirzepatide Dosage Chart
This Cagrilintide + Tirzepatide dosage chart summarizes the staggered tirzepatide and cagrilintide weekly titration phases shown in the dosing section above.
Cagrilintide + Tirzepatide Reconstitution Guide
Each vial is reconstituted on its own. The math below mirrors the Tirzepatide protocol page and the Cagrilintide protocol page so the numbers match across the site.
Label every vial
Both compounds use U-100 insulin syringes. A draw error matters - 0.5 mL at tirzepatide 10 mg/mL is 5 mg of tirzepatide. The same volume at cagrilintide 2.5 mg/mL is only 1.25 mg of cagrilintide. The compounds are dosed at very different scales. Label each vial with the compound name, concentration, and reconstitution date.
Tirzepatide Reconstitution Math
Tirzepatide - dose per draw at common vial sizes
Vial Size
5 mg
BAC Water
1.0 mL
Concentration
5 mg/mL
2.5 mg
0.50 mL (50 units)
5 mg
1.00 mL (100 units)
10 mg
N/A
15 mg
N/A
Vial Size
10 mg
BAC Water
2.0 mL
Concentration
5 mg/mL
2.5 mg
0.50 mL (50 units)
5 mg
1.00 mL (100 units)
10 mg
2.00 mL (200 units*)
15 mg
3.00 mL (300 units*)
Vial Size
10 mg
BAC Water
1.0 mL
Concentration
10 mg/mL
2.5 mg
0.25 mL (25 units)
5 mg
0.50 mL (50 units)
10 mg
1.00 mL (100 units)
15 mg
1.50 mL (150 units*)
Vial Size
30 mg
BAC Water
3.0 mL
Concentration
10 mg/mL
2.5 mg
0.25 mL (25 units)
5 mg
0.50 mL (50 units)
10 mg
1.00 mL (100 units)
15 mg
1.50 mL (150 units*)
| Vial Size | BAC Water | Concentration | 2.5 mg | 5 mg | 10 mg | 15 mg |
|---|---|---|---|---|---|---|
| 5 mg | 1.0 mL | 5 mg/mL | 0.50 mL (50 units) | 1.00 mL (100 units) | N/A | N/A |
| 10 mg | 2.0 mL | 5 mg/mL | 0.50 mL (50 units) | 1.00 mL (100 units) | 2.00 mL (200 units*) | 3.00 mL (300 units*) |
| 10 mg | 1.0 mL | 10 mg/mL | 0.25 mL (25 units) | 0.50 mL (50 units) | 1.00 mL (100 units) | 1.50 mL (150 units*) |
| 30 mg | 3.0 mL | 10 mg/mL | 0.25 mL (25 units) | 0.50 mL (50 units) | 1.00 mL (100 units) | 1.50 mL (150 units*) |
* Volumes above 100 units exceed a standard 1 mL insulin syringe.
Cagrilintide Reconstitution Math
Cagrilintide - dose per draw at common vial sizes
Vial Size
5 mg
BAC Water
2.0 mL
Concentration
2.5 mg/mL
0.25 mg
0.10 mL (10 units)
0.5 mg
0.20 mL (20 units)
1.0 mg
0.40 mL (40 units)
2.4 mg
0.96 mL (96 units)
Vial Size
10 mg
BAC Water
2.0 mL
Concentration
5.0 mg/mL
0.25 mg
0.05 mL (5 units)
0.5 mg
0.10 mL (10 units)
1.0 mg
0.20 mL (20 units)
2.4 mg
0.48 mL (48 units)
Vial Size
10 mg
BAC Water
1.0 mL
Concentration
10.0 mg/mL
0.25 mg
0.025 mL (2.5 units)
0.5 mg
0.05 mL (5 units)
1.0 mg
0.10 mL (10 units)
2.4 mg
0.24 mL (24 units)
| Vial Size | BAC Water | Concentration | 0.25 mg | 0.5 mg | 1.0 mg | 2.4 mg |
|---|---|---|---|---|---|---|
| 5 mg | 2.0 mL | 2.5 mg/mL | 0.10 mL (10 units) | 0.20 mL (20 units) | 0.40 mL (40 units) | 0.96 mL (96 units) |
| 10 mg | 2.0 mL | 5.0 mg/mL | 0.05 mL (5 units) | 0.10 mL (10 units) | 0.20 mL (20 units) | 0.48 mL (48 units) |
| 10 mg | 1.0 mL | 10.0 mg/mL | 0.025 mL (2.5 units) | 0.05 mL (5 units) | 0.10 mL (10 units) | 0.24 mL (24 units) |
Cagrilintide is sensitive - inject BAC water down the vial wall and swirl gently. Do not shake.
Math verification
Tirzepatide 10 mg vial + 1.0 mL BAC → 10 mg/mL. A 15 mg dose = 1.50 mL (150 units). A 5 mg dose = 0.50 mL (50 units). Cagrilintide 5 mg vial + 2.0 mL BAC → 2.5 mg/mL. A 2.4 mg dose = 0.96 mL (96 units). 30 mg tirzepatide vial + 3.0 mL BAC → 10 mg/mL. A 15 mg dose = 1.50 mL (150 units).
Pre-Blended Vials (Less Common)
A few suppliers sell pre-blended cag/tirz vials, usually at a 5 mg cag + 5 mg tirz ratio (10 mg total) or similar. Pre-blends simplify handling but lock the ratio. Always verify the actual mg breakdown on the vial label before reconstituting - supplier brand names vary. For a 5/5 mg blend reconstituted with 2.0 mL BAC water, you get 2.5 mg/mL of each compound, so a 0.20 mL draw delivers 0.5 mg cag + 0.5 mg tirz.
Reconstituted Stability
Stability windows for both compounds
Compound
Tirzepatide
Lyophilized
12+ months at -20 °C
Reconstituted (2-8 °C)
28-30 days
Notes
Standard for incretin-class peptides.
Compound
Cagrilintide
Lyophilized
12+ months at -20 °C
Reconstituted (2-8 °C)
28-30 days
Notes
Do not shake (amyloid fibril risk). Discard cloudy solution.
| Compound | Lyophilized | Reconstituted (2-8 °C) | Notes |
|---|---|---|---|
| Tirzepatide | 12+ months at -20 °C | 28-30 days | Standard for incretin-class peptides. |
| Cagrilintide | 12+ months at -20 °C | 28-30 days | Do not shake (amyloid fibril risk). Discard cloudy solution. |
Standard 7-Step Reconstitution
- 01
Warm up briefly
Let the lyophilized vial and BAC water reach room temperature (about 10-15 minutes).
- 02
Wipe the stoppers
Swab both vial stoppers with alcohol and let them dry.
- 03
Draw BAC water
Pull the planned BAC water volume into a sterile syringe.
- 04
Direct flow against the wall
Inject the BAC water slowly down the inside of the vial. Do not aim it at the powder. This matters more for cagrilintide than for tirzepatide.
- 05
Roll, do not shake
Swirl or roll gently until fully dissolved. Shaking can damage cagrilintide.
- 06
Confirm clarity
The solution should be clear and colorless. Cloudy or particulate solutions should be discarded.
- 07
Label and refrigerate
Mark the vial with compound name, concentration, and reconstitution date. Store at 2-8 °C. Use within 28-30 days.
Calculator
Running two-compound math with different mg scales? Use the PepPal Peptide Reconstitution Calculator and enter each compound separately for exact unit conversions.
Cagrilintide + Tirzepatide Side Effects & Safety
Each compound has its own safety profile. Tirzepatide has extensive Phase 3 and post-marketing safety data through Mounjaro and Zepbound. Cagrilintide has Phase 2 and CagriSema Phase 3 data. The exact combination has not been tested in humans, so the combined picture is built by adding each compound's known signals together.
Combined and Amplified Concerns
- Stacked GI side effects. Both compounds independently cause nausea, vomiting, diarrhea, and constipation - especially during dose increases. Running them together is expected to make these effects more frequent and more intense during the co-escalation phase (roughly weeks 9-20 in the staggered protocol). The staggered schedule is built to manage this; PepPal's guide covers protein, fiber, and electrolyte basics for GLP-1 users.
- Severely slowed digestion (gastroparesis risk). Both compounds slow how fast food leaves your stomach through different pathways. Layering both can slow digestion more than either one alone. Watch for feeling full long after eating small amounts, bloating, or acid reflux that worsens after starting the second compound. This is the most important theoretical risk of this specific stack.
- Injection-site reactions. More commonly tied to cagrilintide than tirzepatide. Rotate sites consistently across abdomen, thigh, and flank.
- Gallbladder events. Rapid weight loss raises gallstone risk regardless of which compounds drive the loss. Persistent upper-right abdominal pain after eating should be evaluated by a clinician.
- Pancreatitis (class warning). Tirzepatide carries a standard GLP-1 class warning about pancreatitis. Severe, persistent abdominal pain - especially pain that radiates to the back - is a reason to stop and seek medical attention.
- Sourcing quality. Tirzepatide can be obtained as an FDA-approved prescription drug (Mounjaro / Zepbound) or as research-use material. Cagrilintide is research-use only. Mixing an approved drug with an investigational compound is the standard safety position; sourcing both from research-grade suppliers raises contamination and label-accuracy risk. Verify both vials against a third-party COA when using research-grade supply. See the PepPal guide to reading COAs.
Common Community-Reported Side Effects
- Nausea, vomiting, diarrhea, constipation (worst during escalation steps).
- Injection-site redness or transient irritation (more common with cagrilintide).
- Mild fatigue during early titration.
- Strong appetite suppression - usually a feature, sometimes uncomfortable.
- Bloating or feeling overly full after small meals (delayed gastric emptying).
Contraindication Signals
Standard conservative practice excludes anyone with active gastrointestinal disease, type 1 diabetes, prior pancreatitis, medullary thyroid carcinoma history, or active cancer from any tirzepatide protocol. Adding cagrilintide raises the GI tolerance bar further.
When to reassess
If GI symptoms worsen instead of improving over the first 2-3 weeks of a step, if you cannot keep food down, or if you have severe persistent abdominal pain (especially with back radiation), pause and consult a qualified clinician. For broader stacking-safety context see the PepPal side-effects guide.
Cagrilintide + Tirzepatide Clinical Evidence Context
Direct stack evidence
No published human trial has tested cagrilintide + tirzepatide together. One preclinical study (Valdecantos et al., ADA 2024) showed combination benefit in obese rats. Beyond that, the evidence is per-compound plus the CagriSema (cag + sema) Phase 3 data as the closest human analog.
Tirzepatide
FDA-approved as Mounjaro for type 2 diabetes (2022) and Zepbound for obesity (2023). SURMOUNT-1 (Jastreboff et al., NEJM 2022) reported 22.5% body weight loss at 72 weeks at the 15 mg dose. REDEFINE-4 reported about 25.5% at 84 weeks in a head-to-head trial. This is the strongest single-agent obesity drug currently approved.
See the Tirzepatide protocol page for the standalone reference.
Cagrilintide
Phase 2 monotherapy (Lau et al., Lancet 2021) reported about 10.8% weight loss at 26 weeks at 4.5 mg. Phase 3 CagriSema (Garvey et al., NEJM 2025; REDEFINE-1) reported about 22.7% weight loss at 68 weeks when paired with semaglutide. CagriSema's NDA was filed with FDA in December 2025.
See the Cagrilintide protocol page for the standalone reference.
Preclinical Combination Data
Valdecantos et al. (Diabetes 2024; 73 Suppl 1: 300-OR) gave cagrilintide and tirzepatide together to obese rats. At sub-maximal doses, the combination produced greater weight reduction than either compound alone. Some metabolic markers also improved. This is the only direct combination evidence published as of June 2026.
Combined Stack
In plain terms, this stack hits weight loss from three directions: reduced appetite (GLP-1), better insulin signaling (GIP), and stronger fullness (amylin). It covers more pathways than CagriSema (which is missing GIP) but fewer than cag + retatrutide (which adds glucagon). The combination has one preclinical synergy paper but no human trial data of its own.
Cagrilintide + Tirzepatide Storage & Handling
Storage Reference (Both Compounds)
State
Lyophilized (long-term)
Tirzepatide
-4 °F (-20 °C), 12+ months
Cagrilintide
-4 °F (-20 °C), 12+ months
State
Lyophilized (short-term)
Tirzepatide
35.6-46.4 °F (2-8 °C), several months
Cagrilintide
35.6-46.4 °F (2-8 °C), several months
State
Reconstituted (liquid)
Tirzepatide
35.6-46.4 °F (2-8 °C), 28-30 days
Cagrilintide
35.6-46.4 °F (2-8 °C), 28-30 days
State
Color when reconstituted
Tirzepatide
Clear, colorless
Cagrilintide
Clear, colorless
State
Shake?
Tirzepatide
No - standard peptide handling
Cagrilintide
No - amyloid fibril risk
State
Light protection
Tirzepatide
Yes
Cagrilintide
Yes
State
Oral viable
Tirzepatide
No
Cagrilintide
No
| State | Tirzepatide | Cagrilintide |
|---|---|---|
| Lyophilized (long-term) | -4 °F (-20 °C), 12+ months | -4 °F (-20 °C), 12+ months |
| Lyophilized (short-term) | 35.6-46.4 °F (2-8 °C), several months | 35.6-46.4 °F (2-8 °C), several months |
| Reconstituted (liquid) | 35.6-46.4 °F (2-8 °C), 28-30 days | 35.6-46.4 °F (2-8 °C), 28-30 days |
| Color when reconstituted | Clear, colorless | Clear, colorless |
| Shake? | No - standard peptide handling | No - amyloid fibril risk |
| Light protection | Yes | Yes |
| Oral viable | No | No |
Both compounds share similar refrigerator windows. Cagrilintide is the more handling-sensitive of the two - never shake, and discard any cloudy solution.
Cagrilintide + Tirzepatide vs CagriSema vs Cagrilintide + Retatrutide
The two most common alternatives are CagriSema (the evidence-backed combination of cagrilintide + semaglutide) and cagrilintide + retatrutide (a broader but more speculative option). The table below shows how all three compare.
Receptor key: AMY = amylin receptors (fullness signaling). GLP-1R = appetite suppression. GIPR = insulin sensitivity / metabolic efficiency. GCGR = glucagon receptor (energy burn and fat oxidation).
How the cagrilintide + tirzepatide stack compares
Feature
Components
Cagrilintide + Tirzepatide
Cagrilintide + Tirzepatide
CagriSema (Cag + Sema)
Cagrilintide + Semaglutide
Cagrilintide + Retatrutide
Cagrilintide + Retatrutide
Feature
Receptor coverage
Cagrilintide + Tirzepatide
AMY + GLP-1R + GIPR (3 families)
CagriSema (Cag + Sema)
AMY + GLP-1R (2 families)
Cagrilintide + Retatrutide
AMY + GLP-1R + GIPR + GCGR (4 families)
Feature
Combination clinical data
Cagrilintide + Tirzepatide
Preclinical only (Valdecantos 2024)
CagriSema (Cag + Sema)
Phase 3 REDEFINE-1: ~22.7% at 68 weeks
Cagrilintide + Retatrutide
None (fully speculative)
Feature
Best monotherapy result
Cagrilintide + Tirzepatide
Tirzepatide: 25.5% at 84 weeks
CagriSema (Cag + Sema)
Semaglutide: ~14.9% at 68 weeks
Cagrilintide + Retatrutide
Retatrutide: 28.7% at 68 weeks
Feature
GIP receptor
Cagrilintide + Tirzepatide
Yes (tirzepatide)
CagriSema (Cag + Sema)
No
Cagrilintide + Retatrutide
Yes (retatrutide)
Feature
Glucagon receptor
Cagrilintide + Tirzepatide
No
CagriSema (Cag + Sema)
No
Cagrilintide + Retatrutide
Yes (retatrutide)
Feature
Dysesthesia risk
Cagrilintide + Tirzepatide
No
CagriSema (Cag + Sema)
No
Cagrilintide + Retatrutide
Yes (retatrutide)
Feature
FDA-approved component
Cagrilintide + Tirzepatide
Yes (tirzepatide as Mounjaro / Zepbound)
CagriSema (Cag + Sema)
Semaglutide approved; cag not
Cagrilintide + Retatrutide
Neither approved
Feature
Injections per week
Cagrilintide + Tirzepatide
2 (separate vials)
CagriSema (Cag + Sema)
1 or 2
Cagrilintide + Retatrutide
2 (separate) or 1 (pre-blend)
Feature
Estimated grey-market cost
Cagrilintide + Tirzepatide
$500-$1,000/month
CagriSema (Cag + Sema)
$500-$900/month
Cagrilintide + Retatrutide
$600-$1,200/month
| Feature | Cagrilintide + Tirzepatide | CagriSema (Cag + Sema) | Cagrilintide + Retatrutide |
|---|---|---|---|
| Components | Cagrilintide + Tirzepatide | Cagrilintide + Semaglutide | Cagrilintide + Retatrutide |
| Receptor coverage | AMY + GLP-1R + GIPR (3 families) | AMY + GLP-1R (2 families) | AMY + GLP-1R + GIPR + GCGR (4 families) |
| Combination clinical data | Preclinical only (Valdecantos 2024) | Phase 3 REDEFINE-1: ~22.7% at 68 weeks | None (fully speculative) |
| Best monotherapy result | Tirzepatide: 25.5% at 84 weeks | Semaglutide: ~14.9% at 68 weeks | Retatrutide: 28.7% at 68 weeks |
| GIP receptor | Yes (tirzepatide) | No | Yes (retatrutide) |
| Glucagon receptor | No | No | Yes (retatrutide) |
| Dysesthesia risk | No | No | Yes (retatrutide) |
| FDA-approved component | Yes (tirzepatide as Mounjaro / Zepbound) | Semaglutide approved; cag not | Neither approved |
| Injections per week | 2 (separate vials) | 1 or 2 | 2 (separate) or 1 (pre-blend) |
| Estimated grey-market cost | $500-$1,000/month | $500-$900/month | $600-$1,200/month |
Cost ranges reflect typical research-grade pricing as of June 2026 - verify supplier pricing before ordering. Tirzepatide cost varies a lot between research-grade and prescription Mounjaro / Zepbound channels.
Decision Guidance
- Choose cagrilintide + tirzepatide when you want the strongest single-agent base (tirzepatide is FDA-approved and outperforms semaglutide head-to-head) plus amylin layering. Good middle-ground option between CagriSema and cag + reta.
- Choose CagriSema when you want the strongest combination evidence. CagriSema is the only stack here with Phase 3 combo data and a pending FDA decision.
- Choose cagrilintide + retatrutide when you want maximum receptor coverage (four pathways instead of three) and you accept higher complexity and cost.
- Looking for a non-cagrilintide pairing? The retatrutide + MOTS-c stack swaps amylin satiety for mitochondrial AMPK support.
FAQ
Q1: Can you take cagrilintide and tirzepatide together?
Yes, but not on the same starting day. Standard community protocols run tirzepatide alone for the first 8 weeks (2.5 → 5 mg/week) to confirm GI tolerance, then add cagrilintide at 0.25 mg/week starting Week 9. Both compounds are once weekly. From Week 9 onward, most users dose both on the same day at different injection sites.
Q2: How much cagrilintide do you take with tirzepatide?
Most community protocols start cagrilintide at 0.25 mg/week once tirzepatide is established, then step up every 4 weeks to 0.5, 1.0, 1.7, and 2.4 mg/week. Tirzepatide titrates separately from 2.5 mg up to 15 mg/week. The full staggered schedule is in the dosing section.
Q3: How far apart should I inject cagrilintide and tirzepatide?
Most users inject both on the same day, a few minutes apart at different sites. There is no required time gap. Same day is simpler, but some users split them - tirzepatide Monday and cagrilintide Thursday - to spread out GI side effects during titration. Both compounds have half-lives around 5-8 days, so splitting by a few days does not change overall coverage much.
Q4: Can I inject cagrilintide and tirzepatide at the same port (same injection site)?
No. Use different injection sites for each compound - for example, tirzepatide in the abdomen and cagrilintide in the thigh or upper arm. Different sites reduce local irritation, lower the risk of stacked injection-site reactions, and help you tell which compound is causing any reaction. Never mix the two compounds in one syringe.
Q5: Can I inject cagrilintide and tirzepatide at the same time?
Yes - same time on the same day at different sites is the standard pattern. Most users inject one right after the other. There is no need to wait between injections.
Q6: Can I add cagrilintide after my second dose of tirzepatide?
Most community protocols wait longer than that - typically 8 weeks of tirzepatide alone before adding cagrilintide. Two doses is only 2 weeks in, which is not enough time to confirm GI tolerance or to settle into your titration step. Adding the second compound too early often leads to intense nausea and a forced step-down on one or both compounds.
Q7: When does cagrilintide appetite suppression kick in?
Cagrilintide has a long half-life (about 7-8 days), so it takes time to build up. Most users report noticeable appetite suppression by Week 2-3 after starting it. Some report changes within the first week. At the starting 0.25 mg/week dose, effects are usually mild. Stronger satiety effects typically appear after stepping up to 0.5-1.0 mg/week.
Q8: What is in a 5 mg / 5 mg cag/tirz blend vial?
A typical 5/5 pre-blend contains 5 mg cagrilintide + 5 mg tirzepatide = 10 mg total in one vial. Reconstituted with 2.0 mL bacteriostatic water, this gives 2.5 mg/mL of each compound. A 0.20 mL draw delivers 0.5 mg cag + 0.5 mg tirz. Pre-blends are less common for this stack than for cag/reta - separate vials are the standard.
Q9: How do you reconstitute cagrilintide and tirzepatide?
Reconstitute each vial separately with bacteriostatic water. A common setup is tirzepatide 10 mg + 1.0 mL BAC (= 10 mg/mL; a 5 mg dose = 0.50 mL = 50 units on a U-100 syringe) and cagrilintide 5 mg + 2.0 mL BAC (= 2.5 mg/mL; a 1 mg dose = 0.40 mL = 40 units). Inject BAC water slowly down the vial wall and swirl gently - never shake cagrilintide. Use the PepPal calculator for any custom vial size.
Q10: Is there any combination data for cagrilintide + tirzepatide?
Yes - one preclinical study. Valdecantos et al. (Diabetes 2024) gave both compounds to obese rats. The combination produced greater weight loss than either compound alone at sub-maximal doses. No human trial has tested the combination as of June 2026. CagriSema (cagrilintide + semaglutide) is the closest human analog with Phase 3 data.
Q11: How does this stack compare to CagriSema?
CagriSema pairs cagrilintide with semaglutide (a GLP-1-only drug). It has Phase 3 REDEFINE-1 data showing about 22.7% weight loss at 68 weeks, and an NDA was filed with FDA in December 2025. Cagrilintide + tirzepatide swaps semaglutide for tirzepatide, which adds GIP receptor activity. The cag + tirz combination covers three pathways instead of two, but it has no human trial data of its own.
Q12: What are the side effects of the cagrilintide + tirzepatide stack?
The biggest one is stacked GI side effects - nausea, vomiting, diarrhea, and constipation - because both compounds slow digestion. Cagrilintide is more likely to cause injection-site reactions. Tirzepatide carries a standard GLP-1 class warning for pancreatitis. Rapid weight loss raises gallstone risk. See the side effects section for the full breakdown.
Q13: How long should I run this stack?
Most community protocols use a 24-week staggered titration to reach maintenance, then run open-ended at maintenance with periodic re-evaluation. Tirzepatide trials (SURMOUNT-1) lasted 72 weeks. Some users cycle 16-24 weeks on, 4-8 weeks off. No validated cycle length exists for the combination specifically.
Q14: Can I use prescription Mounjaro or Zepbound with research-grade cagrilintide?
Theoretically yes - tirzepatide is the same active ingredient whether it is prescription (Mounjaro / Zepbound) or research-use. Some users pair their prescription tirzepatide with research-grade cagrilintide. This is an off-label combination that has not been studied directly. Talk to a qualified clinician before doing this, especially if your tirzepatide is prescribed for a specific condition.
Q15: Can I combine this stack with semaglutide, retatrutide, or pramlintide?
Generally no. Tirzepatide already covers GLP-1 (so semaglutide adds redundancy). Retatrutide also covers GLP-1 and GIP (the same receptors tirzepatide hits), so it overlaps. Pramlintide is a short-acting amylin analog, which cagrilintide already covers as a long-acting version. None of these adds new pathway coverage - they just stack side effects.
Q16: Is this medical advice?
No. Everything on this page is for educational and research-reference purposes only. Tirzepatide is FDA-approved (Mounjaro 2022, Zepbound 2023), but this specific combination with cagrilintide is not. Cagrilintide is investigational only as of June 2026. Consult a qualified healthcare provider before pursuing any peptide protocol.
Sources & Research
- 1. Valdecantos P, Rada P, Ghosh S, Rondinone CM, Valverde AM. 300-OR: Beneficial Effect of the Combination Therapy of Cagrilintide, a Dual Amylin/Calcitonin Agonist, and Tirzepatide, a Dual GLP-1/GIP Agonist, on Body Weight Loss in Obese Rats. Diabetes (2024)
- 2. Garvey WT, et al. Coadministered Cagrilintide and Semaglutide in Adults with Overweight or Obesity. New England Journal of Medicine (2025)
- 3. Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide Once Weekly for the Treatment of Obesity. New England Journal of Medicine (2022)
- 4. Lau DCW, Erichsen L, Francisco AM, et al. Once-weekly cagrilintide for weight management in people with overweight and obesity. The Lancet (2021)
- 5. Enebo LB, Berthelsen KK, Kankam M, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of concomitant administration of multiple doses of cagrilintide with semaglutide 2.4 mg. The Lancet (2021)
- 6. Kruse T, Dahl K, Schaffer L, et al. Development of Cagrilintide, a Long-Acting Amylin Analogue. Journal of Medicinal Chemistry (2021)
- 7. Garvey WT, Frias JP, Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity in people with type 2 diabetes (SURMOUNT-2). The Lancet (2023)
- 8. Dutta D, et al. Efficacy and Safety of Cagrilintide Alone and in Combination with Semaglutide as Anti-Obesity Medications: A Systematic Review and Meta-Analysis. Indian Journal of Endocrinology and Metabolism (2024)
- 9. U.S. Food and Drug Administration FDA Approves New Medication for Chronic Weight Management (Zepbound / tirzepatide). FDA.gov (2023)
- 10. Fletcher MM, et al. Structural and dynamic features of cagrilintide binding to calcitonin and amylin receptors. Nature Communications (2025)
- 11. ClinicalTrials.gov REDEFINE 1 - Cagrilintide and Semaglutide in Adults with Overweight or Obesity. NCT05567796. ClinicalTrials.gov (2025)
- 12. ClinicalTrials.gov SURMOUNT-1 - Tirzepatide Once Weekly in Adults with Obesity. NCT04184622. ClinicalTrials.gov (2022)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page