CJC-1295 with DAC Quick Start
CJC-1295 with DAC is a 30-amino acid GHRH analog with a Drug Affinity Complex (DAC) modification at position 30 that lets the peptide attach to circulating albumin. That albumin binding shields it from breakdown and stretches its half-life from minutes (the No DAC version) to about 6-8 days. In plain English: one injection keeps signaling the pituitary to release growth hormone for nearly a week.
It is also called DAC:GRF and was developed by ConjuChem Biotechnologies. It reached Phase 2 development for HIV lipodystrophy in 2006 before that trial was halted. As of June 2026, CJC-1295 with DAC is not FDA-approved and has no active approval pathway.
Route
Subcutaneous injection. Reconstitute lyophilized powder with bacteriostatic water before use.
Schedule
Common research-planning cadence is once weekly. Some protocols split into two doses (Mon/Thu).
Measure
Use vial concentration and U-100 insulin syringe units. 10 mg vial + 3.0 mL BAC water = about 3,333 mcg/mL.
Supplies
BAC water, U-100 insulin syringes, alcohol swabs, and refrigerated storage for the reconstituted vial.
Research status
Investigational. Phase 2 was halted in 2006 after a participant cardiovascular death attributed to pre-existing disease.
Disclaimer
This page is an educational research reference and is not medical advice. CJC-1295 with DAC is investigational. No compound on this site is intended for human consumption. Consult a qualified healthcare professional before considering any peptide protocol.
Use this protocol for dosing, vial mixing, and schedule planning. For the full background, read the CJC-1295 peptide guide on how it works, research, side effects, and legal status.
CJC-1295 with DAC Dosing Protocol & Schedule
Common research-planning ranges land between 1-2 mg subcutaneously once weekly. Because the half-life is 6-8 days, the compound takes roughly 3-4 weeks to reach steady state. Conservative starting doses give time to assess tolerance before any escalation.
CJC-1295 with DAC weekly dosing schedule
Phase
Initiation
Window
Weeks 1-2
Weekly dose
500-1,000 mcg once weekly
Notes
Start low to assess tolerance. Evening administration is common in protocol planning.
Phase
Therapeutic range
Window
Weeks 3-8
Weekly dose
1,000 mcg once weekly
Notes
Most common maintenance dose in research and community workflows.
Phase
Elevated dose
Window
Weeks 3-12
Weekly dose
2,000 mcg once weekly or 1 mg twice weekly
Notes
Some protocols split the weekly dose for a smoother GH/IGF-1 profile.
Phase
Maximum studied
Window
Phase 2 trial
Weekly dose
Up to 240 mcg/kg/week
Notes
HIV lipodystrophy protocol used weight-based dosing far above community ranges.
| Phase | Window | Weekly dose | Notes |
|---|---|---|---|
| Initiation | Weeks 1-2 | 500-1,000 mcg once weekly | Start low to assess tolerance. Evening administration is common in protocol planning. |
| Therapeutic range | Weeks 3-8 | 1,000 mcg once weekly | Most common maintenance dose in research and community workflows. |
| Elevated dose | Weeks 3-12 | 2,000 mcg once weekly or 1 mg twice weekly | Some protocols split the weekly dose for a smoother GH/IGF-1 profile. |
| Maximum studied | Phase 2 trial | Up to 240 mcg/kg/week | HIV lipodystrophy protocol used weight-based dosing far above community ranges. |
Trial-context ranges are reported for reference only. This is not a dosing recommendation.
Cycle structure
Cycle guidelines
Approach
Standard
Cycle length
8-12 weeks
Off period
4-6 weeks
Best for
General research planning to limit desensitization risk.
Approach
Extended
Cycle length
12-16 weeks
Off period
6-8 weeks
Best for
Longer-research-window contexts where steady-state IGF-1 is the target.
Approach
Split-dose
Cycle length
8-12 weeks
Off period
4-6 weeks
Best for
1 mg twice weekly for a smoother GH/IGF-1 envelope.
| Approach | Cycle length | Off period | Best for |
|---|---|---|---|
| Standard | 8-12 weeks | 4-6 weeks | General research planning to limit desensitization risk. |
| Extended | 12-16 weeks | 6-8 weeks | Longer-research-window contexts where steady-state IGF-1 is the target. |
| Split-dose | 8-12 weeks | 4-6 weeks | 1 mg twice weekly for a smoother GH/IGF-1 envelope. |
Cycle structures reflect community research planning, not approved clinical use.
Practical timing notes. Once-weekly dosing is pharmacokinetically sufficient given the 6-8 day half-life, so timing is less sensitive than with No DAC. Evening dosing remains common in research planning. If a dose is missed, common community practice is to dose as soon as remembered unless the next scheduled dose is within about two to three days.
CJC-1295 with DAC Supplies Needed
Supply math below assumes 1 mg once weekly from a 10 mg vial reconstituted with up to 3.0 mL BAC water (about 3,333 mcg/mL). Adjust vial counts if running 2 mg/week or split twice-weekly dosing.
Recommended USA Supply
Use discount code SAVE10 at Peptira checkout. See why we love Peptira.
CJC-1295 DAC Supply

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials
Assumes 1 mg/week from a 10 mg vial; adjust counts if running 2 mg/week or split twice-weekly dosing.
| Cycle length | Planning note |
|---|---|
4-8 weeks 1 vial | 4 weeks: 10 mg vial covers about 10 weekly 1 mg doses.; 8 weeks: 8 weekly doses with about 2 mg remaining as margin. |
12-16 weeks 2 vials | 12 weeks: 12 weekly doses require a second vial after week 10.; 16 weeks: 16 weekly doses with margin for reconstitution loss. |
4-8 weeks
1 vial
4 weeks: 10 mg vial covers about 10 weekly 1 mg doses.; 8 weeks: 8 weekly doses with about 2 mg remaining as margin.
12-16 weeks
2 vials
12 weeks: 12 weekly doses require a second vial after week 10.; 16 weeks: 16 weekly doses with margin for reconstitution loss.
Insulin Syringes (U-100)
0.3 mL / 30-unit syringes align cleanly with a 1 mg dose when a 10 mg vial is mixed with 3.0 mL BAC water (30 units).
| Cycle length | Planning note |
|---|---|
4 weeks 4 syringes | 1 syringe per weekly injection. |
8 weeks 8 syringes | 1 per week; recommend a 10-pack with margin. |
12 weeks 12 syringes | 1 per week; double if dosing twice weekly. |
16 weeks 16 syringes | Round up for dropped or damaged syringes. |
4 weeks
4 syringes
1 syringe per weekly injection.
8 weeks
8 syringes
1 per week; recommend a 10-pack with margin.
12 weeks
12 syringes
1 per week; double if dosing twice weekly.
16 weeks
16 syringes
Round up for dropped or damaged syringes.
Bacteriostatic Water
Use no more than 3.0 mL per 10 mg vial for the baseline math on this page (other concentrations work; see reconstitution table).
| Cycle length | Planning note |
|---|---|
4-16 weeks 1 x 10 mL bottle | 4 weeks: 1 vial uses up to 3.0 mL; bottle gives ample margin.; 8 weeks: 1 vial uses up to 3.0 mL total.; 12 weeks: 2 vials use up to 6.0 mL total.; 16 weeks: 2 vials use up to 6.0 mL total; add a second bottle only if running higher-dose vial counts. |
4-16 weeks
1 x 10 mL bottle
4 weeks: 1 vial uses up to 3.0 mL; bottle gives ample margin.; 8 weeks: 1 vial uses up to 3.0 mL total.; 12 weeks: 2 vials use up to 6.0 mL total.; 16 weeks: 2 vials use up to 6.0 mL total; add a second bottle only if running higher-dose vial counts.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments. Double syringe and swab counts if running a split twice-weekly schedule.
Companion Supplies & Routine Support
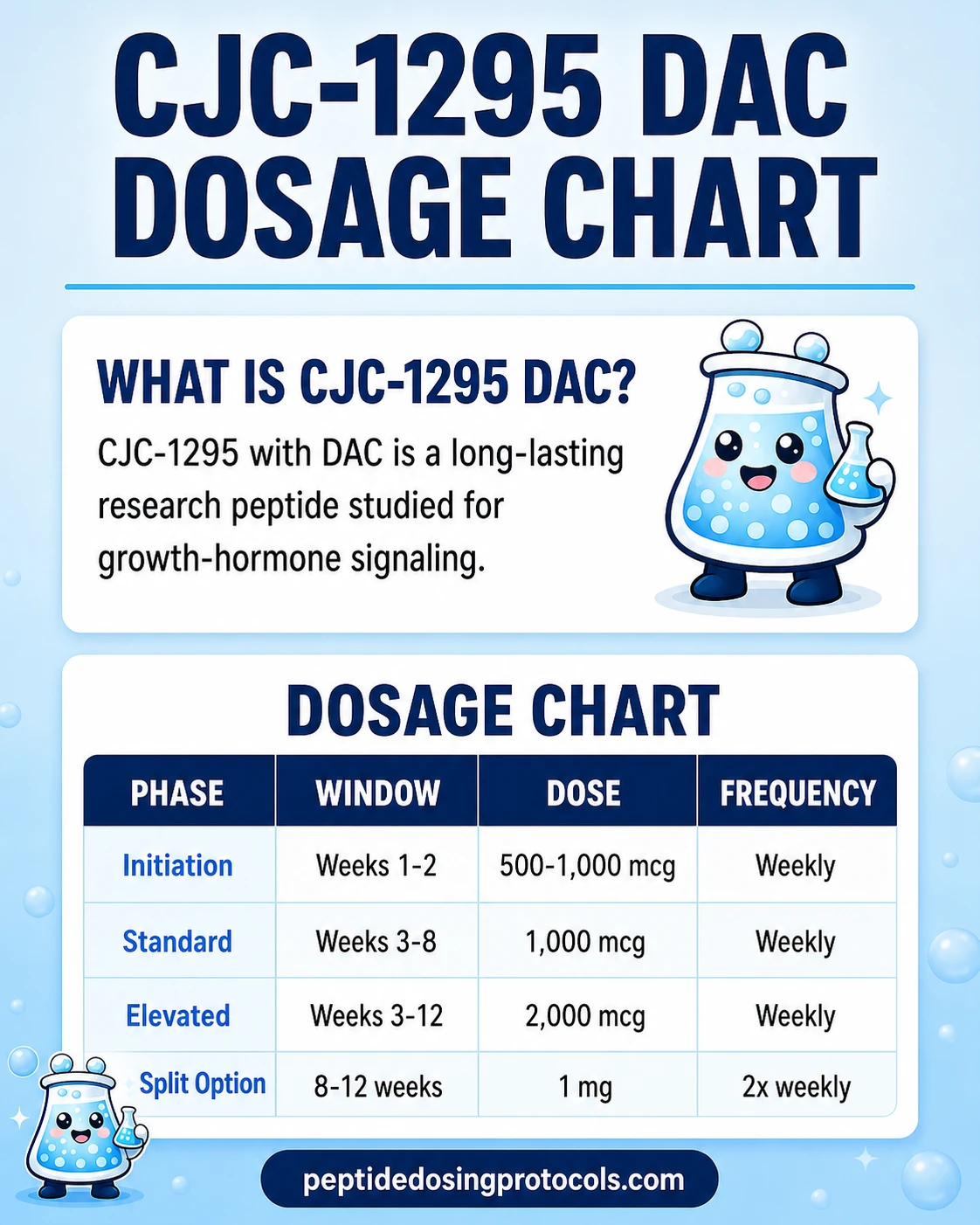
CJC-1295 DAC Dosage Chart
This CJC-1295 DAC dosage chart summarizes the weekly research dosing ranges from 500 mcg to 2,000 mcg shown in the dosing section above.
CJC-1295 with DAC Reconstitution Guide
The table below assumes a 10 mg vial and shows BAC water volumes up to 3.0 mL, with the resulting concentration and U-100 syringe units at typical weekly doses. 'Units' refers to the markings on a U-100 insulin syringe, where 100 units equals 1.0 mL.
CJC-1295 with DAC reconstitution and syringe math
Vial size
10 mg
BAC water added
1.0 mL
Concentration
10,000 mcg/mL
500 mcg
0.05 mL (5 units)
1,000 mcg
0.10 mL (10 units)
2,000 mcg
0.20 mL (20 units)
Vial size
10 mg
BAC water added
2.0 mL
Concentration
5,000 mcg/mL
500 mcg
0.10 mL (10 units)
1,000 mcg
0.20 mL (20 units)
2,000 mcg
0.40 mL (40 units)
Vial size
10 mg
BAC water added
3.0 mL
Concentration
~3,333 mcg/mL
500 mcg
0.15 mL (15 units)
1,000 mcg
0.30 mL (30 units)
2,000 mcg
0.60 mL (60 units)
| Vial size | BAC water added | Concentration | 500 mcg | 1,000 mcg | 2,000 mcg |
|---|---|---|---|---|---|
| 10 mg | 1.0 mL | 10,000 mcg/mL | 0.05 mL (5 units) | 0.10 mL (10 units) | 0.20 mL (20 units) |
| 10 mg | 2.0 mL | 5,000 mcg/mL | 0.10 mL (10 units) | 0.20 mL (20 units) | 0.40 mL (40 units) |
| 10 mg | 3.0 mL | ~3,333 mcg/mL | 0.15 mL (15 units) | 0.30 mL (30 units) | 0.60 mL (60 units) |
Units assume a U-100 insulin syringe. The table caps BAC water at 3.0 mL for a 10 mg vial. Use the calculator below to confirm exact draw volume for any custom mix.
Step-by-step reconstitution
- 01
Gather supplies
CJC-1295 with DAC vial, bacteriostatic water, alcohol swabs, and a U-100 insulin syringe.
- 02
Inspect the vial
Check label, lot, and concentration. The lyophilized powder should look intact, not melted or discolored.
- 03
Clean stoppers
Wipe both stoppers with separate alcohol swabs and let them dry completely.
- 04
Draw bacteriostatic water
Pull the planned BAC water volume from the table above into a syringe.
- 05
Add water slowly
Inject the BAC water down the inside vial wall, not directly onto the powder, to limit foaming.
- 06
Mix gently
Swirl or roll the vial. Do not shake vigorously. The solution should be clear and colorless with no particles.
- 07
Label and store
Mark the vial with concentration and date, then refrigerate at 35.6-46.4F (2-8C). Use within 3-4 weeks.
Need exact units for a custom vial?
Use the PepPal peptide reconstitution calculator to confirm syringe units for any vial size and BAC water volume.
How CJC-1295 with DAC Works
CJC-1295 with DAC tells the pituitary gland to release more growth hormone, and the DAC modification keeps that signal active for days instead of minutes. The peptide shares the same 29-amino acid GHRH-analog core as CJC-1295 No DAC, with stabilizing substitutions at positions 2, 8, 15, and 27. The DAC version adds a maleimidopropionyl group at position 30 that latches onto albumin in the blood. Albumin then acts as a carrier protein that shields the peptide from breakdown and kidney filtration.
GHRH receptor activation
CJC-1295 with DAC binds to GHRH receptors on somatotroph cells in the pituitary, triggering a cAMP signaling cascade that drives growth hormone production and release. Receptor-binding activity is identical to CJC-1295 No DAC. The DAC modification only changes how long the peptide stays in circulation, not how strongly it stimulates the receptor.
Albumin bioconjugation and extended half-life
Once injected, the DAC component reacts with albumin in the bloodstream and binds covalently. That albumin tether is the entire reason the half-life stretches from about 30 minutes (No DAC) to roughly 5.8-8.1 days, as reported in the Phase 1 PK data from Teichman et al. (2006). I verified that half-life range against the JCEM paper directly.
Sustained GH and IGF-1 elevation
In Phase 1 data, a single CJC-1295 with DAC injection raised growth hormone roughly 2-10 fold for at least 6 days and IGF-1 about 1.5-3 fold for 9-11 days. With repeated weekly dosing, IGF-1 elevation accumulated and lasted up to 28 days. A companion analysis (Ionescu and Frohman, 2006) reported that the body's natural pulsatile GH rhythm was preserved even with DAC on board, which suggests sustained exposure does not completely flatten the natural release pattern.
Downstream IGF-1 pathway
When growth hormone stays elevated, the liver produces more IGF-1, which is the main mediator of GH's effects on tissues. Sustained IGF-1 supports protein synthesis, collagen turnover, lipolysis, and tissue repair signaling. The steady IGF-1 envelope from DAC differs from the shorter pulse profile produced by No DAC.
Who CJC-1295 with DAC Is For and Who Should Avoid It
CJC-1295 with DAC is investigational. Even in research planning, common screening protocols exclude several groups based on the known biology of GHRH analogs and the cardiovascular signal that ended Phase 2 development.
- Active or recent malignancy: GH/IGF-1 elevation is generally avoided in cancer contexts.
- Significant cardiovascular disease: the halted Phase 2 trial saw a participant cardiovascular death attributed to pre-existing coronary disease.
- Diabetes or pre-diabetes: GH elevation can affect insulin sensitivity.
- Pregnancy or lactation: no human safety data.
- Known peptide hypersensitivity.
- Anyone without qualified clinician oversight, especially given the long half-life and persistence of any adverse effects.
Long half-life implication
Because CJC-1295 with DAC stays active for 6-8 days, any adverse effect can persist for days rather than clearing in hours. That makes professional oversight especially important.
CJC-1295 with DAC Side Effects & Safety
Phase 1 data described CJC-1295 with DAC as relatively well tolerated at lower dose ranges, with adverse events increasing at higher exposure. The most important safety signal in the published record came from the halted Phase 2 trial.
Reported adverse events
- Injection-site reactions: pain, redness, itching, induration (lumps under the skin), and swelling.
- Temporary flushing or warmth from blood vessel dilation.
- Headache.
- Gastrointestinal symptoms such as nausea.
- Water retention, particularly at higher doses.
- Numbness or tingling in extremities reported in some cohorts.
Dose-dependent pattern
Higher dose cohorts showed more frequent tolerability issues. Lower 30-60 mcg/kg ranges were reported as better tolerated in Phase 1. Phase 1 studies reported no discontinuations for adverse events and no serious adverse events in those cohorts.
DAC-specific consideration
Because the half-life is 6-8 days, side effects can persist for days rather than minutes. That is the most important practical difference from shorter-acting GHRH analogs.
Phase 2 cardiovascular signal
A 2006 Phase 2 HIV lipodystrophy trial (NCT00267527) was halted after one participant died from a myocardial infarction. The attending physician attributed the death to pre-existing coronary disease rather than the study drug. ConjuChem discontinued development as a precaution. As of June 2026, there is no active FDA approval pathway.
Cross-class safety context
For a broader peptide side-effect overview, see the PepPal Peptide Side Effects Guide.
CJC-1295 with DAC Timeline & What to Monitor
Because the half-life is 6-8 days, exposure builds gradually. Steady state takes roughly 3-4 weeks. The Phase 1 record gives the clearest picture of when measurable changes appear.
Reported timeline from the published record
Window
0-6 days post single dose
What was measured
GH elevated 2-10 fold (Teichman 2006).
Window
0-9 to 11 days post single dose
What was measured
IGF-1 elevated 1.5-3 fold (Teichman 2006).
Window
Weeks 3-4 of weekly dosing
What was measured
Approximate steady state for IGF-1.
Window
Through 28 days of weekly dosing
What was measured
Cumulative IGF-1 elevation reported.
| Window | What was measured |
|---|---|
| 0-6 days post single dose | GH elevated 2-10 fold (Teichman 2006). |
| 0-9 to 11 days post single dose | IGF-1 elevated 1.5-3 fold (Teichman 2006). |
| Weeks 3-4 of weekly dosing | Approximate steady state for IGF-1. |
| Through 28 days of weekly dosing | Cumulative IGF-1 elevation reported. |
Trial-context findings only. This is not a dosing recommendation or a promise of personal outcomes.
What people commonly ask about
Community reports over 8-12 week cycles often describe better recovery between sessions, deeper sleep, gradual changes in body composition, and skin or connective tissue feel. None of those endpoints were tested in controlled long-term trials, so they should be treated as anecdotal context, not expected results.
What is reasonable to monitor
- IGF-1 (baseline, mid-cycle, and end of cycle) under clinician oversight.
- Fasting glucose and HbA1c, given the GH/insulin-sensitivity interaction.
- Blood pressure and resting heart rate during cycles.
- Subjective tolerability: injection-site reactions, water retention, paresthesia.
If unwanted effects appear, common research-planning practice is to pause and re-evaluate before continuing, especially because the long half-life means effects can persist for days.
CJC-1295 with DAC Clinical Evidence Context
Direct human evidence on CJC-1295 with DAC comes from a small cluster of Phase 1 trials, a halted Phase 2 trial, and supporting preclinical work, all published between 2005 and 2009. I verified the Phase 1 PK numbers cited below against the Teichman et al. JCEM paper directly.
Human evidence (Phase 1)
Teichman et al. 2006 (JCEM): single ascending dose and multiple-dose Phase 1 in healthy adults. Reported half-life of 5.8-8.1 days, GH elevation 2-10 fold for 6+ days, IGF-1 elevation 1.5-3 fold for 9-11 days, and cumulative IGF-1 elevation up to 28 days with repeated weekly dosing.
Human evidence (pulsatility)
Ionescu and Frohman 2006 (JCEM): companion overnight PK analysis in healthy men. Reported preserved pulsatile GH secretion with CJC-1295 on board, trough GH +7.5 fold, mean GH +46%, and IGF-1 +45%.
Human evidence (Phase 2, halted)
ConjuChem Phase 2 HIV lipodystrophy trial (NCT00267527): 192 patients, dose-escalation up to 240 mcg/kg/week, halted in 2006 after one participant cardiovascular death attributed by the attending physician to pre-existing coronary disease.
Preclinical evidence
Jette et al. 2005 in rats identified CJC-1295 as a long-lasting GRF analog. Alba et al. 2006 showed daily CJC-1295 normalized growth and somatotroph proliferation in GHRH-knockout mice.
Mechanism follow-up
Sackmann-Sala et al. 2009 reported serum protein profile changes consistent with GH/IGF-1 axis activation in adults receiving CJC-1295.
Evidence gap
No modern Phase 2 or Phase 3 trials are registered for CJC-1295 with DAC as of June 2026. There is no FDA approval pathway and no long-term controlled human safety data beyond the 2006 program.
CJC-1295 with DAC Storage & Handling
Storage reference
State
Lyophilized (powder)
Storage
-4F (-20C) or below long-term
Shelf life
12-24+ months per supplier label
State
Lyophilized (powder)
Storage
35.6-46.4F (2-8C)
Shelf life
Several months per supplier label
State
Lyophilized (powder)
Storage
Room temperature
Shelf life
Weeks (shipping window only)
State
Reconstituted (liquid)
Storage
35.6-46.4F (2-8C)
Shelf life
3-4 weeks typical research-planning window
State
Reconstituted (frozen aliquots)
Storage
-4F (-20C)
Shelf life
About 3-4 months
| State | Storage | Shelf life |
|---|---|---|
| Lyophilized (powder) | -4F (-20C) or below long-term | 12-24+ months per supplier label |
| Lyophilized (powder) | 35.6-46.4F (2-8C) | Several months per supplier label |
| Lyophilized (powder) | Room temperature | Weeks (shipping window only) |
| Reconstituted (liquid) | 35.6-46.4F (2-8C) | 3-4 weeks typical research-planning window |
| Reconstituted (frozen aliquots) | -4F (-20C) | About 3-4 months |
Use supplier label and stability data when available. Do not refer to this table as a clinical beyond-use date.
- Protect from light.
- Avoid repeated freeze-thaw cycles, which can degrade DAC peptide integrity.
- Use bacteriostatic water (not sterile water) for multi-dose vials.
- Discard cloudy or discolored solutions.
CJC-1295 with DAC Protocol Mistakes & Troubleshooting
Most practical issues with weekly DAC protocols come from the long half-life, the relatively small once-weekly draw volume, and reconstitution math that differs from daily peptides.
- 01
Missed dose
Common community practice is to dose as soon as remembered, unless the next scheduled dose is within about 2-3 days, then resume the regular schedule.
- 02
Cloudy or discolored vial
Discard. CJC-1295 with DAC should reconstitute clear and colorless.
- 03
Wrong BAC water volume
Recalculate concentration first. The vial is still usable; you only need to update your draw volume to match the new mg/mL using the reconstitution table.
- 04
Side effects feel too strong
Pause before the next weekly dose and reassess with a clinician. Long half-life means dose escalation has a delayed, persistent footprint.
- 05
Persistent injection-site lump
Rotate sites, reassess injection technique, and consider a clinician review. Persistent indurations should not be ignored.
- 06
Storage mistake
Reconstituted vial left at room temperature for hours can usually be returned to refrigeration, but a vial left out overnight or longer is generally discarded.
- 07
Confused DAC vs No DAC
DAC is once weekly. No DAC is daily or multiple times daily. Always confirm the vial label and supplier listing before reconstituting.
CJC-1295 with DAC Regulatory Status
As of June 2026, CJC-1295 with DAC is not FDA-approved for any indication. Phase 2 development for HIV lipodystrophy was discontinued in 2006 after the trial was halted, and no active modern Phase 2 or Phase 3 trials are registered on ClinicalTrials.gov.
- FDA: not approved; included in the FDA Category 2 bulk drug substances review record (FDA-2024-N-4777-0009).
- EMA: not approved.
- ClinicalTrials.gov: NCT00267527 marked terminated; no active modern registrations identified at the June 2026 review.
- Compounding pharmacy access: limited and regulator-dependent. CJC-1295 with DAC is not on the FDA's approved-bulk-substance list for 503A compounding.
All product references on this page are research-use-only and are not for human consumption.
CJC-1295 with DAC vs CJC-1295 No DAC vs Tesamorelin vs Ipamorelin
The biggest practical differences between CJC-1295 with DAC and its closest comparators are half-life and dosing cadence. Tesamorelin is the only FDA-approved compound in the table below, with an indication for HIV lipodystrophy.
GH-secretagogue comparison
Feature
Class
CJC-1295 with DAC
Long-acting GHRH analog (albumin-binding)
CJC-1295 No DAC
GHRH analog
Tesamorelin
GHRH analog
Ipamorelin
GHRP (ghrelin mimetic)
Feature
Half-life
CJC-1295 with DAC
6-8 days
CJC-1295 No DAC
~30 minutes
Tesamorelin
~26 minutes
Ipamorelin
~2 hours
Feature
Dosing frequency
CJC-1295 with DAC
1-2x per week
CJC-1295 No DAC
1-3x daily
Tesamorelin
Once daily
Ipamorelin
1-3x daily
Feature
Common dose range
CJC-1295 with DAC
1,000-2,000 mcg per week
CJC-1295 No DAC
100-300 mcg per injection
Tesamorelin
1-2 mg daily (FDA label)
Ipamorelin
100-300 mcg per injection
Feature
GH pattern
CJC-1295 with DAC
Sustained elevation
CJC-1295 No DAC
Pulsatile
Tesamorelin
Pulsatile
Ipamorelin
Brief pulse
Feature
FDA status
CJC-1295 with DAC
Not approved
CJC-1295 No DAC
Not approved
Tesamorelin
FDA-approved (HIV lipodystrophy)
Ipamorelin
Not approved
Feature
Practical advantage
CJC-1295 with DAC
Weekly cadence; strongest long-acting PK
CJC-1295 No DAC
Faster titration; physiologic pulses
Tesamorelin
Only approved GHRH analog
Ipamorelin
Selective GH pulse with minimal cortisol/prolactin impact
| Feature | CJC-1295 with DAC | CJC-1295 No DAC | Tesamorelin | Ipamorelin |
|---|---|---|---|---|
| Class | Long-acting GHRH analog (albumin-binding) | GHRH analog | GHRH analog | GHRP (ghrelin mimetic) |
| Half-life | 6-8 days | ~30 minutes | ~26 minutes | ~2 hours |
| Dosing frequency | 1-2x per week | 1-3x daily | Once daily | 1-3x daily |
| Common dose range | 1,000-2,000 mcg per week | 100-300 mcg per injection | 1-2 mg daily (FDA label) | 100-300 mcg per injection |
| GH pattern | Sustained elevation | Pulsatile | Pulsatile | Brief pulse |
| FDA status | Not approved | Not approved | FDA-approved (HIV lipodystrophy) | Not approved |
| Practical advantage | Weekly cadence; strongest long-acting PK | Faster titration; physiologic pulses | Only approved GHRH analog | Selective GH pulse with minimal cortisol/prolactin impact |
Sustained exposure makes adverse effects harder to reverse and may raise desensitization concerns over long cycles. Reconstitution math differs across compounds; verify before any planning.
CJC-1295 No DAC
Same GHRH-analog core; dosed daily for a pulsatile profile. See the CJC-1295 No DAC protocol.
Tesamorelin
FDA-approved GHRH analog for HIV lipodystrophy. See the tesamorelin protocol.
Ipamorelin
GHRP that pairs with GHRH analogs in many GH-pulse stacks. See the ipamorelin protocol.
CJC-1295 DAC Blood Tests & Monitoring
CJC-1295 DAC is discussed as a longer-acting GH-axis research peptide. Monitoring centers on IGF-1, glucose handling, lipids, thyroid context, and fluid-retention symptoms.
Blood test markers to discuss with a clinician
Marker
IGF-1
Why it matters
Shows the downstream signal after GH-axis stimulation and helps frame whether the pathway is being pushed harder.
Timing
Follow-up
Marker
A1c
Why it matters
Tracks longer-term glucose control because GH-axis stimulation may affect insulin sensitivity.
Timing
Baseline
Marker
Fasting glucose
Why it matters
Gives a current glucose snapshot before and during GH-axis changes.
Timing
Follow-up
Marker
Lipid panel
Why it matters
Reviews cholesterol and triglyceride trends that may shift with GH-axis activity and body composition changes.
Timing
Baseline
Marker
TSH and free T4
Why it matters
Adds thyroid context because thyroid status can affect energy, weight, and GH-axis interpretation.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| IGF-1 | Shows the downstream signal after GH-axis stimulation and helps frame whether the pathway is being pushed harder. | Follow-up |
| A1c | Tracks longer-term glucose control because GH-axis stimulation may affect insulin sensitivity. | Baseline |
| Fasting glucose | Gives a current glucose snapshot before and during GH-axis changes. | Follow-up |
| Lipid panel | Reviews cholesterol and triglyceride trends that may shift with GH-axis activity and body composition changes. | Baseline |
| TSH and free T4 | Adds thyroid context because thyroid status can affect energy, weight, and GH-axis interpretation. | Optional |
Monitoring guidance is GH-axis and IGF-1 pathway-based, supported by human CJC-1295 data showing GH and IGF-1 increases.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with diabetes risk, cancer history, sleep apnea, edema, carpal tunnel symptoms, or thyroid disease.
Follow-up
Re-check IGF-1 and metabolic markers after 6-8 weeks or after meaningful dose changes.
Longer term
For longer use, review GH-axis and metabolic trends every 3-6 months with a clinician.
How to interpret the labs
- IGF-1 should be interpreted against age, symptoms, and baseline values rather than as a stand-alone target.
- Fluid retention, numbness, joint pain, sleep apnea symptoms, and glucose changes matter during GH-axis protocols.
- Cancer history or active malignancy concerns need clinician review before GH-axis stimulation is considered.
Do not wait for routine labs
Rapid fluid retention, shortness of breath, severe headaches, vision changes, or new neurologic symptoms need medical review. New or worsening numbness, carpal tunnel symptoms, or sleep apnea symptoms should be discussed with a clinician.
FAQ
Q1: What is the starting dose of CJC-1295 with DAC?
Most research-planning protocols start at 500-1,000 mcg (0.5-1 mg) once weekly by subcutaneous injection. Conservative starts are common because the 6-8 day half-life means side effects can persist for days. This is not a dosing recommendation; see Peptide Dosing Protocols for full reference context.
Q2: What is CJC-1295 with DAC's half-life?
Estimated half-life is approximately 5.8-8.1 days based on Phase 1 PK data from Teichman et al. (2006). The DAC modification enables albumin binding, which extends activity far beyond CJC-1295 No DAC (about 30 minutes) and native GHRH (about 7 minutes).
Q3: What results were reported in CJC-1295 with DAC trials?
Phase 1 data reported growth hormone elevation roughly 2-10 fold for at least 6 days and IGF-1 elevation 1.5-3 fold for 9-11 days from a single dose, with cumulative IGF-1 elevation lasting up to 28 days during weekly dosing. These are trial findings, not promised personal outcomes.
Q4: How is CJC-1295 with DAC reconstituted?
A 10 mg vial reconstituted with 3.0 mL bacteriostatic water yields about 3,333 mcg/mL, where a 1 mg dose equals 30 units on a U-100 syringe. For other BAC water volumes up to 3.0 mL, see the reconstitution table above or use the PepPal calculator.
Q5: Is CJC-1295 with DAC FDA-approved?
No. As of June 2026, CJC-1295 with DAC is not FDA-approved. Phase 2 development was discontinued in 2006 after the HIV lipodystrophy trial was halted, and there is no active approval pathway.
Q6: What are the most common side effects?
Most reported effects include injection-site reactions, flushing, headache, GI symptoms, and water retention. Because the half-life is 6-8 days, adverse effects can persist longer than with shorter-acting GHRH analogs. The 2006 Phase 2 trial was halted after a participant cardiovascular death attributed by the attending physician to pre-existing coronary disease.
Q7: How does CJC-1295 with DAC compare to CJC-1295 No DAC?
Receptor activity is essentially identical because both share the same GHRH-analog core. The DAC version extends the half-life from about 30 minutes to 6-8 days, which enables weekly dosing but produces sustained exposure. No DAC requires daily or multi-daily injections and is easier to titrate quickly. See CJC-1295 No DAC for the daily-dosing comparison.
Q8: What vial sizes are available for CJC-1295 with DAC?
This page's planning math assumes a 10 mg research vial. At 1 mg per week, a 10 mg vial typically covers about ten weekly doses depending on priming loss and the exact BAC water volume used.
Q9: How much bacteriostatic water should be added?
For the 10 mg vial baseline on this page, examples use 1.0, 2.0, or 3.0 mL BAC water, with 3.0 mL as the maximum shown. Choose the volume that gives clean U-100 syringe-unit math for the target weekly dose. The PepPal calculator confirms exact draw volumes.
Q10: What is the maximum dose studied in trials?
Phase 1 single-dose exposure went up to 250 mcg/kg, and the halted Phase 2 protocol used weekly weight-based dosing up to 240 mcg/kg/week. These ranges are far above the 1-2 mg/week common in research-planning workflows. This is not a dosing recommendation.
Q11: How should reconstituted CJC-1295 with DAC be stored?
Store reconstituted solution refrigerated at 35.6-46.4F (2-8C) and generally use within 3-4 weeks. For longer storage, frozen single-use aliquots at -4F (-20C) are typical to avoid repeated freeze-thaw cycles.
Q12: What clinical trials have been conducted on CJC-1295 with DAC?
Published data includes two Phase 1 randomized controlled studies and a pulsatility companion analysis (all 2006), plus the halted Phase 2 HIV lipodystrophy trial NCT00267527. No active modern trials are registered as of June 2026.
Q13: Where can I calculate reconstitution and syringe units?
Use the PepPal reconstitution calculator for exact dose-to-unit conversions across vial size and BAC water volume.
Q14: Is this page medical advice?
No. Peptide Dosing Protocols pages are educational research references. CJC-1295 with DAC is investigational and not approved for human use. Consult a qualified clinician before considering any peptide protocol.
Sources & Research
- 1. Teichman SL, Neale A, Lawrence B, et al. Prolonged Stimulation of Growth Hormone (GH) and Insulin-Like Growth Factor I Secretion by CJC-1295, a Long-Acting Analog of GH-Releasing Hormone, in Healthy Adults. Journal of Clinical Endocrinology and Metabolism (2006)
- 2. Ionescu M, Frohman LA. Pulsatile Secretion of Growth Hormone (GH) Persists during Continuous Stimulation by CJC-1295, a Long-Acting GH-Releasing Hormone Analog. Journal of Clinical Endocrinology and Metabolism (2006)
- 3. Jette L, Leger R, Thibaudeau K, et al. Human Growth Hormone-Releasing Factor (hGRF)1-29-Albumin Bioconjugates Activate the GRF Receptor on the Anterior Pituitary in Rats: Identification of CJC-1295 as a Long-Lasting GRF Analog. Endocrinology (2005)
- 4. Alba M, Fintini D, Sagazio A, et al. Once-daily administration of CJC-1295, a long-acting GHRH analog, normalizes growth in the GHRH knockout mouse. American Journal of Physiology - Endocrinology and Metabolism (2006)
- 5. Sackmann-Sala L, Ding J, Frohman LA, Kopchick JJ. Activation of the GH/IGF-1 axis by CJC-1295, a long-acting GHRH analog, results in serum protein profile changes in normal adult subjects. Growth Hormone and IGF Research (2009)
- 6. Clemmons DR. Long-acting forms of growth hormone-releasing hormone and growth hormone: effects in normal volunteers and adults with growth hormone deficiency. Hormone Research (2007)
- 7. Henninge J, Pepaj M, Hullstein I, Hemmersbach P. Identification of CJC-1295, a growth-hormone-releasing peptide, in an unknown pharmaceutical preparation. Drug Testing and Analysis (2010)
- 8. ConjuChem Biotechnologies Phase 2 Trial of CJC-1295 in HIV-Associated Visceral Fat Accumulation (NCT00267527). ClinicalTrials.gov (2006)
- 9. Aidsmap (Carter M). Lipodystrophy study halted after patient death. Aidsmap News (2006)
- 10. U.S. Food and Drug Administration. Bulk Drug Substances Nominated for Use in Compounding Under Section 503A - CJC-1295 review record (FDA-2024-N-4777-0009, attachment 6). FDA.gov (2024)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page