CagriSema Quick Start
CagriSema is the once-weekly fixed-dose combination of cagrilintide 2.4 mg(a long-acting amylin analogue) and semaglutide 2.4 mg (a GLP-1 receptor agonist) developed by Novo Nordisk for chronic weight management.
On December 18, 2025, Novo Nordisk submitted a New Drug Application to the FDA, with review expected in 2026. CagriSema is not currently approved in the U.S. or EU. This page is an educational research reference and does not constitute medical advice.
Researchers planning a cagrilintide + semaglutide protocol generally choose one of two formats: a pre-blended vial that delivers both compounds in a single weekly injection, or two separate vials titrated independently. Both formats appear below.
Reconstitute
Pre-blended vial: add BAC water per vial spec; separate vials: reconstitute each independently.
Dosing
Final research-target weekly dose: cagrilintide 2.4 mg + semaglutide 2.4 mg.
Titration
Typically 16 weeks of dose escalation before maintenance, mirroring the REDEFINE protocol.
Cycle length
REDEFINE trials ran 68 weeks; research cycles are commonly 12–24 weeks.
Status
Investigational; FDA NDA filed December 2025; not approved.
Disclaimer
This page is an educational research reference and is not medical advice. CagriSema is not FDA-approved. The dosing schedules below mirror the protocols used in published Phase 3 clinical trials and are reported here for educational research context only. They are not dosing recommendations and are not a substitute for guidance from a qualified healthcare provider.
CagriSema Dosing Protocol & Schedule
The REDEFINE 1 and REDEFINE 2 Phase 3 trials titrated participants over roughly 16 weeks to a final research-target dose of cagrilintide 2.4 mg plus semaglutide 2.4 mg, administered once weekly by subcutaneous injection. The schedule below mirrors that protocol structure for educational research planning. It is not a dosing recommendation.
CagriSema Dosing Guide
Choose the vial format you are using to see the matching schedule.
A single fixed-dose vial delivers cagrilintide and semaglutide together in one weekly injection.
Blend ratio
2.4 / 2.4 mg
1:1 fixed-dose
At the maintenance dose, each weekly injection delivers cagrilintide 2.4 mg and semaglutide 2.4 mg. Earlier titration weeks deliver smaller, paired amounts; the per-injection volume depends on the specific vial concentration.
Final research-target dose
2.4 mg + 2.4 mg weekly
Titration length
~16 weeks
Trial duration
68 weeks (REDEFINE 1 / REDEFINE 2)
Route
Subcutaneous, once weekly
Compound Delivery: 2.4 mg / 2.4 mg Maintenance
| Cagrilintide | 2.4 mg |
|---|---|
| Semaglutide | 2.4 mg |
Pre-blended vials simplify weekly administration to a single injection but lock the ratio at 1:1. Researchers who want to titrate one compound independently of the other should use the separate-vials format.
Typical 16-Week Titration
Pre-blended CagriSema Titration (mirrors REDEFINE protocol structure)
Week
1–4
Cagrilintide
0.25 mg
Semaglutide
0.25 mg
Notes
Initiation: gastrointestinal tolerability is highest priority.
Week
5–8
Cagrilintide
0.5 mg
Semaglutide
0.5 mg
Notes
Early escalation; nausea typically peaks in this window.
Week
9–12
Cagrilintide
1.0 mg
Semaglutide
1.0 mg
Notes
Mid escalation.
Week
13–16
Cagrilintide
1.7 mg
Semaglutide
1.7 mg
Notes
Late escalation.
Week
17+
Cagrilintide
2.4 mg
Semaglutide
2.4 mg
Notes
Maintenance research-target dose.
| Week | Cagrilintide | Semaglutide | Notes |
|---|---|---|---|
| 1–4 | 0.25 mg | 0.25 mg | Initiation: gastrointestinal tolerability is highest priority. |
| 5–8 | 0.5 mg | 0.5 mg | Early escalation; nausea typically peaks in this window. |
| 9–12 | 1.0 mg | 1.0 mg | Mid escalation. |
| 13–16 | 1.7 mg | 1.7 mg | Late escalation. |
| 17+ | 2.4 mg | 2.4 mg | Maintenance research-target dose. |
Titration step values follow the REDEFINE Phase 3 protocol structure as reported by Novo Nordisk and the NEJM publications. This is not a dosing recommendation.
Two vials administered as two injections per session (or staggered) when independent titration matters.
Separate-vial workflow
Independent dose control for cagrilintide and semaglutide
Use separate vials when you want to escalate cagrilintide and semaglutide on different schedules, hold one compound at a lower dose, or accommodate different vial concentrations.
Injection burden
1–2 injections per session
Best for
Independent titration; flexible ratios
Cycle driver
Whichever compound titrates more slowly
Cagrilintide
- Loading
- 0.25 → 2.4 mg over ~16 weeks
- Frequency
- Once weekly
- Maintenance
- 2.4 mg
- Route
- SubQ
Semaglutide
- Loading
- 0.25 → 2.4 mg over ~16 weeks
- Frequency
- Once weekly
- Maintenance
- 2.4 mg
- Route
- SubQ
Weekly Schedule Example (Maintenance)
Same day each week
Cagrilintide 2.4 mg SubQ + Semaglutide 2.4 mg SubQ
Use separate syringes for each compound. Many researchers inject both on the same day at the same site rotation; staggering by a few hours is also common to isolate any tolerability signal to one compound.
Cycle Guidelines
CagriSema Cycle Length Reference
Approach
Trial-mirroring cycle
Duration
68 weeks
Off Period
Per clinician guidance
Best For
Matching REDEFINE 1 / REDEFINE 2 clinical trials.
Approach
Standard research cycle
Duration
12–24 weeks
Off Period
4–8 weeks
Best For
Most planning windows; aligns with phase 2 obesity trial readouts.
Approach
Short investigative cycle
Duration
8–12 weeks
Off Period
4 weeks
Best For
Tolerability and titration assessment only.
| Approach | Duration | Off Period | Best For |
|---|---|---|---|
| Trial-mirroring cycle | 68 weeks | Per clinician guidance | Matching REDEFINE 1 / REDEFINE 2 clinical trials. |
| Standard research cycle | 12–24 weeks | 4–8 weeks | Most planning windows; aligns with phase 2 obesity trial readouts. |
| Short investigative cycle | 8–12 weeks | 4 weeks | Tolerability and titration assessment only. |
REDEFINE trials measured outcomes at 68 weeks. Shorter cycles will see proportionally smaller weight-change endpoints.
CagriSema Supplies Needed
Plan supplies based on the once-weekly schedule above. The math below assumes the pre-blended format with one injection per week. If you run separate vials, double the syringe and swab counts and add a second BAC water draw per session.
Recommended USA Supply
Choose your region
Use discount code PEPPAL at Peptide Partners checkout. See why we love Peptide Partners.

Cagrilintide (10mg vials)

At-Home Blood Test
Research Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials
The math below assumes 20 mg pre-blended vials containing cagrilintide 10 mg plus semaglutide 10 mg. At 4.8 mg total per weekly maintenance dose, each vial covers 4 full maintenance draws with a small residual.
| Cycle length | Planning note |
|---|---|
8 weeks 2 vials | 8 full weekly maintenance doses; about 1.6 mg total residual. |
12 weeks 3 vials | 12 full weekly maintenance doses; about 2.4 mg total residual. |
16 weeks 4 vials | 16 full weekly maintenance doses; about 3.2 mg total residual. |
24 weeks 6 vials | 24 full weekly maintenance doses; about 4.8 mg total residual. |
68 weeks (trial-length) 17 vials | 68 full weekly maintenance doses; matches REDEFINE 1 / REDEFINE 2 duration. |
8 weeks
2 vials
8 full weekly maintenance doses; about 1.6 mg total residual.
12 weeks
3 vials
12 full weekly maintenance doses; about 2.4 mg total residual.
16 weeks
4 vials
16 full weekly maintenance doses; about 3.2 mg total residual.
24 weeks
6 vials
24 full weekly maintenance doses; about 4.8 mg total residual.
68 weeks (trial-length)
17 vials
68 full weekly maintenance doses; matches REDEFINE 1 / REDEFINE 2 duration.
Insulin Syringes (U-100)
One syringe per weekly injection (pre-blended). Double for separate-vials format.
| Cycle length | Planning note |
|---|---|
8 weeks 8 syringes | Pre-blended; 16 if separate vials. |
12 weeks 12 syringes | Pre-blended; 24 if separate vials. |
16 weeks 16 syringes | Pre-blended; 32 if separate vials. |
24 weeks 24 syringes | Pre-blended; 48 if separate vials. |
68 weeks (trial-length) 68 syringes | Pre-blended; 136 if separate vials. |
8 weeks
8 syringes
Pre-blended; 16 if separate vials.
12 weeks
12 syringes
Pre-blended; 24 if separate vials.
16 weeks
16 syringes
Pre-blended; 32 if separate vials.
24 weeks
24 syringes
Pre-blended; 48 if separate vials.
68 weeks (trial-length)
68 syringes
Pre-blended; 136 if separate vials.
Bacteriostatic Water
Volume per vial depends on vial size and target concentration. The math below assumes ~2–3 mL per vial.
| Cycle length | Planning note |
|---|---|
8-16 weeks 1 × 30 mL bottle | 8 weeks: Roughly 4–6 mL used; one bottle covers cycle plus margin.; 12 weeks: Roughly 6–9 mL used.; 16 weeks: Roughly 8–12 mL used. |
24 weeks, 68 weeks (trial-length) 2 × 30 mL bottles | 24 weeks: Roughly 12–18 mL used; second bottle for margin.; 68 weeks (trial-length): Roughly 34–51 mL used over the cycle. |
8-16 weeks
1 × 30 mL bottle
8 weeks: Roughly 4–6 mL used; one bottle covers cycle plus margin.; 12 weeks: Roughly 6–9 mL used.; 16 weeks: Roughly 8–12 mL used.
24 weeks, 68 weeks (trial-length)
2 × 30 mL bottles
24 weeks: Roughly 12–18 mL used; second bottle for margin.; 68 weeks (trial-length): Roughly 34–51 mL used over the cycle.
Round up for priming losses, dropped syringes, damaged swabs, and any titration or schedule adjustments.
Companion Supplies & Routine Support
CagriSema Reconstitution Guide
Reconstitution math depends on vial size and the dose you intend to draw each week. The two tabs below mirror the dosing tabs above. For exact syringe-unit calculations at any vial size, use the free Peptide Reconstitution Calculator.
Reconstitution by Vial Format
A single vial holding both compounds in fixed ratio.
The featured pre-blended CagriSema vial contains 20 mg total: cagrilintide 10 mg plus semaglutide 10 mg. At the 2.4 mg + 2.4 mg maintenance dose, that is 4.8 mg total per week, so one vial covers 4 full weekly maintenance draws with about 0.8 mg total residual. BAC water volume is dictated by the vial concentration printed on the COA — there is no universal default for a fixed-dose combination, so verify the supplier's spec before reconstituting.
Pre-blended Reconstitution Reference (verify against supplier COA)
Total mg per vial
20 mg (4 full doses)
BAC water added
2.0 mL
Concentration (combined)
10 mg/mL
Approx weekly draw at 4.8 mg total
0.48 mL = 48 units U-100
Total mg per vial
20 mg (4 full doses)
BAC water added
3.0 mL
Concentration (combined)
6.67 mg/mL
Approx weekly draw at 4.8 mg total
0.72 mL = 72 units U-100
Total mg per vial
20 mg (4 full doses)
BAC water added
2.5 mL
Concentration (combined)
8 mg/mL
Approx weekly draw at 4.8 mg total
0.60 mL = 60 units U-100
| Total mg per vial | BAC water added | Concentration (combined) | Approx weekly draw at 4.8 mg total |
|---|---|---|---|
| 20 mg (4 full doses) | 2.0 mL | 10 mg/mL | 0.48 mL = 48 units U-100 |
| 20 mg (4 full doses) | 3.0 mL | 6.67 mg/mL | 0.72 mL = 72 units U-100 |
| 20 mg (4 full doses) | 2.5 mL | 8 mg/mL | 0.60 mL = 60 units U-100 |
These rows are illustrative only. Always verify total mg and concentration on the supplier's COA before drawing a dose.
Reconstitute each compound independently.
Common research vial sizes for cagrilintide and semaglutide are 5 mg and 10 mg. The table below assumes 2.4 mg weekly maintenance for each compound.
Separate-vials Reconstitution Reference
Compound
Cagrilintide
Vial size
5 mg
BAC water
2.0 mL
Concentration
2.5 mg/mL
Weekly draw at 2.4 mg
0.96 mL = 96 units U-100
Compound
Cagrilintide
Vial size
10 mg
BAC water
3.0 mL
Concentration
3.33 mg/mL
Weekly draw at 2.4 mg
0.72 mL = 72 units U-100
Compound
Semaglutide
Vial size
5 mg
BAC water
2.0 mL
Concentration
2.5 mg/mL
Weekly draw at 2.4 mg
0.96 mL = 96 units U-100
Compound
Semaglutide
Vial size
10 mg
BAC water
3.0 mL
Concentration
3.33 mg/mL
Weekly draw at 2.4 mg
0.72 mL = 72 units U-100
| Compound | Vial size | BAC water | Concentration | Weekly draw at 2.4 mg |
|---|---|---|---|---|
| Cagrilintide | 5 mg | 2.0 mL | 2.5 mg/mL | 0.96 mL = 96 units U-100 |
| Cagrilintide | 10 mg | 3.0 mL | 3.33 mg/mL | 0.72 mL = 72 units U-100 |
| Semaglutide | 5 mg | 2.0 mL | 2.5 mg/mL | 0.96 mL = 96 units U-100 |
| Semaglutide | 10 mg | 3.0 mL | 3.33 mg/mL | 0.72 mL = 72 units U-100 |
Volumes near 1 mL exceed standard U-100 / 0.3 mL syringe capacity. For higher draws, use a 1 mL U-100 syringe.
Reconstitution Steps
1. Wash your hands and lay out a clean work surface.
2. Wipe the rubber stopper of each vial with an alcohol swab and let it dry.
3. Draw the planned BAC water volume into a fresh syringe.
4. Inject the BAC water down the inside wall of the peptide vial — do not spray directly onto the lyophilized powder.
5. Swirl gently until the powder is fully dissolved. Do not shake.
6. Label the vial with the date of reconstitution and the concentration.
7. Refrigerate at 36–46°F (2–8°C) and use within the supplier-specified stability window.
Use the calculator for exact units
For any custom vial size, BAC water volume, or weekly dose, the free Peptide Reconstitution Calculator returns exact U-100 syringe units in seconds.
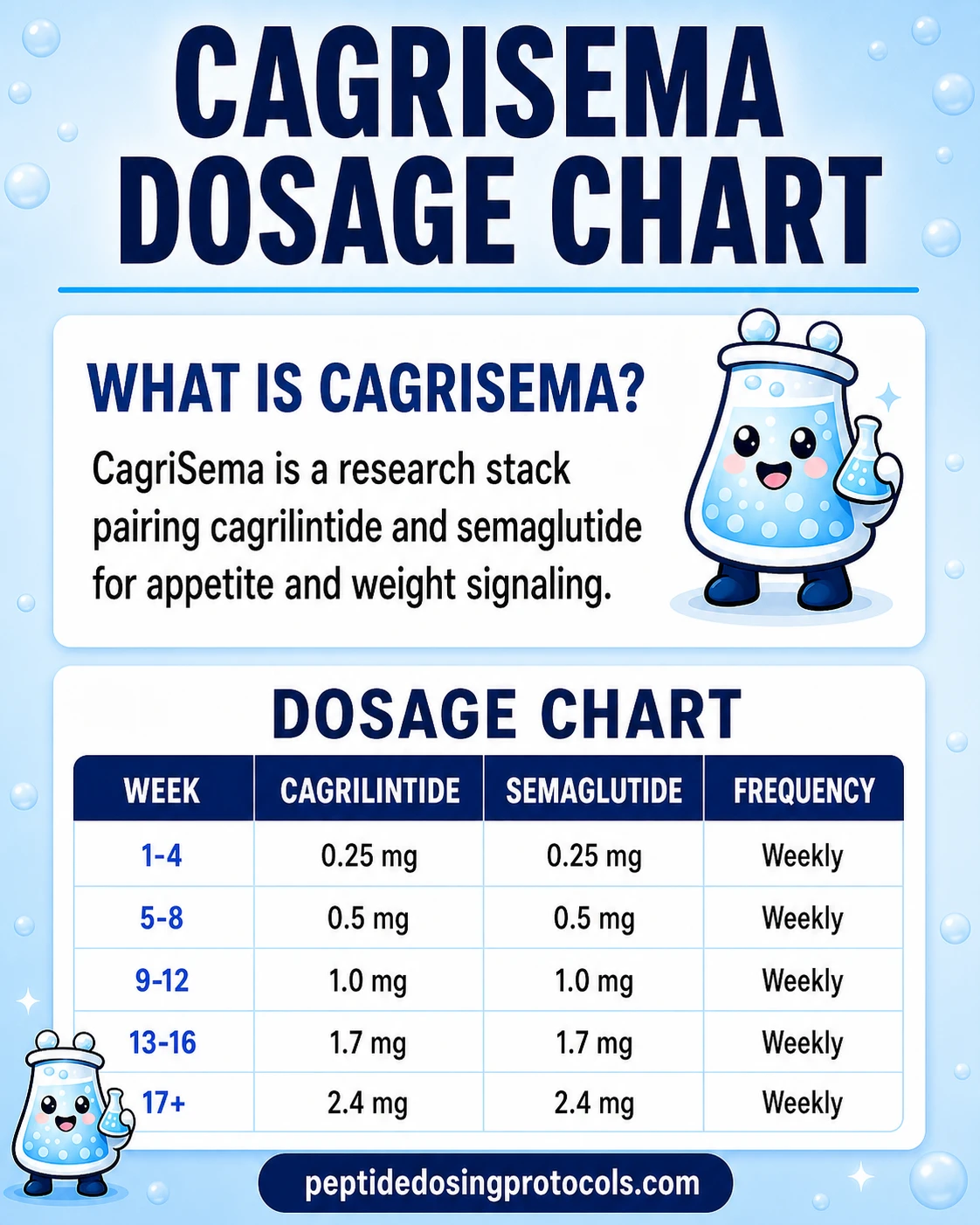
CagriSema Dosage Chart
This CagriSema dosage chart summarizes the common 16-week titration ladder for paired cagrilintide and semaglutide dosing, from 0.25 mg weekly to the 2.4 mg weekly research-target dose for each compound.
Why CagriSema Combines Cagrilintide and Semaglutide
Appetite is regulated by overlapping signals from the gut, pancreas, and brain. Cagrilintide and semaglutide target two of those signals through different receptors, which is the rationale for combining them.
Cagrilintide — amylin pathway
Cagrilintide is a long-acting amylin analogue described in the literature as a dual amylin and calcitonin receptor agonist (DACRA). Amylin is normally co-secreted with insulin after meals; it strengthens meal-stop satiety, slows gastric emptying, and suppresses post-meal glucagon. The Phase 1b development paper reported a half-life of roughly 159–195 hours, which supports once-weekly dosing.
Semaglutide — GLP-1 pathway
Semaglutide is a GLP-1 receptor agonist already FDA-approved for chronic weight management as Wegovy (2.4 mg) and for type 2 diabetes as Ozempic. GLP-1 agonists reduce appetite, slow gastric emptying, and improve glycemic control through glucose-dependent insulin secretion.
Why pair them
The pathways overlap on satiety and gastric emptying but engage different receptor families. In REDEFINE 1, the combination produced larger average weight loss than either compound alone — 20.4% with CagriSema versus 14.9% with semaglutide alone and 11.5% with cagrilintide alone, all under the treatment-policy estimand. That's the practical evidence that the two pathways are additive rather than redundant in humans.
CagriSema Side Effects & Safety
CagriSema's tolerability profile is dominated by gastrointestinal events, consistent with the GLP-1 receptor agonist class and amylin pathway literature. Most events were reported as mild-to-moderate and concentrated during dose escalation.
REDEFINE 1 — adults with overweight/obesity, no diabetes
GI adverse events were reported in 79.6% of CagriSema participants vs 39.9% on placebo. Specific event rates included nausea (55% vs 12.6%), constipation (30.7% vs 11.6%), and vomiting (26.1% vs 4.1%). Discontinuation due to adverse events was 5.9% on CagriSema vs 3.5% on placebo.
REDEFINE 2 — adults with type 2 diabetes
GI events were reported in 72.5% of CagriSema participants vs 34.4% on placebo. Discontinuation due to adverse events was 8.4% on CagriSema vs 3% on placebo.
Pattern across both trials
Nausea, vomiting, and diarrhea peaked during dose escalation and tapered during maintenance; constipation remained more stable across the trial period. The sponsor described the safety profile as comparable with the broader GLP-1 receptor agonist class. PepPal's guide to companion supplements for GLP-1 users covers protein, fiber, electrolytes, and lab-driven nutrient support.
Stack-specific unknowns and quality risk
No published trial has compared CagriSema head-to-head against a research-use compounded equivalent. Because CagriSema is investigational, any non-FDA-approved or compounded product must be evaluated for identity, purity, and contamination risk before use. The FDA in early 2026 highlighted enforcement actions targeting non-approved GLP-1 active ingredients in compounded drugs, which underscores the quality-control concern.
CagriSema Clinical Trials Evidence
CagriSema's evidence base is unusually strong for a peptide research stack: two large Phase 3 trials with NEJM publications, plus Phase 1b/2 supporting data. The numbers below are from the published REDEFINE 1 and REDEFINE 2 papers and the Novo Nordisk FDA filing announcement.
REDEFINE Trial Headlines
Trial
REDEFINE 1
Phase
3
Duration
68 weeks
Population (N)
3,417 adults with obesity or overweight + ≥1 comorbidity, without T2D
Key Result
−20.4% mean weight change vs −3.0% placebo (treatment-policy); −22.7% vs −2.3% (trial-product). 91.9% achieved ≥5% weight loss vs 31.5% placebo.
Trial
REDEFINE 2
Phase
3
Duration
68 weeks
Population (N)
1,206 adults with T2D + obesity/overweight
Key Result
−13.7% mean weight change vs −3.4% placebo (treatment-policy). 73.5% reached HbA1c ≤6.5% vs 15.9% placebo.
Trial
REDEFINE 11 (ongoing)
Phase
3
Duration
Longer duration
Population (N)
Adults with BMI ≥30
Key Result
Long-term efficacy and maintenance — readout pending.
Trial
REDEFINE 3 (ongoing)
Phase
3
Duration
Event-driven
Population (N)
Adults with cardiovascular disease
Key Result
Cardiovascular outcomes — readout pending.
Trial
REIMAGINE 2
Phase
3
Duration
Reported 2026
Population (N)
Adults with T2D
Key Result
Sponsor reported HbA1c reduction of 1.91 percentage points and 14.2% weight loss.
Trial
Phase 1b (Lau et al., 2021)
Phase
1b
Duration
20 weeks
Population (N)
Multiple-ascending-dose study
Key Result
Cagrilintide half-life ~159–195 hours; supports once-weekly dosing.
| Trial | Phase | Duration | Population (N) | Key Result |
|---|---|---|---|---|
| REDEFINE 1 | 3 | 68 weeks | 3,417 adults with obesity or overweight + ≥1 comorbidity, without T2D | −20.4% mean weight change vs −3.0% placebo (treatment-policy); −22.7% vs −2.3% (trial-product). 91.9% achieved ≥5% weight loss vs 31.5% placebo. |
| REDEFINE 2 | 3 | 68 weeks | 1,206 adults with T2D + obesity/overweight | −13.7% mean weight change vs −3.4% placebo (treatment-policy). 73.5% reached HbA1c ≤6.5% vs 15.9% placebo. |
| REDEFINE 11 (ongoing) | 3 | Longer duration | Adults with BMI ≥30 | Long-term efficacy and maintenance — readout pending. |
| REDEFINE 3 (ongoing) | 3 | Event-driven | Adults with cardiovascular disease | Cardiovascular outcomes — readout pending. |
| REIMAGINE 2 | 3 | Reported 2026 | Adults with T2D | Sponsor reported HbA1c reduction of 1.91 percentage points and 14.2% weight loss. |
| Phase 1b (Lau et al., 2021) | 1b | 20 weeks | Multiple-ascending-dose study | Cagrilintide half-life ~159–195 hours; supports once-weekly dosing. |
REDEFINE 1 and REDEFINE 2 are the basis for the December 2025 FDA NDA. The Reuters report on a head-to-head trial against tirzepatide (February 2026) noted CagriSema did not meet a non-inferiority threshold against tirzepatide on average weight loss at 84 weeks.
The most useful nuance for readers comparing headlines: REDEFINE 1's 20.4% number is the treatment-policy estimand (closer to intention-to-treat — what happens regardless of whether participants stayed on treatment). The 22.7% number is the trial-product estimand (what happens if participants stay on treatment as intended). Most consumer coverage quotes one without naming which, which makes cross-trial comparisons against tirzepatide's headlines noisier than they need to be.
CagriSema Storage & Handling
Storage Reference
Lyophilized (powder form)
Cagrilintide
-4°F (-20°C) long-term
Semaglutide
-4°F (-20°C) long-term
Pre-blended CagriSema
-4°F (-20°C) long-term
Reconstituted (liquid form)
Cagrilintide
35.6–46.4°F (2–8°C)
Semaglutide
35.6–46.4°F (2–8°C)
Pre-blended CagriSema
35.6–46.4°F (2–8°C)
Appearance
Cagrilintide
Clear after reconstitution
Semaglutide
Clear after reconstitution
Pre-blended CagriSema
Clear after reconstitution
Stability window after reconstitution
Cagrilintide
Up to ~28 days refrigerated
Semaglutide
Up to ~28 days refrigerated
Pre-blended CagriSema
Per supplier COA
| Cagrilintide | Semaglutide | Pre-blended CagriSema | |
|---|---|---|---|
| Lyophilized (powder form) | -4°F (-20°C) long-term | -4°F (-20°C) long-term | -4°F (-20°C) long-term |
| Reconstituted (liquid form) | 35.6–46.4°F (2–8°C) | 35.6–46.4°F (2–8°C) | 35.6–46.4°F (2–8°C) |
| Appearance | Clear after reconstitution | Clear after reconstitution | Clear after reconstitution |
| Stability window after reconstitution | Up to ~28 days refrigerated | Up to ~28 days refrigerated | Per supplier COA |
Always defer to the supplier's specific stability window. Discard if the solution becomes cloudy or shows particulate.
Avoid freezing reconstituted solution. Avoid direct sunlight and ambient temperatures above 77°F (25°C) for extended periods.
CagriSema vs Tirzepatide vs Semaglutide Alone
The three most relevant comparators for CagriSema are tirzepatide (Zepbound/Mounjaro), semaglutide alone (Wegovy/Ozempic), and cagrilintide alone. The table below summarizes the pharmacology and headline efficacy.
CagriSema vs Comparators
Feature
Receptor targets
CagriSema
Amylin/calcitonin + GLP-1
Tirzepatide (Zepbound)
GIP + GLP-1
Semaglutide alone (Wegovy)
GLP-1
Cagrilintide alone
Amylin/calcitonin (DACRA)
Feature
Dosing frequency
CagriSema
Once weekly
Tirzepatide (Zepbound)
Once weekly
Semaglutide alone (Wegovy)
Once weekly
Cagrilintide alone
Once weekly
Feature
Maintenance dose
CagriSema
2.4 mg + 2.4 mg
Tirzepatide (Zepbound)
Up to 15 mg
Semaglutide alone (Wegovy)
2.4 mg
Cagrilintide alone
2.4 mg (in REDEFINE arms)
Feature
Headline weight loss
CagriSema
−20.4% at 68 wks (REDEFINE 1, treatment-policy)
Tirzepatide (Zepbound)
Up to −22.5% at 72 wks (SURMOUNT-1, 15 mg arm)
Semaglutide alone (Wegovy)
−14.9% at 68 wks (REDEFINE 1 reference arm)
Cagrilintide alone
−11.5% at 68 wks (REDEFINE 1 reference arm)
Feature
FDA status (June 2026)
CagriSema
NDA filed Dec 2025; not approved
Tirzepatide (Zepbound)
Approved (Zepbound, Mounjaro)
Semaglutide alone (Wegovy)
Approved (Wegovy, Ozempic)
Cagrilintide alone
Investigational
Feature
Head-to-head data
CagriSema
Did not meet non-inferiority vs tirzepatide at 84 wks (Reuters Feb 2026)
Tirzepatide (Zepbound)
—
Semaglutide alone (Wegovy)
—
Cagrilintide alone
—
| Feature | CagriSema | Tirzepatide (Zepbound) | Semaglutide alone (Wegovy) | Cagrilintide alone |
|---|---|---|---|---|
| Receptor targets | Amylin/calcitonin + GLP-1 | GIP + GLP-1 | GLP-1 | Amylin/calcitonin (DACRA) |
| Dosing frequency | Once weekly | Once weekly | Once weekly | Once weekly |
| Maintenance dose | 2.4 mg + 2.4 mg | Up to 15 mg | 2.4 mg | 2.4 mg (in REDEFINE arms) |
| Headline weight loss | −20.4% at 68 wks (REDEFINE 1, treatment-policy) | Up to −22.5% at 72 wks (SURMOUNT-1, 15 mg arm) | −14.9% at 68 wks (REDEFINE 1 reference arm) | −11.5% at 68 wks (REDEFINE 1 reference arm) |
| FDA status (June 2026) | NDA filed Dec 2025; not approved | Approved (Zepbound, Mounjaro) | Approved (Wegovy, Ozempic) | Investigational |
| Head-to-head data | Did not meet non-inferiority vs tirzepatide at 84 wks (Reuters Feb 2026) | — | — | — |
These compounds are not interchangeable. Headline numbers come from different populations, durations, and estimand definitions — the table is for orientation, not direct conclusion.
Practical reading: tirzepatide currently shows the highest average weight loss in head-to-head reporting and is FDA-approved. CagriSema's REDEFINE 1 number is competitive against tirzepatide's SURMOUNT-1 figure, but a direct head-to-head trial reported in February 2026 favored tirzepatide. Semaglutide alone remains the most widely available approved GLP-1 option. Related PDP protocol pages: Tirzepatide, Semaglutide, Cagrilintide, Retatrutide.
CagriSema Blood Tests & Monitoring
CagriSema combines cagrilintide and semaglutide, so monitoring should cover amylin and GLP-1 metabolic pathways. The practical focus is glucose, kidney function, lipids, GI tolerance, gallbladder/pancreas symptoms, and thyroid-history cautions.
Blood test markers to discuss with a clinician
Marker
A1c
Why it matters
Shows longer-term glucose control and helps track metabolic response over time.
Timing
Baseline
Marker
Fasting glucose
Why it matters
Gives a current glucose snapshot, especially when appetite and diabetes medication needs change.
Timing
Follow-up
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews kidney function, liver enzymes, electrolytes, and glucose, which matter with GI symptoms or dehydration.
Timing
Baseline
Marker
Lipid panel
Why it matters
Tracks cardiometabolic changes during weight-loss or diabetes-management phases.
Timing
Follow-up
Marker
Blood pressure and resting heart rate
Why it matters
Adds cardiovascular context during weight loss, medication changes, and hydration shifts.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| A1c | Shows longer-term glucose control and helps track metabolic response over time. | Baseline |
| Fasting glucose | Gives a current glucose snapshot, especially when appetite and diabetes medication needs change. | Follow-up |
| Comprehensive metabolic panel (CMP) | Reviews kidney function, liver enzymes, electrolytes, and glucose, which matter with GI symptoms or dehydration. | Baseline |
| Lipid panel | Tracks cardiometabolic changes during weight-loss or diabetes-management phases. | Follow-up |
| Blood pressure and resting heart rate | Adds cardiovascular context during weight loss, medication changes, and hydration shifts. | Optional |
Monitoring guidance is label-informed for semaglutide and trial-informed/pathway-based for cagrilintide.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting or escalating, especially with diabetes, kidney disease, pancreatitis history, gallbladder history, thyroid cancer history, or major calorie restriction.
Follow-up
Repeat glucose and CMP-related markers after 4-12 weeks or sooner if vomiting, dehydration, or glucose symptoms occur.
Longer term
For ongoing protocols, review metabolic and kidney trends every 3-6 months with a clinician.
How to interpret the labs
- CagriSema has stronger appetite and GI-tolerance relevance than a broad metabolic panel alone can show.
- Diabetes medication review may be needed when food intake and glucose trends change.
- Personal or family history of medullary thyroid carcinoma or MEN2 is an important label-based caution for the semaglutide component.
Do not wait for routine labs
Severe abdominal pain, persistent vomiting, signs of dehydration, fainting, allergic symptoms, or severe low-glucose symptoms need medical review. A neck mass, trouble swallowing, or persistent hoarseness should be discussed with a clinician.
FAQ
Q1: Is CagriSema FDA-approved?
No. As of June 2026, CagriSema is not FDA-approved. Novo Nordisk submitted a New Drug Application to the FDA on December 18, 2025, with FDA review expected during 2026. Until any approval is granted, CagriSema remains investigational and is not available as a prescription medication. This page is an educational research reference and not medical advice.
Q2: What is the CagriSema dose used in clinical trials?
The REDEFINE 1 and REDEFINE 2 Phase 3 trials used a once-weekly subcutaneous dose of cagrilintide 2.4 mg combined with semaglutide 2.4 mg, reached after roughly 16 weeks of dose titration. The titration started at 0.25 mg of each compound and stepped up every 4 weeks. This is reported here for educational research context and is not a dosing recommendation.
Q3: How much weight loss did CagriSema produce in REDEFINE 1?
In REDEFINE 1, adults with obesity or overweight (without diabetes) treated with CagriSema had a mean body weight reduction of 20.4% at 68 weeks under the treatment-policy estimand, compared with 3.0% on placebo. Under the trial-product estimand (assuming participants stayed on treatment), the reduction was 22.7%. Always check which estimand a headline number is using before comparing across trials.
Q4: What is the difference between the treatment-policy and trial-product estimands?
Both are statistical frameworks for analyzing trial outcomes. The treatment-policy estimand is closer to intention-to-treat: it estimates the effect regardless of whether participants stayed on treatment or used rescue therapies. The trial-product estimand is closer to as-treated: it estimates the effect if participants stayed on treatment as intended. CagriSema's REDEFINE 1 result reads as 20.4% under treatment-policy or 22.7% under trial-product. The numbers are not contradictory — they answer different questions.
Q5: How does CagriSema compare to tirzepatide?
Both produce large average weight loss in obesity. In a head-to-head open-label trial reported in February 2026, average weight loss at 84 weeks favored tirzepatide, and the sponsor noted CagriSema did not meet its prespecified non-inferiority target against tirzepatide. As of June 2026, tirzepatide is FDA-approved (Zepbound, Mounjaro) and CagriSema is not. See the Tirzepatide protocol for receptor and dosing details.
Q6: Is CagriSema a peptide?
Yes. CagriSema is a fixed-dose combination of two peptide-based drugs. Cagrilintide is a long-acting amylin analogue. Semaglutide is a GLP-1 receptor agonist. Both are peptide therapeutics rather than small molecules. Same for related GLP-1 brand names — semaglutide is the active in Ozempic, Wegovy, and Rybelsus.
Q7: What are the most common CagriSema side effects?
Gastrointestinal events were the most common in both REDEFINE 1 and REDEFINE 2. In REDEFINE 1, GI events were reported in 79.6% of CagriSema participants versus 39.9% on placebo, including nausea (55%), constipation (30.7%), and vomiting (26.1%). Symptoms typically peaked during dose escalation and tapered during maintenance. Discontinuation due to adverse events was 5.9% in REDEFINE 1 and 8.4% in REDEFINE 2.
Q8: How long is a typical CagriSema research cycle?
REDEFINE 1 and REDEFINE 2 ran 68 weeks, with the first ~16 weeks dedicated to dose titration. Many research planning windows are shorter — 12 to 24 weeks is common for tolerability and titration assessment, with longer cycles for efficacy endpoints. Shorter cycles will see proportionally smaller weight-change endpoints than the full trial-length numbers.
Q9: Pre-blended vs separate vials — which format makes sense?
Pre-blended fixed-dose vials reduce weekly administration to a single injection but lock the cagrilintide:semaglutide ratio at 1:1. Separate vials require two injections (or staggered injections) and add reconstitution overhead, but they let you titrate or hold one compound independently. Most researchers mirroring the REDEFINE protocol use the pre-blended format.
Q10: Where can CagriSema be sourced for research?
CagriSema as a fixed-dose combination is investigational and not commercially available. Cagrilintide and semaglutide are individually available through research-use suppliers. Quality varies — verify identity, purity, and Certificate of Analysis documentation before use. The FDA in early 2026 publicly highlighted enforcement actions targeting non-approved GLP-1 active ingredients in compounded products, so source verification is non-negotiable.
Q11: Does CagriSema improve blood sugar in addition to weight?
Yes, in adults with type 2 diabetes. In REDEFINE 2, 73.5% of CagriSema participants reached HbA1c ≤6.5% versus 15.9% on placebo (treatment-policy estimand). Sponsor-reported REIMAGINE 2 data described an HbA1c reduction of 1.91 percentage points alongside 14.2% weight loss. This dual benefit is part of the rationale for filing CagriSema in both obesity and T2D contexts.
Q12: Is the dosing on this page medical advice?
No. Every dose, schedule, and supply quantity on this page is reported for educational research context and mirrors the published REDEFINE Phase 3 trial protocol. Nothing here is medical advice or a dosing recommendation. CagriSema is not FDA-approved as of the date above. Consult a qualified healthcare provider for any personal medical decision.
Sources & Research
- 1. Garvey WT, Blüher M, Osorto Contreras CK, et al. Coadministered Cagrilintide and Semaglutide in Adults with Overweight or Obesity (REDEFINE 1). New England Journal of Medicine (2025)
- 2. Davies MJ, Bajaj HS, Broholm C, et al. Cagrilintide–Semaglutide in Adults with Overweight or Obesity and Type 2 Diabetes (REDEFINE 2). New England Journal of Medicine (2025)
- 3. Novo Nordisk Inc. Novo Nordisk files for FDA approval of CagriSema, the first once-weekly combination of GLP-1 and amylin analogues for weight management. PR Newswire / Novo Nordisk corporate release (2025)
- 4. Enebo LB, Berthelsen KK, Kankam M, et al. Safety, tolerability, pharmacokinetics, and pharmacodynamics of concomitant administration of multiple doses of cagrilintide with semaglutide 2·4 mg for weight management: a randomised, controlled, phase 1b trial. The Lancet (2021)
- 5. Frias JP, Deenadayalan S, Erichsen L, et al. Efficacy and safety of co-administered once-weekly cagrilintide 2·4 mg with once-weekly semaglutide 2·4 mg in type 2 diabetes: a multicentre, randomised, double-blind, active-controlled, phase 2 trial. The Lancet (2023)
- 6. Lau DCW, Erichsen L, Francisco AM, et al. Once-weekly cagrilintide for weight management in people with overweight and obesity: a multicentre, randomised, double-blind, placebo-controlled and active-controlled, dose-finding phase 2 trial. The Lancet (2021)
- 7. ClinicalTrials.gov REDEFINE 3: A Research Study to See the Effects of CagriSema in People Living With Diseases in the Heart and Blood Vessels. ClinicalTrials.gov registry entry NCT05669755 (2025)
- 8. Novo Nordisk A/S. CagriSema demonstrated superior HbA1c reduction of 1.91 points and weight loss of 14.2% in adults with type 2 diabetes in the REIMAGINE 2 trial. BioSpace / Novo Nordisk corporate release (2026)
- 9. Reuters Novo Nordisk's CagriSema trial deals blow in obesity drug battle with Eli Lilly. Reuters (2026)
- 10. U.S. Food and Drug Administration FDA Intends to Take Action Against Non-FDA-Approved GLP-1 Drugs. FDA press announcement (2025)
- 11. U.S. Food and Drug Administration FDA Approves New Medication for Chronic Weight Management (tirzepatide / Zepbound). FDA press announcement (2023)
- 12. Hay DL, Chen S, Lutz TA, Parkes DG, Roth JD. Amylin: Pharmacology, Physiology, and Clinical Potential. Pharmacological Reviews (2015)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: July 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page