CJC-1295 + Ipamorelin Quick Start
The CJC-1295 + Ipamorelin stack is the most widely planned growth hormone (GH) peptide combination in the research community. CJC-1295 mimics the body's GHRH signal, telling the pituitary gland to make GH. Ipamorelin works through a separate ghrelin receptor pathway, telling the pituitary to release GH. Two different signals on the same target cell.
This guide focuses on CJC-1295 without DAC because its 30-minute to 2-hour half-life matches Ipamorelin's roughly 2-hour half-life, which preserves the body's natural pulsatile GH release. CJC-1295 with DAC has a 6-8 day half-life and a different planning model that fits poorly with Ipamorelin's short pulse.
Reconstitute
20 mg blend vial: add 3.0 mL BAC water → 6.67 mg/mL total (3.33 mg/mL each peptide).
Schedule
Most common research planning is once daily SubQ, on an empty stomach, before bed.
Easy measuring
On a U-100 syringe, 6 units = 0.06 mL = 200 mcg of each peptide from a 20 mg blend at 3.0 mL.
Supplies
1 vial covers about 50 daily draws at 200 mcg of each peptide or about 33 daily draws at 300 mcg of each.
Research status
Not FDA-approved. Each compound has separate human data; the combined blend has no published human RCT.
Disclaimer
This page is an educational research reference and is not medical advice. Both compounds are research-use-only and not FDA-approved. Anyone with active or prior cancer, pituitary disease, diabetic retinopathy, severe kidney disease, or pregnancy/breastfeeding should not use GH-stimulating peptides.
This page is for stack timing, dose setup, and practical planning. For the larger research view, see the CJC-1295 + Ipamorelin stack guide on each peptide's role, research, and safety notes.
CJC-1295 + Ipamorelin Dosing Protocol & Schedule
Choose the format you are working with. The featured math assumes a pre-blended 20 mg vial containing 10 mg CJC-1295 + 10 mg Ipamorelin. Separate 10 mg vials are used when researchers want independent dose control or a different ratio.
CJC-1295 + Ipamorelin Dosing Guide
Choose the vial format you are using to see the matching instructions.
20 mg blend (10 mg CJC-1295 + 10 mg Ipamorelin) at a 1:1 ratio.
Blend ratio
10 / 10 mg
1:1 (CJC-1295 no DAC : Ipamorelin)
20 mg total per vial: 10 mg CJC-1295 (no DAC) + 10 mg Ipamorelin. Reconstituted with 3.0 mL BAC water, the maximum fill used for this vial math.
Reconstitute
3.0 mL BAC water
Concentration
6.67 mg/mL total (3.33 mg/mL each)
Daily draw (200 mcg each)
6 units = 0.06 mL
Typical cycle
8-12 weeks
Dose selector
Component Delivery
| CJC-1295 (no DAC) | 100 mcg |
|---|---|
| Ipamorelin | 100 mcg |
Common research-planning targets land at 200-300 mcg of each compound daily. Lower doses (100-150 mcg) are typical for the first 2-4 weeks before titration.
Titration Plan (Once Daily)
Gradual titration on a 20 mg blend reconstituted with 3.0 mL BAC water
Week
Weeks 1-2
Dose (each peptide)
100 mcg
Insulin units
3 units
Volume
0.03 mL
Week
Weeks 3-4
Dose (each peptide)
150 mcg
Insulin units
4.5 units
Volume
0.045 mL
Week
Weeks 5-8
Dose (each peptide)
200 mcg
Insulin units
6 units
Volume
0.06 mL
Week
Weeks 9-12
Dose (each peptide)
200-300 mcg
Insulin units
6-9 units
Volume
0.06-0.09 mL
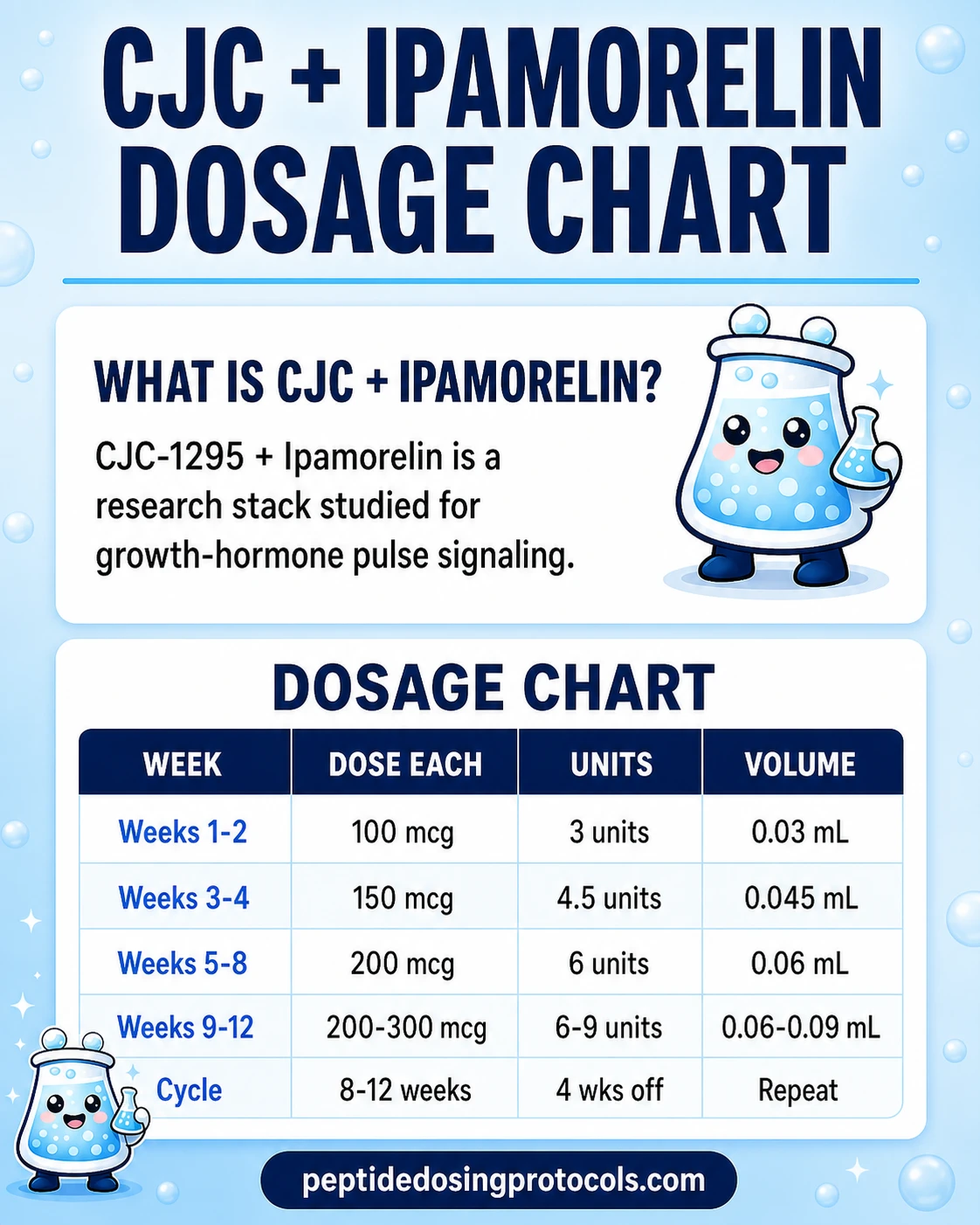
| Week | Dose (each peptide) | Insulin units | Volume |
|---|---|---|---|
| Weeks 1-2 | 100 mcg | 3 units | 0.03 mL |
| Weeks 3-4 | 150 mcg | 4.5 units | 0.045 mL |
| Weeks 5-8 | 200 mcg | 6 units | 0.06 mL |
| Weeks 9-12 | 200-300 mcg | 6-9 units | 0.06-0.09 mL |
These are research-planning ranges drawn from common protocol summaries (Teichman 2006 dosing studied CJC-1295 with DAC, not no-DAC). They are not personal dosing recommendations.
10 mg CJC-1295 (no DAC) and 10 mg Ipamorelin in independent vials.
Separate-vial workflow
Independent dose control
Use separate vials when researchers want to titrate each peptide independently, study a non-1:1 ratio, or stop one compound early.
Injection burden
Can mix into one syringe or use two
Best for
Asymmetric dosing or staggered cycling
Cycle driver
Compound-specific titration
CJC-1295 (no DAC)
- Loading
- 100 mcg
- Frequency
- Once daily
- Maintenance
- 200-300 mcg
- Route
- SubQ
Ipamorelin
- Loading
- 100 mcg
- Frequency
- Once daily
- Maintenance
- 200-300 mcg
- Route
- SubQ
Weekly Schedule Example
Monday
CJC-1295 200 mcg + Ipamorelin 200 mcg
Tuesday
CJC-1295 200 mcg + Ipamorelin 200 mcg
Wednesday
CJC-1295 200 mcg + Ipamorelin 200 mcg
Thursday
CJC-1295 200 mcg + Ipamorelin 200 mcg
Friday
CJC-1295 200 mcg + Ipamorelin 200 mcg
Saturday
CJC-1295 200 mcg + Ipamorelin 200 mcg
Sunday
CJC-1295 200 mcg + Ipamorelin 200 mcg
When mixing both peptides into a single syringe, draw each peptide separately and combine in the syringe. Use a fresh syringe per session.
Separate-Vial Reconstitution
Reconstitution math for 10 mg standalone vials
Vial
CJC-1295 10 mg
BAC water
3.0 mL
Concentration
3.33 mg/mL
200 mcg dose
6 units (0.06 mL)
Vial
Ipamorelin 10 mg
BAC water
3.0 mL
Concentration
3.33 mg/mL
200 mcg dose
6 units (0.06 mL)
| Vial | BAC water | Concentration | 200 mcg dose |
|---|---|---|---|
| CJC-1295 10 mg | 3.0 mL | 3.33 mg/mL | 6 units (0.06 mL) |
| Ipamorelin 10 mg | 3.0 mL | 3.33 mg/mL | 6 units (0.06 mL) |
This separate-vial reference uses 3.0 mL as the maximum fill for the same vial-capacity constraint.
Cycle Guidelines
Common research-planning cycle structures
Approach
Standard
On Cycle
8-12 weeks
Off Period
4 weeks
Notes
Most common research-planning structure.
Approach
Extended
On Cycle
16 weeks
Off Period
8 weeks
Notes
Used for longer-arc plans; off-period helps reset receptor sensitivity.
Approach
Short test
On Cycle
4-6 weeks
Off Period
4 weeks
Notes
Used for short tolerability windows or budget-limited plans.
| Approach | On Cycle | Off Period | Notes |
|---|---|---|---|
| Standard | 8-12 weeks | 4 weeks | Most common research-planning structure. |
| Extended | 16 weeks | 8 weeks | Used for longer-arc plans; off-period helps reset receptor sensitivity. |
| Short test | 4-6 weeks | 4 weeks | Used for short tolerability windows or budget-limited plans. |
Off-cycle periods are commonly described in protocol summaries as a way to reduce the risk of receptor desensitization with sustained ghrelin-receptor stimulation.
DAC vs No-DAC Decision
CJC-1295 comes in two forms. CJC-1295 without DAC has a 30-minute to 2-hour half-life and is the standard pairing for Ipamorelin because their pulse timing matches. CJC-1295 with DAC carries a Drug Affinity Complex that binds it to albumin, extending half-life to 5.8-8.1 days (Teichman 2006, JCEM). DAC is dosed weekly or biweekly and produces sustained GHRH stimulation that does not pair cleanly with Ipamorelin's pulsatile mechanism.
Injection Timing
- Inject on an empty stomach. Most planning summaries suggest 2-3 hours after the last meal because elevated insulin and blood glucose blunt GH release.
- Wait roughly 20-30 minutes after injecting before eating.
- Pre-bed timing is the most common single-dose window because it amplifies the natural nocturnal GH pulse.
- Twice-daily plans most often use morning (fasted) and pre-bed.
- Rotate injection sites between abdomen, thigh, and upper arm to reduce local irritation.
CJC-1295 + Ipamorelin Supplies Needed
Plan based on once-daily dosing from a 20 mg pre-blended vial (10 mg + 10 mg) reconstituted with 3.0 mL BAC water. Separate-vial planning will use roughly the same syringe and swab counts because the schedule is identical.
Recommended USA Supply
Use discount code SAVE10 at Peptira checkout. See why we love Peptira.
Ipamorelin + CJC Blend

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials (20 mg blend)
1 vial covers about 50 daily draws at 200 mcg of each peptide or about 33 daily draws at 300 mcg of each. Counts below assume titration into the 200-300 mcg target range.
| Cycle length | Planning note |
|---|---|
4 weeks 1 vial | Titration low; 1 vial leaves substantial margin. |
8 weeks 1-2 vials | 1 vial covers the standard 100 -> 200 mcg titration; 2 vials if escalating early or adding margin. |
12 weeks 2 vials | Covers the most common cycle length at 200-300 mcg of each peptide. |
16 weeks 3 vials | Extended cycle planning with margin for 300 mcg maintenance. |
4 weeks
1 vial
Titration low; 1 vial leaves substantial margin.
8 weeks
1-2 vials
1 vial covers the standard 100 -> 200 mcg titration; 2 vials if escalating early or adding margin.
12 weeks
2 vials
Covers the most common cycle length at 200-300 mcg of each peptide.
16 weeks
3 vials
Extended cycle planning with margin for 300 mcg maintenance.
Insulin Syringes (U-100, 30- or 50-unit preferred)
1 syringe per daily injection. Use the smaller barrels for better readability on draws under 0.10 mL.
| Cycle length | Planning note |
|---|---|
4 weeks 28 syringes | 1 per day. |
8 weeks 56 syringes | 1 per day. |
12 weeks 84 syringes | 1 per day. |
16 weeks 112 syringes | 1 per day. |
4 weeks
28 syringes
1 per day.
8 weeks
56 syringes
1 per day.
12 weeks
84 syringes
1 per day.
16 weeks
112 syringes
1 per day.
Bacteriostatic Water
Use 3.0 mL per 20 mg blend vial.
| Cycle length | Planning note |
|---|---|
4-16 weeks 1 x 10 mL bottle | 4 weeks: 1 vial uses 3 mL total.; 8 weeks: 1-2 vials use 3-6 mL total.; 12 weeks: 2 vials use 6 mL total.; 16 weeks: 3 vials use 9 mL total. |
4-16 weeks
1 x 10 mL bottle
4 weeks: 1 vial uses 3 mL total.; 8 weeks: 1-2 vials use 3-6 mL total.; 12 weeks: 2 vials use 6 mL total.; 16 weeks: 3 vials use 9 mL total.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments.
Companion Supplies & Routine Support
CJC-1295 + Ipamorelin Dosage Chart
This CJC-1295 + Ipamorelin dosage chart summarizes the pre-blended CJC-1295 and ipamorelin titration ranges shown in the dosing section above.
CJC-1295 + Ipamorelin Reconstitution Guide
Reconstitution by Format
Match reconstitution to the vial type you are using.
20 mg blend (10 mg + 10 mg) at 1:1 ratio.
20 mg blend reconstitution math
BAC water
2.0 mL
Total concentration
10.0 mg/mL total (5.0 mg/mL each)
Per peptide
5.0 mg/mL
Common 200 mcg dose
4 units (0.04 mL)
BAC water
2.5 mL
Total concentration
8.0 mg/mL total (4.0 mg/mL each)
Per peptide
4.0 mg/mL
Common 200 mcg dose
5 units (0.05 mL)
BAC water
3.0 mL
Total concentration
6.67 mg/mL total (3.33 mg/mL each)
Per peptide
3.33 mg/mL
Common 200 mcg dose
6 units (0.06 mL)
| BAC water | Total concentration | Per peptide | Common 200 mcg dose |
|---|---|---|---|
| 2.0 mL | 10.0 mg/mL total (5.0 mg/mL each) | 5.0 mg/mL | 4 units (0.04 mL) |
| 2.5 mL | 8.0 mg/mL total (4.0 mg/mL each) | 4.0 mg/mL | 5 units (0.05 mL) |
| 3.0 mL | 6.67 mg/mL total (3.33 mg/mL each) | 3.33 mg/mL | 6 units (0.06 mL) |
3.0 mL is the maximum fill used for this 20 mg blend math. Do not use higher BAC water volumes unless the vial is confirmed to hold more.
10 mg CJC-1295 + 10 mg Ipamorelin in independent vials.
10 mg vial reconstitution math
Vial
CJC-1295 10 mg
BAC water
3.0 mL
Concentration
3.33 mg/mL
200 mcg dose
6 units (0.06 mL)
Vial
Ipamorelin 10 mg
BAC water
3.0 mL
Concentration
3.33 mg/mL
200 mcg dose
6 units (0.06 mL)
| Vial | BAC water | Concentration | 200 mcg dose |
|---|---|---|---|
| CJC-1295 10 mg | 3.0 mL | 3.33 mg/mL | 6 units (0.06 mL) |
| Ipamorelin 10 mg | 3.0 mL | 3.33 mg/mL | 6 units (0.06 mL) |
This separate-vial reference uses 3.0 mL as the maximum fill for the same vial-capacity constraint.
Step-by-Step Reconstitution
- 01
Inspect the vial
Check label, lot, and appearance. The lyophilized powder should be intact and the vial should be sealed.
- 02
Wipe the stopper
Wipe the vial stopper with a fresh alcohol prep pad and let it air dry.
- 03
Draw BAC water
Draw the planned volume of bacteriostatic water with a sterile syringe (3.0 mL for the 20 mg blend or 10 mg separate vials).
- 04
Inject down the wall
Insert the needle and slowly inject the BAC water down the inside wall of the vial. Do not spray it directly onto the powder.
- 05
Swirl, do not shake
Gently roll or swirl the vial until the powder dissolves. Shaking can damage the peptide.
- 06
Label and store
Label the vial with the date and concentration. Refrigerate at 35.6-46.4 F (2-8 C), shielded from light.
- 07
Calculate the draw
Use the dosing tab math above. Use a fresh sterile insulin syringe each time you draw a dose.
Need a calculator?
Use the PepPal peptide stack calculator to confirm any custom BAC volume or dose.
Why CJC-1295 and Ipamorelin Work Together
Most peptide stacks combine compounds that work through similar pathways. This stack does the opposite. CJC-1295 (no DAC) and Ipamorelin trigger growth hormone release through two completely different receptor systems on the same pituitary cells.
Two Pathways, One Pulse
CJC-1295 is a 30-amino-acid GHRH analog. It binds GHRH receptors on pituitary somatotrophs, the cells that produce GH. Its short half-life (30 minutes to 2 hours) preserves the body's natural pulsatile signaling pattern. Think of it as the production-side signal: tell the pituitary to make GH and prepare to release it.
Ipamorelin is a 5-amino-acid pentapeptide that binds the ghrelin receptor (GHSR1a) on the same pituitary cells. Activating that receptor triggers a calcium-dependent release of GH that amplifies whatever GHRH signaling is already in progress. Think of it as the release-side signal: trigger the actual GH pulse.
Cellular work suggests these two pathways do not just add up — they multiply. A 2002 study (Cunha & Mayo) showed that active ghrelin-receptor signaling potentiates GHRH signaling on the same cell.
Why Ipamorelin Specifically
Older growth hormone secretagogues like GHRP-2 and GHRP-6 also bind the ghrelin receptor, but they elevate cortisol, prolactin, and appetite. Ipamorelin does not. Raun et al. (1998) showed no significant cortisol or ACTH elevation even at 200 times the effective GH-releasing dose. That selectivity is the reason Ipamorelin became the default GHRP for research planning.
- CJC-1295 (no DAC): production-side signal via the GHRH receptor.
- Ipamorelin: release-side signal via the ghrelin receptor (GHSR1a).
- Combined effect is widely described as synergistic in preclinical and pharmacology literature; no published human RCT has tested the exact blend at common research-planning doses.
CJC-1295 + Ipamorelin Side Effects & Safety
Compound-Level Effects
- Facial flushing or warmth in the first 5-10 minutes after injection (more common with CJC-1295 than Ipamorelin).
- Mild water retention in the first 1-2 weeks of a cycle that often stabilizes.
- Vivid dreams or improved sleep depth, attributed to GH's effect on slow-wave sleep.
- A small bump in hunger 20-30 minutes after Ipamorelin dosing; less pronounced than GHRP-6.
- Mild injection-site irritation; reduced by site rotation and proper technique.
Stack-Specific Unknowns
No published human RCT has evaluated the CJC-1295 (no DAC) + Ipamorelin combination at the daily 200-300 mcg planning doses common online. Side-effect summaries above are extrapolated from the individual compounds and from supervised clinic use of similar GHRH + GHRP combinations. Long-term safety data beyond 90 days is limited even for the individual compounds.
Concerns That Require Attention
- Cancer history: GH and IGF-1 promote cell proliferation. Anyone with active cancer, prior cancer history, or unscreened tumors should not use any GH-stimulating peptide. This applies to CJC-1295, Ipamorelin, and all other secretagogues.
- Carpal tunnel-style symptoms (tingling, numbness in hands) signal excessive GH or IGF-1; reduce dose or pause.
- Blood glucose: GH is counter-regulatory to insulin. People with diabetes, insulin resistance, or pre-diabetes need to monitor closely.
- Persistent joint pain past the first 2 weeks is a signal to reduce dose.
- Immunogenicity (rare allergic-type reactions) was named in FDA review documents for ipamorelin and CJC-1295.
Monitoring
- IGF-1 baseline before starting, then mid-cycle (week 6-8) and 4 weeks post-cycle.
- Fasting glucose and HbA1c if metabolic risk factors are present.
- Joint and hand symptoms throughout the cycle.
- Optional: thyroid panel if running multi-month plans, since long-term GH stimulation studies have flagged hypothyroidism in a minority of users.
Quality Control
Because no GH peptide is FDA-approved, product quality varies between research suppliers. A current Certificate of Analysis (COA) for the specific lot is the minimum quality signal. Independent testing platforms like Finnrick add a second layer of verification. Buying from a supplier with no current public testing is a real risk.
CJC-1295 + Ipamorelin Timeline & What to Monitor
Effects from this stack are typically described in stages because the underlying changes (GH and IGF-1 elevation, then downstream tissue and metabolic shifts) build over time.
Common research-planning timeline (anecdotal aggregation)
Window
Weeks 1-2
What is commonly reported
Improved sleep depth, more vivid dreams, mild water retention.
What is being measured
Subjective sleep, recovery.
Window
Weeks 3-4
What is commonly reported
Better recovery from training, reduced soreness.
What is being measured
Subjective recovery, training tolerance.
Window
Weeks 5-8
What is commonly reported
Body composition shifts begin (lean mass, fat distribution).
What is being measured
Body weight, waist circumference, optional DEXA.
Window
Weeks 8-12
What is commonly reported
Plateauing of subjective effects; receptor sensitivity discussion begins.
What is being measured
IGF-1, glucose, joint symptoms.
Window
Post-cycle (4 weeks)
What is commonly reported
Subjective effects taper as GH/IGF-1 axis returns toward baseline.
What is being measured
Repeat IGF-1 to confirm return to baseline.
| Window | What is commonly reported | What is being measured |
|---|---|---|
| Weeks 1-2 | Improved sleep depth, more vivid dreams, mild water retention. | Subjective sleep, recovery. |
| Weeks 3-4 | Better recovery from training, reduced soreness. | Subjective recovery, training tolerance. |
| Weeks 5-8 | Body composition shifts begin (lean mass, fat distribution). | Body weight, waist circumference, optional DEXA. |
| Weeks 8-12 | Plateauing of subjective effects; receptor sensitivity discussion begins. | IGF-1, glucose, joint symptoms. |
| Post-cycle (4 weeks) | Subjective effects taper as GH/IGF-1 axis returns toward baseline. | Repeat IGF-1 to confirm return to baseline. |
These windows are aggregated from clinic and research-community summaries, not from a single controlled trial of the blend.
CJC-1295 + Ipamorelin Clinical Evidence Context
Direct stack evidence
No published human randomized trial has evaluated the CJC-1295 (no DAC) + Ipamorelin combination at the daily 200-300 mcg doses common in online research planning. Evidence below covers each compound separately and is extrapolated to the blend.
CJC-1295 with DAC (human)
Teichman et al., 2006 (JCEM): 24 healthy adults, ascending single and multiple SubQ doses, 28 and 49-day arms. GH increased 2-10 fold for 6+ days; IGF-1 increased 1.5-3 fold for 9-11 days. Estimated half-life 5.8-8.1 days. Note: this is the DAC variant, not the no-DAC form most often paired with Ipamorelin.
CJC-1295 with DAC, pulsatility (human)
Ionescu & Frohman, 2006 (JCEM): showed that pulsatile GH secretion persists during continuous CJC-1295 stimulation, with GH pulse frequency and timing preserved.
CJC-1295, animal model
Alba et al., 2006 (Endocrinology): once-daily CJC-1295 normalized growth in a GHRH-knockout mouse, supporting the GHRH-receptor mechanism.
Ipamorelin selectivity
Raun et al., 1998 (Eur J Endocrinol): Ipamorelin produced GH release without elevating ACTH or cortisol, even at 200x the effective GH-releasing dose. This is the foundational selectivity paper.
Ipamorelin pharmacokinetics (human)
Gobburu et al., 1999 (J Clin Pharmacol): pharmacokinetic-pharmacodynamic modeling of Ipamorelin in healthy volunteers; GH peak around 40 minutes post-dose, half-life roughly 1.5-2.5 hours.
Stack-level mechanism (cell)
Cunha & Mayo, 2002 (Endocrinology): demonstrated that active ghrelin-receptor signaling potentiates GHRH receptor signaling on the same pituitary cell, providing the mechanistic case for combining GHRH + GHRP.
Direct stack evidence
No published human RCT has tested CJC-1295 (no DAC) + Ipamorelin at the daily 200-300 mcg doses common online. The FDA's October 2024 PCAC review documents specifically noted limited clinical data on this combination.
CJC-1295 + Ipamorelin Storage & Handling
Storage and stability
State
Lyophilized (powder)
Storage
-4 F (-20 C) long-term, dry and dark
Shelf life
Use supplier label; commonly 24+ months when stored cold and dry.
State
Reconstituted (liquid)
Storage
35.6-46.4 F (2-8 C), refrigerated, shielded from light
Shelf life
Most planning summaries use within 28-30 days. Discard sooner if cloudy, discolored, or contaminated.
State
Avoid
Storage
Repeated freeze-thaw cycles, room temperature for extended periods
Shelf life
Both peptides degrade with heat and oxidation.
| State | Storage | Shelf life |
|---|---|---|
| Lyophilized (powder) | -4 F (-20 C) long-term, dry and dark | Use supplier label; commonly 24+ months when stored cold and dry. |
| Reconstituted (liquid) | 35.6-46.4 F (2-8 C), refrigerated, shielded from light | Most planning summaries use within 28-30 days. Discard sooner if cloudy, discolored, or contaminated. |
| Avoid | Repeated freeze-thaw cycles, room temperature for extended periods | Both peptides degrade with heat and oxidation. |
Allow vials to reach room temperature before opening to reduce condensation absorption.
CJC-1295 + Ipamorelin vs Sermorelin, MK-677, and GHRP-2
Common GH-secretagogue alternatives
Comparison
Sermorelin (alone or with Ipamorelin)
vs CJC-1295 + Ipamorelin
Sermorelin is the original GHRH analog (FDA-approved 1997 for pediatric GH deficiency, withdrawn 2008). Stronger human evidence base, but very short half-life (10-12 minutes) and lower bioavailability. Pairs with Ipamorelin similarly. Researchers often choose Sermorelin when published evidence depth matters more than convenience.
Comparison
Tesamorelin + Ipamorelin blend
vs CJC-1295 + Ipamorelin
The Tesamorelin + Ipamorelin blend swaps CJC-1295 for tesamorelin, an FDA-approved GHRH analog in HIV-associated lipodystrophy. It uses different vial ratios and dose math, so it should be planned from its own protocol rather than treated as a CJC-1295 substitute.
Comparison
CJC-1295 with DAC alone
vs CJC-1295 + Ipamorelin
DAC's 5.8-8.1 day half-life enables weekly dosing and is more convenient, but produces sustained GHRH stimulation rather than pulses. Pairs poorly with Ipamorelin's pulsatile mechanism. Better suited for standalone weekly plans.
Comparison
MK-677 (Ibutamoren)
vs CJC-1295 + Ipamorelin
Oral ghrelin mimetic. No injections, but produces continuous GH elevation similar to CJC-1295 DAC, with greater appetite increase and possible insulin sensitivity issues over months. CJC-1295 + Ipamorelin offers more precise timing control.
Comparison
GHRP-2 + GHRH analog
vs CJC-1295 + Ipamorelin
GHRP-2 is more potent at raw GH stimulation than Ipamorelin. But GHRP-2 elevates cortisol, prolactin, and appetite (food intake increased ~36% in one study). Researchers who want minimal cortisol and prolactin impact choose Ipamorelin.
| Comparison | vs CJC-1295 + Ipamorelin |
|---|---|
| Sermorelin (alone or with Ipamorelin) | Sermorelin is the original GHRH analog (FDA-approved 1997 for pediatric GH deficiency, withdrawn 2008). Stronger human evidence base, but very short half-life (10-12 minutes) and lower bioavailability. Pairs with Ipamorelin similarly. Researchers often choose Sermorelin when published evidence depth matters more than convenience. |
| Tesamorelin + Ipamorelin blend | The Tesamorelin + Ipamorelin blend swaps CJC-1295 for tesamorelin, an FDA-approved GHRH analog in HIV-associated lipodystrophy. It uses different vial ratios and dose math, so it should be planned from its own protocol rather than treated as a CJC-1295 substitute. |
| CJC-1295 with DAC alone | DAC's 5.8-8.1 day half-life enables weekly dosing and is more convenient, but produces sustained GHRH stimulation rather than pulses. Pairs poorly with Ipamorelin's pulsatile mechanism. Better suited for standalone weekly plans. |
| MK-677 (Ibutamoren) | Oral ghrelin mimetic. No injections, but produces continuous GH elevation similar to CJC-1295 DAC, with greater appetite increase and possible insulin sensitivity issues over months. CJC-1295 + Ipamorelin offers more precise timing control. |
| GHRP-2 + GHRH analog | GHRP-2 is more potent at raw GH stimulation than Ipamorelin. But GHRP-2 elevates cortisol, prolactin, and appetite (food intake increased ~36% in one study). Researchers who want minimal cortisol and prolactin impact choose Ipamorelin. |
These compounds are not interchangeable. Each has a different pharmacology, side-effect profile, and regulatory status.
CJC-1295 + Ipamorelin Regulatory Status
As of June 2026, neither CJC-1295 nor Ipamorelin is FDA-approved for any clinical use. Both compounds have been the subject of recent compounding-pharmacy regulatory review.
- September 2023: FDA placed multiple peptides — including CJC-1295 (free base, acetate, DAC variants) and ipamorelin (acetate and free base) — on Category 2 of the interim 503A bulks list, signaling significant safety or evidence concerns and effectively halting routine 503A compounding.
- September 2024: After a settlement and withdrawn nominations, the FDA removed certain peptides from Category 2 and scheduled PCAC (Pharmacy Compounding Advisory Committee) review meetings.
- October 29, 2024: PCAC reviewed ipamorelin acetate and ipamorelin (free base). FDA recommended against inclusion in the 503A Bulks Regulation.
- December 4, 2024: PCAC reviewed AOD-9604, CJC-1295 (free base, acetate, DAC variants), and thymosin alpha-1.
- February 2026: HHS Secretary Robert F. Kennedy Jr. publicly indicated intent to reclassify multiple peptides toward Category 1; formal FDA action and revised lists have not been published as of June 2026. Reclassification timing is uncertain.
- Both compounds remain widely available through research-grade peptide suppliers operating under 'research use only, not for human consumption' labeling. Research-grade product is not equivalent to FDA-approved or compounded medicine.
Regulatory uncertainty
The 2026 reclassification picture is moving. Always check FDA.gov and the Federal Register for the most current 503A list and any new guidance before making purchasing or research-planning decisions.
CJC-1295 + Ipamorelin GH Pulse Stack Blood Tests & Monitoring
This stack combines a GHRH analog with a GH secretagogue, so monitoring centers on GH-axis activity. The key areas are IGF-1, glucose handling, lipids, thyroid context, and fluid-retention symptoms.
Blood test markers to discuss with a clinician
Marker
IGF-1
Why it matters
Shows the downstream signal after repeated GH-pulse stimulation.
Timing
Follow-up
Marker
A1c
Why it matters
Tracks longer-term glucose control because GH-axis changes may affect insulin sensitivity.
Timing
Baseline
Marker
Fasting glucose
Why it matters
Gives a current glucose snapshot before and during GH-axis protocols.
Timing
Follow-up
Marker
Lipid panel
Why it matters
Reviews cholesterol and triglyceride trends during body-composition or GH-axis changes.
Timing
Baseline
Marker
TSH and free T4
Why it matters
Thyroid status can affect energy, weight, and GH-axis interpretation.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| IGF-1 | Shows the downstream signal after repeated GH-pulse stimulation. | Follow-up |
| A1c | Tracks longer-term glucose control because GH-axis changes may affect insulin sensitivity. | Baseline |
| Fasting glucose | Gives a current glucose snapshot before and during GH-axis protocols. | Follow-up |
| Lipid panel | Reviews cholesterol and triglyceride trends during body-composition or GH-axis changes. | Baseline |
| TSH and free T4 | Thyroid status can affect energy, weight, and GH-axis interpretation. | Optional |
Monitoring guidance is GH-axis pathway-based and extrapolated from GHRH analog and GH secretagogue physiology.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with diabetes risk, sleep apnea, edema, thyroid disease, cancer history, or pituitary history.
Follow-up
Re-check IGF-1 and metabolic markers after 6-8 weeks or after meaningful protocol changes.
Longer term
For longer protocols, review GH-axis and metabolic trends every 3-6 months with a clinician.
How to interpret the labs
- IGF-1 should be interpreted with age, symptoms, baseline levels, and protocol duration.
- Fluid retention, joint pain, numbness, sleep apnea symptoms, appetite changes, and glucose changes matter.
- Cancer history or active malignancy concerns need clinician review before GH-axis stimulation is considered.
Do not wait for routine labs
Rapid swelling, severe headaches, vision changes, chest pain, shortness of breath, or allergic symptoms need medical review. New numbness, wrist pain, or worsening sleep apnea symptoms should be discussed with a clinician.
FAQ
Q1: What does the CJC-1295 + Ipamorelin stack do?
It stimulates the body's own growth hormone release through two separate receptor pathways. CJC-1295 (no DAC) hits GHRH receptors on the pituitary, telling the pituitary to make GH. Ipamorelin hits the ghrelin receptor on the same cells, triggering the actual GH pulse. The combination is described in pharmacology literature as synergistic. Neither compound is FDA-approved for any clinical use.
Q2: What is the standard CJC-1295 + Ipamorelin dosage?
The most common research-planning range is 100-300 mcg of each peptide, injected subcutaneously once daily on an empty stomach. A typical pre-blended 20 mg vial (10 mg + 10 mg) reconstituted with 3.0 mL bacteriostatic water gives a clean 6-unit insulin draw for 200 mcg of each peptide. This is research-planning context, not a personal dosing recommendation.
Q3: Should I use CJC-1295 with or without DAC?
Without DAC for Ipamorelin pairing. The no-DAC variant has a 30-minute to 2-hour half-life that matches Ipamorelin's roughly 2-hour half-life, which preserves the body's natural pulsatile GH release. CJC-1295 with DAC has a 5.8-8.1 day half-life and produces sustained GHRH stimulation that does not pair cleanly with Ipamorelin's pulse-based mechanism.
Q4: How is the 20 mg blend reconstituted?
The featured research-planning approach is 3.0 mL of bacteriostatic water, which gives 6.67 mg/mL total concentration (3.33 mg/mL of each peptide). On a U-100 insulin syringe, 3 units delivers 100 mcg of each peptide, 6 units delivers 200 mcg, and 9 units delivers 300 mcg. Use the reconstitution section for lower BAC water volumes when smaller draw volumes are needed.
Q5: How long is a typical cycle?
Most research-planning cycles run 8-12 weeks on, followed by 4 weeks off. Extended plans go 16 weeks on, 8 weeks off. Off-cycle periods are commonly described as a way to reduce the chance of receptor desensitization with sustained ghrelin-receptor stimulation. Long-term safety beyond 90 days has not been studied for the combined blend.
Q6: What supplies are needed for one cycle?
For an 8-week once-daily plan on a 20 mg pre-blended vial: plan on 1-2 vials of CJC-1295 + Ipamorelin, 56 insulin syringes (U-100, 30- or 50-unit barrel preferred), 1 x 10 mL bottle of bacteriostatic water, and 2 x 100-count boxes of alcohol swabs. See the supplies section for cycle-by-cycle math.
Q7: What are the main side effects?
Commonly reported: temporary facial flushing, mild water retention in the first 1-2 weeks, vivid dreams, deeper sleep, and a small post-injection hunger bump from Ipamorelin. Concerns that require attention: carpal tunnel-style tingling (signals excessive GH/IGF-1), elevated fasting glucose, persistent joint pain, and rare immunogenicity reactions. Anyone with active or prior cancer, pituitary disease, diabetic retinopathy, severe kidney disease, or pregnancy should not use GH-stimulating peptides.
Q8: Are CJC-1295 and Ipamorelin FDA-approved?
No. As of June 2026, neither compound is FDA-approved for any clinical use. Both were placed on FDA Category 2 in September 2023, removed in September 2024 after withdrawn nominations, and reviewed by PCAC in late 2024 with FDA recommending against 503A Bulks inclusion. Reclassification discussions in 2026 are ongoing but no formal change has been published. See the regulatory status section for the timeline.
Q9: Is there direct human research on the CJC-1295 + Ipamorelin blend?
No published human randomized trial has tested the CJC-1295 (no DAC) + Ipamorelin combination at the daily 200-300 mcg doses common online. The case for the stack rests on each compound's individual human pharmacokinetic data plus cellular and animal evidence that the two pathways are synergistic on the same pituitary cell.
Q10: Is this medical advice?
No. This page is an educational research reference. It summarizes published pharmacology, clinical-trial dosing context, and common protocol planning patterns. It is not a personal dosing recommendation and is not a substitute for guidance from a licensed clinician.
Sources & Research
- 1. Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA Prolonged Stimulation of Growth Hormone (GH) and Insulin-Like Growth Factor I Secretion by CJC-1295, a Long-Acting Analog of GH-Releasing Hormone, in Healthy Adults. Journal of Clinical Endocrinology & Metabolism (JCEM) (2006)
- 2. Ionescu M, Frohman LA Pulsatile Secretion of Growth Hormone (GH) Persists during Continuous Stimulation by CJC-1295, a Long-Acting GH-Releasing Hormone Analog. Journal of Clinical Endocrinology & Metabolism (JCEM) (2006)
- 3. Alba M, Fintini D, Sagazio A, Lawrence B, Castaigne JP, Frohman LA, Salvatori R Once-daily administration of CJC-1295, a long-acting growth hormone-releasing hormone (GHRH) analog, normalizes growth in the GHRH knockout mouse. American Journal of Physiology / Endocrinology (2006)
- 4. Raun K, Hansen BS, Johansen NL, Thøgersen H, Madsen K, Ankersen M, Andersen PH Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology (1998)
- 5. Gobburu JV, Agersø H, Jusko WJ, Ynddal L Pharmacokinetic-pharmacodynamic modeling of ipamorelin, a growth hormone releasing peptide, in human volunteers. Pharmaceutical Research (1999)
- 6. Cunha SR, Mayo KE Ghrelin and growth hormone (GH) secretagogues potentiate GH-releasing hormone (GHRH)-induced cyclic adenosine 3',5'-monophosphate production in cells expressing transfected GHRH and GH secretagogue receptors. Endocrinology (2002)
- 7. Sackmann-Sala L, Ding J, Frohman LA, Kopchick JJ Activation of the GH/IGF-1 axis by CJC-1295, a long-acting GHRH analog, results in serum protein profile changes in normal adult subjects. Growth Hormone & IGF Research (2009)
- 8. Sigalos JT, Pastuszak AW The Safety and Efficacy of Growth Hormone Secretagogues. Sexual Medicine Reviews / PMC (2018)
- 9. U.S. Food and Drug Administration FDA Briefing Document, Pharmacy Compounding Advisory Committee (PCAC) Meeting — Ipamorelin Acetate and Ipamorelin (free base). FDA.gov (2024)
- 10. U.S. Food and Drug Administration Interim 503A Bulks List — Category 2 / PCAC review notices for CJC-1295 (free base, acetate, DAC variants), ipamorelin, AOD-9604, and thymosin alpha-1. FDA.gov / Federal Register (2024)
- 11. Junnila RK, List EO, Berryman DE, Murrey JW, Kopchick JJ The GH/IGF-1 axis in ageing and longevity. Nature Reviews Endocrinology (2013)
- 12. Sinha DK, Balasubramanian A, Tatem AJ, et al. Beyond the androgen receptor: the role of growth hormone secretagogues in the modern management of body composition in hypogonadal males. Translational Andrology and Urology / PMC (2020)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page