GHRP-6 Quick Start
GHRP-6 stands for growth hormone releasing peptide-6. It is a small synthetic peptide (six amino acids) that copies part of how the hunger hormone ghrelin works. Instead of adding growth hormone (GH) from outside, it signals your own pituitary gland to release a pulse of GH. It was the first peptide of its kind, described by Cyril Bowers in 1984.
Two honest points up front. First, GHRP-6's standout trait is strong appetite stimulation — the most of any peptide in its family. That can help someone trying to eat more, but it works against most fat-loss or lean-physique goals. Second, the GH rise is real but modest compared with injectable HGH, so results depend heavily on training, sleep, and nutrition. It is most often paired with a GHRH analog (like CJC-1295 / mod GRF 1-29 or sermorelin) because the two together produce a bigger GH pulse than either alone.
How it works
Activates the ghrelin receptor (GHS-R1a) to trigger a natural GH pulse.
Signature effect
Intense hunger within minutes; useful for some, a drawback for others.
Timing rule
Food, especially carbs and fat, blunts the GH response, so it is used on an empty stomach.
Status
Not FDA-approved, research-use-only, and WADA-banned in sport.
Educational use only
This page is an educational research reference, not medical advice or a treatment plan. GHRP-6 is not FDA-approved and is prohibited in sport by WADA. Talk to a qualified clinician before considering any peptide, and never start an injectable peptide without medical supervision.
GHRP-6 Dosing Protocol & Schedule
Most GHRP-6 dosing discussions come back to two practical ideas: the saturation dose and meal timing. The saturation dose is the point where adding more peptide is unlikely to add much more GH response, and food near the injection window can blunt the pulse. The figures below are educational only, not dosing instructions.
GHRP-6 Dosing Guide
GHRP-6 is used either on its own or paired with a GHRH analog. The two approaches are shown below.
The simplest research structure: GHRP-6 by itself.
Most research-use discussions describe 100-300 mcg per SubQ injection, taken three times daily at least 4 hours apart. Common timing is morning, midday, and bedtime. Each injection is usually placed on an empty stomach, about 2-3 hours after a meal and 30 minutes before eating. Because GHRP-6 is short acting, multiple daily injections are discussed more often than once-daily dosing. This is educational only, not a dosing recommendation.
Cycles described online often run several weeks to a few months. There is no regulator-set schedule, and no controlled human trial validates a GHRP-6 schedule for muscle gain or fat loss.
Why the mod GRF / CJC-1295 / sermorelin blends are searched so often.
GHRP-6 and a GHRH analog work on two different receptors, and human studies show the GH response to the two together is larger than to either one alone. That is the logic behind the popular blends: mod GRF 1-29 (CJC-1295 without DAC) + GHRP-6, CJC-1295 + GHRP-6, or sermorelin + GHRP-6.
When GHRP-6 is paired with a GHRH analog, research-use discussions usually place both injections in the same dosing window, often at similar microgram amounts. The same empty-stomach timing still applies. This is not a dosing recommendation.
Related stack
For the broader GH-pulse stacking idea, see the CJC-1295 + Ipamorelin GH Pulse stack guide.
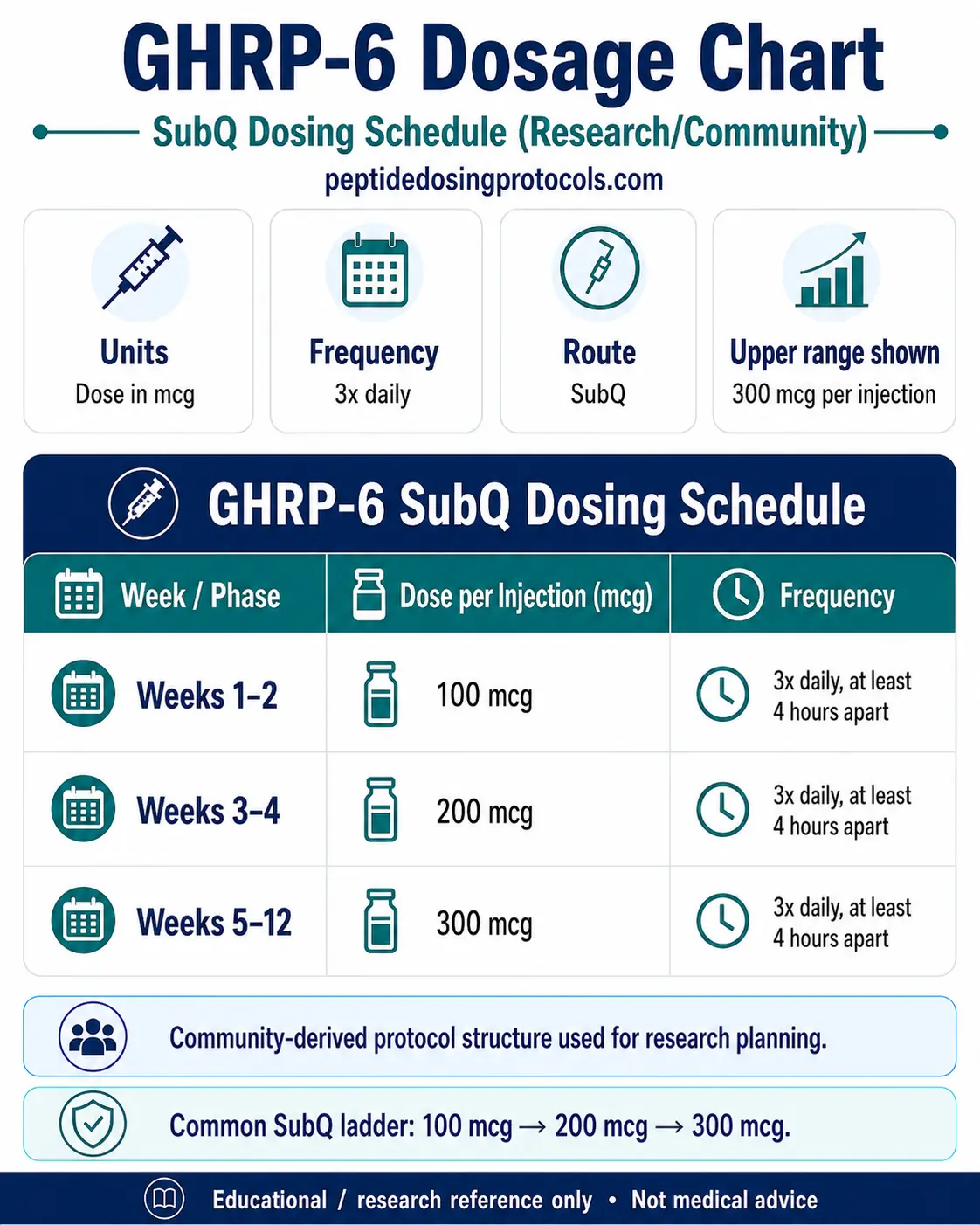
SubQ Dosing Schedule (Research/Community)
Week / Phase
Weeks 1-2
Dose per Injection (mcg)
100 mcg
Frequency
3x daily, at least 4 hours apart
Week / Phase
Weeks 3-4
Dose per Injection (mcg)
200 mcg
Frequency
3x daily, at least 4 hours apart
Week / Phase
Weeks 5-12
Dose per Injection (mcg)
300 mcg
Frequency
3x daily, at least 4 hours apart
| Week / Phase | Dose per Injection (mcg) | Frequency |
|---|---|---|
| Weeks 1-2 | 100 mcg | 3x daily, at least 4 hours apart |
| Weeks 3-4 | 200 mcg | 3x daily, at least 4 hours apart |
| Weeks 5-12 | 300 mcg | 3x daily, at least 4 hours apart |
Educational only. Each injection is commonly timed on an empty stomach, about 2-3 hours after meals and 30 minutes before eating. This is not a dosing recommendation.
This is not a dosing recommendation
Do not treat GHRP-6 like a casual supplement. The figures here are educational only. GHRP-6 is not FDA-approved, can affect hunger and blood sugar, and should be discussed with a qualified clinician before any use.
GHRP-6 Supplies Needed
This supply planner assumes a 5 mg vial mixed with 3 mL bacteriostatic water, with dosing stepped from 100 mcg to 300 mcg per injection. The math uses three injections per day.
Recommended USA Supply
Use discount code SAVE10 at Peptira checkout. See why we love Peptira.

GHRP-6 Supply

At-Home Blood Test
Research Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials
A 5 mg vial reconstituted with 3 mL BAC water gives about 1,667 mcg/mL. The vial counts below follow the 100 mcg, 200 mcg, and 300 mcg step-up schedule at three injections per day.
| Cycle length | Planning note |
|---|---|
4 weeks 3 vials | ~12.6 mg total peptide needed. |
6 weeks 6 vials | ~25.2 mg total peptide needed. |
8 weeks 8 vials | ~37.8 mg total peptide needed. |
12 weeks 13 vials | ~63 mg total peptide needed. |
4 weeks
3 vials
~12.6 mg total peptide needed.
6 weeks
6 vials
~25.2 mg total peptide needed.
8 weeks
8 vials
~37.8 mg total peptide needed.
12 weeks
13 vials
~63 mg total peptide needed.
Insulin Syringes (U-100)
One syringe per injection; 0.3 mL / 30-unit barrels suit the draw volumes in this schedule.
| Cycle length | Planning note |
|---|---|
4 weeks 84 syringes | 3 injections per day |
6 weeks 126 syringes | 3 injections per day |
8 weeks 168 syringes | 3 injections per day |
12 weeks 252 syringes | 3 injections per day |
4 weeks
84 syringes
3 injections per day
6 weeks
126 syringes
3 injections per day
8 weeks
168 syringes
3 injections per day
12 weeks
252 syringes
3 injections per day
Bacteriostatic Water
Use 3 mL per 5 mg vial for reconstitution. Do not exceed a 3 mL vial capacity.
| Cycle length | Planning note |
|---|---|
4 weeks 1 x 10 mL bottle | 3 vials use 9 mL |
6 weeks 2 x 10 mL bottles | 6 vials use 18 mL |
8 weeks 3 x 10 mL bottles | 8 vials use 24 mL |
12 weeks 4 x 10 mL bottles | 13 vials use 39 mL |
4 weeks
1 x 10 mL bottle
3 vials use 9 mL
6 weeks
2 x 10 mL bottles
6 vials use 18 mL
8 weeks
3 x 10 mL bottles
8 vials use 24 mL
12 weeks
4 x 10 mL bottles
13 vials use 39 mL
Round up for priming losses, dropped syringes, and damaged swabs. If you stack GHRP-6 with a GHRH analog in separate vials, double the syringe and vial planning for the second compound.
Companion Supplies & Routine Support
GHRP-6 Reconstitution Guide
GHRP-6 comes as a freeze-dried (lyophilized) powder, most commonly in a 5 mg vial. You mix it with bacteriostatic water before use. The math below assumes a 5 mg vial with 3 mL bacteriostatic water, which is the max-volume assumption used on this page.
Reconstitution Math (5 mg vial, 3 mL BAC water)
Dose
100 mcg
Concentration
~1,667 mcg/mL
Dose volume
0.06 mL
U-100 units
6 units
Dose
200 mcg
Concentration
~1,667 mcg/mL
Dose volume
0.12 mL
U-100 units
12 units
Dose
300 mcg
Concentration
~1,667 mcg/mL
Dose volume
0.18 mL
U-100 units
18 units
| Dose | Concentration | Dose volume | U-100 units |
|---|---|---|---|
| 100 mcg | ~1,667 mcg/mL | 0.06 mL | 6 units |
| 200 mcg | ~1,667 mcg/mL | 0.12 mL | 12 units |
| 300 mcg | ~1,667 mcg/mL | 0.18 mL | 18 units |
This assumes 5 mg total peptide divided by 3 mL BAC water. Do not use examples above 3 mL when the vial cannot safely hold more than 3 mL.
- Let the vial and bacteriostatic water reach room temperature.
- Wipe both rubber stoppers with a fresh alcohol swab.
- Draw the chosen volume of bacteriostatic water into a syringe.
- Aim the water down the inside glass wall, not directly onto the powder.
- Do not shake. Swirl gently or let it sit until the powder fully dissolves.
- The solution should look clear and colorless; discard if cloudy or full of particles.
- Label with the date and store refrigerated.
Check your numbers
Use the calculator for custom vial size, water volume, and syringe-unit math before drawing a dose.
GHRP-6 Dosage Chart
This GHRP-6 dosage chart summarizes the SubQ research schedule from 100 mcg to 300 mcg per injection, with each phase shown by week range, dose, and injection frequency.
How GHRP-6 Works
In plain terms, GHRP-6 acts like the hunger hormone ghrelin. It binds a receptor in the pituitary and brain and tells the body to release a short burst of its own growth hormone. That burst then raises IGF-1, the downstream signal tied to recovery and tissue growth.
Technically, GHRP-6 is an agonist at the growth hormone secretagogue receptor 1a (GHS-R1a), the same receptor ghrelin uses. This pathway is separate from growth hormone-releasing hormone (GHRH), which is why combining GHRP-6 with a GHRH analog produces a bigger pulse than either alone. The same receptor also drives appetite in the hypothalamus, which explains the strong hunger.
- Target: GHS-R1a (the ghrelin receptor).
- Effect: a pulse of natural GH, then a rise in IGF-1.
- Synergy: adds to GHRH-analog signaling for a larger GH pulse.
- Side note: the same receptor strongly increases appetite.
Who Should Avoid GHRP-6
Some groups should not use GHRP-6 without close medical guidance, mainly because growth hormone affects blood sugar and because of its unproven long-term safety.
- People with diabetes or insulin resistance, since GH can raise blood sugar and lower insulin sensitivity.
- People with active or prior cancer, because GH/IGF-1 signaling is a theoretical concern.
- Pregnant or breastfeeding people (safety not established).
- Competitive athletes, because GH secretagogues are banned and detectable.
This list is not complete. A qualified clinician should review your full history, medications, and lab work first.
GHRP-6 Side Effects & Safety
The most consistent effect is intense hunger, often within minutes of a dose. Other commonly reported effects include water retention or puffiness, tingling or numbness in the hands (a GH-related effect), a brief head-rush or flushing, and tiredness.
At higher doses, GHRP-6 also nudges up cortisol and prolactin, more than newer peptides like ipamorelin do. Because GH affects glucose, blood sugar and insulin sensitivity can shift, which matters most for people with diabetes or prediabetes.
Quality and blood sugar
Research-use vials are not tested or approved for human use, so purity and contamination are real risks. If you have any blood-sugar condition, GH-raising peptides deserve medical oversight and monitoring.
GHRP-6 Expected Timeline & Monitoring
The GH pulse itself happens within minutes of a dose, and appetite often spikes just as fast. But visible body-composition changes are slow and modest. Where they happen, they usually need consistent use over about 8 to 12 weeks alongside training and good nutrition. GHRP-6 is not a substitute for injectable HGH and should not be expected to match it.
One mechanism detail worth knowing: repeated high doses can blunt the response over time (desensitization), which is part of why dosing near the saturation point, not above it, is the common approach. People monitoring effects often track IGF-1 and, if relevant, fasting glucose.
GHRP-6 Clinical Evidence Context
The biology is well documented; the physique claims are not. Here is how the evidence splits.
GH release in humans — well established
Since Bowers' 1984 work, GHRP-6 has been shown to release GH in people, and it was studied as a GH-secretagogue tool for testing pituitary GH reserve. Human studies also confirmed it needs intact GHRH signaling for a maximal pulse, which is why stacks exist.
Hormonal footprint — documented
Controlled human comparisons (for example, ghrelin vs GHRP-6 vs GHRP-2) showed GHRP-6 raises GH along with measurable ACTH, cortisol, and prolactin, separating it from the cleaner profile of ipamorelin.
Cardioprotection / tissue protection — preclinical
GH secretagogues including GHRP-6 have an animal and cell literature on protecting heart and other tissue from injury. This is early, not approved, and not proven in large human trials.
Muscle, fat loss, anti-aging — thin human outcome data
Despite heavy marketing, there is little controlled human evidence that GHRP-6 produces meaningful muscle gain or fat loss on its own. The reliable effects are the GH pulse and the appetite increase.
Bottom line: GHRP-6 reliably does what its name says (it releases GH and drives hunger), but the leap to body-composition results is not well supported by controlled human trials.
GHRP-6 Storage & Handling
Storage
Lyophilized (Powder Form)
GHRP-6
-4F (-20C) long-term
Reconstituted (Liquid Form)
GHRP-6
35.6-46.4F (2-8C)
Appearance
GHRP-6
Clear, colorless
| GHRP-6 | |
|---|---|
| Lyophilized (Powder Form) | -4F (-20C) long-term |
| Reconstituted (Liquid Form) | 35.6-46.4F (2-8C) |
| Appearance | Clear, colorless |
Keep away from light and heat. Discard reconstituted solution that turns cloudy or develops particles.
Reconstituted peptide is generally used within a few weeks; follow the supplier's stated stability where available.
GHRP-6 Troubleshooting
- Cloudy vial or floating particles: do not use it.
- Weak or no effect: check timing; eating fat or carbs near a dose blunts the GH pulse.
- Overwhelming hunger: this is expected with GHRP-6; many switch to ipamorelin if hunger is unwanted.
- Tingling or numb hands: a known GH-related effect; reassess the dose with a clinician.
- Confusing the units: at about 1,667 mcg/mL, 100 mcg is about 6 units, not 100 units.
GHRP-6 Regulatory Status
As of June 2026, GHRP-6 has no FDA-approved use and no approved drug product in major regulated markets. Its close relative GHRP-2 was approved in Japan as a diagnostic agent (pralmorelin), but GHRP-6 itself has no such approval.
- US: research-use-only material, labeled not for human use; not on the FDA 503A bulks list, and GH-secretagogue peptides have generally been treated as outside routine compounding.
- Sport: prohibited by WADA at all times under Section S2 (peptide hormones and growth factors), and detectable on testing.
- Marketing: sold by research-chemical suppliers, not pharmacies; quality and labeling vary.
Regulatory categories change. Confirm current status before relying on any of the above.
GHRP-6 vs GHRP-2, Ipamorelin, MK-677 & GHRH Analogs
GHRP-6 sits in a crowded field. The quick differences below explain the most-searched comparisons.
Context Comparison
Compound
GHRP-6
Receptor / type
Ghrelin receptor (GHS)
Key difference vs GHRP-6
Strongest appetite; modest cortisol/prolactin at higher doses
Compound
GHRP-2
Receptor / type
Ghrelin receptor (GHS)
Key difference vs GHRP-6
More GH per mcg, less hunger; approved in Japan as a diagnostic
Compound
Ipamorelin
Receptor / type
Ghrelin receptor (GHS)
Key difference vs GHRP-6
Cleanest: GH pulse without meaningful hunger, cortisol, or prolactin
Compound
MK-677
Receptor / type
Ghrelin receptor (oral)
Key difference vs GHRP-6
Oral, long-acting daily GH/IGF-1 raise; not injected
Compound
CJC-1295 / sermorelin
Receptor / type
GHRH receptor
Key difference vs GHRP-6
Different receptor; paired with GHRP-6 for a bigger pulse
Compound
HGH
Receptor / type
Direct hormone
Key difference vs GHRP-6
Adds GH directly; far stronger and more controllable, but a drug
| Compound | Receptor / type | Key difference vs GHRP-6 |
|---|---|---|
| GHRP-6 | Ghrelin receptor (GHS) | Strongest appetite; modest cortisol/prolactin at higher doses |
| GHRP-2 | Ghrelin receptor (GHS) | More GH per mcg, less hunger; approved in Japan as a diagnostic |
| Ipamorelin | Ghrelin receptor (GHS) | Cleanest: GH pulse without meaningful hunger, cortisol, or prolactin |
| MK-677 | Ghrelin receptor (oral) | Oral, long-acting daily GH/IGF-1 raise; not injected |
| CJC-1295 / sermorelin | GHRH receptor | Different receptor; paired with GHRP-6 for a bigger pulse |
| HGH | Direct hormone | Adds GH directly; far stronger and more controllable, but a drug |
Different mechanisms and evidence levels. This comparison is not a ranking or recommendation.
FAQ
Q1: What is GHRP-6?
GHRP-6 (growth hormone releasing peptide-6) is a synthetic six-amino-acid peptide that activates the ghrelin receptor and signals the pituitary to release a pulse of your own growth hormone. It was the first peptide of its kind, described by Cyril Bowers in 1984, and it is the parent compound behind GHRP-2, hexarelin, and ipamorelin.
Q2: What is GHRP-6 used for?
In research it is used to study growth hormone release and was used as a tool to test pituitary GH reserve. In the grey market it is used to raise GH for recovery, body composition, and appetite. Its most reliable real-world effects are a short GH pulse and a strong increase in hunger.
Q3: How is GHRP-6 dosed?
Research-use discussions usually describe 100-300 mcg per SubQ injection on an empty stomach, often three times daily and spaced at least 4 hours apart. The common timing pattern is morning, midday, and bedtime. This is educational only, not a dosing recommendation.
Q4: GHRP-2 vs GHRP-6: what is the difference?
Both hit the same receptor, but GHRP-2 releases more GH per microgram and causes less hunger, while GHRP-6 causes the strongest appetite of any peptide in the family and raises cortisol and prolactin a bit more at higher doses. GHRP-2 was approved in Japan as a diagnostic; GHRP-6 is not approved anywhere.
Q5: GHRP-6 vs ipamorelin: which is cleaner?
Ipamorelin is usually called the cleaner option because it releases GH without meaningful appetite, cortisol, or prolactin effects. GHRP-6 produces a strong GH pulse but also strong hunger and a broader hormonal footprint. The right choice depends on whether appetite stimulation is wanted or not.
Q6: Does GHRP-6 build muscle?
On its own, the evidence for meaningful muscle gain is weak, and the GH rise is modest next to injectable HGH. Any body-composition effect tends to be slow and depends on training, sleep, and nutrition over roughly 8 to 12 weeks. It is most often stacked with a GHRH analog for a larger GH pulse.
Q7: What are the side effects of GHRP-6?
The biggest one is intense hunger. Others include water retention, tingling or numbness in the hands, a brief head-rush or flushing, and tiredness. At higher doses it can raise cortisol and prolactin, and because GH affects blood sugar, glucose and insulin sensitivity can shift.
Q8: How do you reconstitute GHRP-6?
For a common 5 mg vial, adding 3 mL of bacteriostatic water gives about 1,667 mcg/mL, where a 100 mcg dose equals about 0.06 mL or 6 units on a U-100 syringe. Add the water gently down the vial wall, do not shake, and discard if the solution is cloudy.
Q9: When should GHRP-6 be taken?
On an empty stomach, because food, especially fat and carbohydrate, can blunt the GH pulse. Common timing is morning, midday, and bedtime, spaced at least 4 hours apart, with each injection about 2-3 hours after meals and 30 minutes before eating. This is educational only, not a recommendation.
Q10: Is GHRP-6 legal or FDA-approved?
GHRP-6 has no FDA-approved use and no approved drug product in major regulated markets. It is sold as research-use-only material rather than as a medicine. It is also prohibited in sport by WADA at all times. Confirm current rules before relying on this.
Q11: Is this page medical advice?
No. This is an educational research reference, not medical advice or a treatment plan. Always talk to a qualified clinician before considering any peptide.
Sources & Research
- 1. Bowers CY, Momany FA, Reynolds GA, Hong A On the in vitro and in vivo activity of a new synthetic hexapeptide that acts on the pituitary to specifically release growth hormone. Endocrinology (1984)
- 2. Howard AD, Feighner SD, Cully DF, et al. A receptor in pituitary and hypothalamus that functions in growth hormone release. Science (1996)
- 3. Kojima M, Hosoda H, Date Y, Nakazato M, Matsuo H, Kangawa K Ghrelin is a growth-hormone-releasing acylated peptide from stomach. Nature (1999)
- 4. Arvat E, Maccario M, Di Vito L, et al. Endocrine activities of ghrelin in humans: comparison with GHRP-6 and GHRP-2 (GH, ACTH, cortisol, prolactin). Journal of Clinical Endocrinology & Metabolism (2001)
- 5. Leal-Cerro A, Pereira JL, Garcia-Luna PP, et al. Growth hormone (GH)-releasing peptide-6 requires endogenous hypothalamic GH-releasing hormone for maximal GH stimulation. Journal of Clinical Endocrinology & Metabolism (1998)
- 6. Berlanga-Acosta J, Abreu-Cruz A, Garcia-Ojalvo A, et al. Synthetic growth hormone-releasing peptides (GHRPs): a historical appraisal of the evidences supporting their cytoprotective effects. Clinical Medicine Insights: Cardiology (2017)
- 7. Patchett AA, Nargund RP, Tata JR, et al. Design and biological activities of L-163,191 (MK-0677): a potent, orally active growth hormone secretagogue. Proceedings of the National Academy of Sciences USA (1995)
- 8. Kojima M, Kangawa K Ghrelin: structure and function. Physiological Reviews (2005)
- 9. World Anti-Doping Agency Prohibited List, Section S2: Peptide Hormones, Growth Factors, Related Substances (growth hormone secretagogues). WADA (2026)
- 10. U.S. Food & Drug Administration Bulk Drug Substances Used in Compounding Under Section 503A of the FD&C Act. FDA (2026)
Related Dosing Protocols
Educational use only
This guide is an educational research reference, not medical advice or a treatment plan. GHRP-6 is not FDA-approved and is prohibited in sport by WADA. Talk to a qualified clinician before considering any peptide.
Calculate vial math
Use the calculator for custom vial size, BAC-water volume, and syringe-unit math.
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: Jun 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page