Tesamorelin + Ipamorelin Quick Start
The tesamorelin + ipamorelin blend pairs two compounds that raise growth hormone (GH) through different doors. Tesamorelin is a synthetic GHRH analog: it copies growth hormone-releasing hormone and tells the pituitary gland to make more GH. Ipamorelin is a ghrelin mimetic (a growth hormone secretagogue): it acts on a separate receptor to add to the same GH pulse. For a non-dosing background guide, see Peptide Advisors' tesamorelin + ipamorelin blend overview.
This page is a research-planning reference. It explains how the blend is commonly structured, how to reconstitute each ratio, and what supplies a cycle needs. It does not tell you what to take. Tesamorelin is FDA-approved only for HIV-associated lipodystrophy, ipamorelin is not FDA-approved, and no human trial has tested the two together as a blend.
The supplier blend (Ion Peptides) comes in two ratios in a 3 mL maximum vial: a 10/3 vial (10 mg tesamorelin + 3 mg ipamorelin, 13 mg total) and a 5/5 vial (5 mg tesamorelin + 5 mg ipamorelin, 10 mg total). Choose the ratio first, because it changes the per-unit math.
Reconstitute
Add 3.0 mL BAC water to either vial. 10/3 vial -> ~4.33 mg/mL total; 5/5 vial -> ~3.33 mg/mL total.
Easy measuring
On a U-100 syringe, 10 units = 0.10 mL. 10/3: that draw = ~0.33 mg tes + ~0.10 mg ipa. 5/5: ~0.167 mg tes + ~0.167 mg ipa.
Schedule
Once daily subcutaneous is the common structure; evening dosing is often chosen to track natural nighttime GH release.
Supplies
One 3 mL vial, U-100 insulin syringes, bacteriostatic water, alcohol swabs, sharps bin.
Research status
Educational reference only. Not FDA-approved as a blend. Not medical advice.
Disclaimer
This page is an educational research reference and is not medical advice. Tesamorelin is FDA-approved only for HIV-associated lipodystrophy; ipamorelin is not FDA-approved; the blend is not FDA-approved. No direct human trial has evaluated this combination. Talk to a qualified clinician before making health decisions.
Tesamorelin + Ipamorelin Blend Ratio (10/3 vs 5/5)
Unlike a fixed single-vial product, this blend ships in two ratios. The ratio decides how much of each compound sits in every draw. Pick the ratio before you reconstitute.
Two supplier ratios in a 3 mL vial
Vial
10/3
Tesamorelin
10 mg
Ipamorelin
3 mg
Total peptide
13 mg
Leans toward
GHRH-dominant (more tesamorelin per draw)
Vial
5/5
Tesamorelin
5 mg
Ipamorelin
5 mg
Total peptide
10 mg
Leans toward
Balanced 1:1 GHRH / ghrelin-mimetic
| Vial | Tesamorelin | Ipamorelin | Total peptide | Leans toward |
|---|---|---|---|---|
| 10/3 | 10 mg | 3 mg | 13 mg | GHRH-dominant (more tesamorelin per draw) |
| 5/5 | 5 mg | 5 mg | 10 mg | Balanced 1:1 GHRH / ghrelin-mimetic |
Total peptide drives concentration. The 10/3 vial holds more total peptide, so the same volume delivers more total milligrams.
The 10/3 vial keeps tesamorelin as the lead compound, with a smaller ipamorelin add-on. The 5/5 vial gives equal parts of each, which is the ratio most closely matched by the published 1:1 blend protocols. Neither ratio has been validated in a human blend trial; both are research-planning choices.
Tesamorelin + Ipamorelin Dosing Protocol & Schedule
The most common research-planning structure is a once-daily subcutaneous injection with gradual titration: start low, hold for a week or two, then step up. For reference, the FDA label dose of tesamorelin alone is 2 mg/day (legacy formulation) or 1.28 mg/day for the newer EGRIFTA WR formulation, and ipamorelin has been studied at roughly 100-300 mcg per dose in research settings. This is not a dosing recommendation.
Tesamorelin + Ipamorelin Dosing Guide
Choose the vial format you are using to see the matching instructions.
Use one vial of tesamorelin and one of ipamorelin when you want to adjust each compound on its own.
Separate-vial workflow
Independent dose control
Separate vials let you move tesamorelin and ipamorelin independently. This matters if you want to hold one steady while adjusting the other, or run them on different timing.
Injection burden
1-2 injections/session
Best for
Dose flexibility and timing control
Cycle driver
Compound-specific adjustment
Tesamorelin
- Loading
- 1-2 mg
- Frequency
- Once daily
- Maintenance
- 1-2 mg
- Route
- SubQ
Ipamorelin
- Loading
- 200-300 mcg
- Frequency
- 1-2x daily
- Maintenance
- 200-300 mcg
- Route
- SubQ
Weekly Schedule Example
Monday
Tesamorelin (PM) + Ipamorelin (AM)
Tuesday
Tesamorelin (PM) + Ipamorelin (AM)
Wednesday
Tesamorelin (PM) + Ipamorelin (AM)
Thursday
Tesamorelin (PM) + Ipamorelin (AM)
Friday
Tesamorelin (PM) + Ipamorelin (AM)
Saturday
Optional rest or continue
Sunday
Optional rest or continue
Use separate syringes for separate vials. The figures above are research-context reference ranges, not a dosing recommendation.
One vial holds both compounds at a fixed ratio (10/3 or 5/5). Every draw delivers both at once.
Blend ratio
10 / 3 mg
GHRH-dominant
13 mg total per vial: 10 mg tesamorelin + 3 mg ipamorelin. Reconstituted with 3.0 mL BAC water -> ~4.33 mg/mL total (3.33 mg/mL tesamorelin + 1.0 mg/mL ipamorelin).
Reconstitute
3.0 mL BAC water
Concentration
4.33 mg/mL total blend
10 units draw
0.10 mL = ~0.43 mg total
Typical cycle
8-16 weeks
Dose selector
Component Delivery - 10/3 Vial
| Tesamorelin | 0.33 mg (333 mcg) |
|---|---|
| Ipamorelin | 0.10 mg (100 mcg) |
The 10/3 vial keeps tesamorelin as the lead compound. A 30-unit draw lands near the tesamorelin research reference range while keeping ipamorelin around 300 mcg.
Blend ratio
5 / 5 mg
Balanced 1:1
10 mg total per vial: 5 mg tesamorelin + 5 mg ipamorelin. Reconstituted with 3.0 mL BAC water -> ~3.33 mg/mL total (1.67 mg/mL each).
Reconstitute
3.0 mL BAC water
Concentration
3.33 mg/mL total blend
10 units draw
0.10 mL = ~0.33 mg total
Typical cycle
8-16 weeks
Dose selector
Component Delivery - 5/5 Vial
| Tesamorelin | 0.167 mg (167 mcg) |
|---|---|
| Ipamorelin | 0.167 mg (167 mcg) |
The 5/5 vial delivers equal parts. This is the ratio that most closely matches published 1:1 blend protocols.
Example gradual titration (5/5 vial, once daily SC) - research reference only
Weeks
1-2
Tesamorelin
167 mcg
Ipamorelin
167 mcg
Units (0.10 mL = 10u)
10 units (0.10 mL)
Weeks
3-4
Tesamorelin
333 mcg
Ipamorelin
333 mcg
Units (0.10 mL = 10u)
20 units (0.20 mL)
Weeks
5-8
Tesamorelin
500 mcg
Ipamorelin
500 mcg
Units (0.10 mL = 10u)
30 units (0.30 mL)
Weeks
9-16
Tesamorelin
667 mcg
Ipamorelin
667 mcg
Units (0.10 mL = 10u)
40 units (0.40 mL)
| Weeks | Tesamorelin | Ipamorelin | Units (0.10 mL = 10u) |
|---|---|---|---|
| 1-2 | 167 mcg | 167 mcg | 10 units (0.10 mL) |
| 3-4 | 333 mcg | 333 mcg | 20 units (0.20 mL) |
| 5-8 | 500 mcg | 500 mcg | 30 units (0.30 mL) |
| 9-16 | 667 mcg | 667 mcg | 40 units (0.40 mL) |
Illustrative titration for the 5/5 vial only. This is not a dosing recommendation. Higher draws can be split across two sites for comfort.
Cycle Guidelines
Approach
Standard
Duration
8-12 weeks
Off Period
4-8 weeks
Best For
General research context
Approach
Extended
Duration
12-16 weeks
Off Period
4-8 weeks
Best For
Longer observation windows
| Approach | Duration | Off Period | Best For |
|---|---|---|---|
| Standard | 8-12 weeks | 4-8 weeks | General research context |
| Extended | 12-16 weeks | 4-8 weeks | Longer observation windows |
Time off is commonly used to limit receptor desensitization. This is a planning convention, not a medical instruction.
Evidence boundary
The dosing structure above is assembled from each compound's separate research record and common community protocol planning. No published human trial has tested the tesamorelin + ipamorelin blend as a single product.
Tesamorelin + Ipamorelin Supplies Needed
Planning is based on once-daily dosing from a single 3 mL vial reconstituted with 3.0 mL BAC water. Vial count assumes a typical research draw of 20-40 units/day; a vial lasts roughly 7-15 days depending on draw size, so most cycles use 1 vial every 1-2 weeks.
Recommended USA Supply
Use discount code PEPPAL at eligible peptide supplier checkouts.

Tesamorelin

Ipamorelin

SiPhox Health At-Home Blood Test
Injection Supplies
Companion Supplies & Routine Support
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials (3 mL blend vial)
Assumes ~20-40 units/day; one vial covers about 7-15 days. Round up for priming loss.
| Cycle length | Planning note |
|---|---|
8 weeks 4-6 vials | ~56 daily doses. |
12 weeks 6-9 vials | ~84 daily doses. |
16 weeks 8-12 vials | ~112 daily doses. |
8 weeks
4-6 vials
~56 daily doses.
12 weeks
6-9 vials
~84 daily doses.
16 weeks
8-12 vials
~112 daily doses.
Insulin Syringes (U-100)
Prefer 0.5 mL / 50-unit syringes to fit larger blend draws.
| Cycle length | Planning note |
|---|---|
8 weeks 56 syringes | 1 per day |
12 weeks 84 syringes | 1 per day |
16 weeks 112 syringes | 1 per day |
8 weeks
56 syringes
1 per day
12 weeks
84 syringes
1 per day
16 weeks
112 syringes
1 per day
Bacteriostatic Water
Use 3.0 mL per vial for reconstitution.
| Cycle length | Planning note |
|---|---|
8 weeks 2 x 10 mL bottles | 4-6 vials use 12-18 mL. |
12 weeks 2-3 x 10 mL bottles | 6-9 vials use 18-27 mL. |
16 weeks 3-4 x 10 mL bottles | 8-12 vials use 24-36 mL. |
8 weeks
2 x 10 mL bottles
4-6 vials use 12-18 mL.
12 weeks
2-3 x 10 mL bottles
6-9 vials use 18-27 mL.
16 weeks
3-4 x 10 mL bottles
8-12 vials use 24-36 mL.
Round up for priming losses, dropped syringes, damaged swabs, and protocol adjustments. Vial counts shift with draw size; recalculate if your daily units differ.
Tesamorelin + Ipamorelin Reconstitution Guide
Reconstitution by Vial Format
Choose your vial format for the matching math.
Independent vials of each compound.
Reconstitute each vial on its own. A common approach is 2-3 mL BAC water per 10 mg vial. For exact concentration and unit math on a single compound, use the dedicated Ipamorelin protocol and a tesamorelin vial's own label, plus the calculator.
Single vial holding both compounds.
Reconstitution math (3.0 mL BAC water, 3 mL vial)
Vial
10/3
Total mg
13 mg
Concentration
4.33 mg/mL total
10 units (0.10 mL) delivers
0.33 mg tes + 0.10 mg ipa
Vial
5/5
Total mg
10 mg
Concentration
3.33 mg/mL total
10 units (0.10 mL) delivers
0.167 mg tes + 0.167 mg ipa
| Vial | Total mg | Concentration | 10 units (0.10 mL) delivers |
|---|---|---|---|
| 10/3 | 13 mg | 4.33 mg/mL total | 0.33 mg tes + 0.10 mg ipa |
| 5/5 | 10 mg | 3.33 mg/mL total | 0.167 mg tes + 0.167 mg ipa |
3.0 mL is the practical maximum for this 3 mL vial. Smaller volumes raise concentration and shrink the draw, but reduce measuring precision at very low units.
- 01
Sanitize
Wipe the vial stopper and your hands; use a fresh syringe.
- 02
Draw BAC water
Pull 3.0 mL bacteriostatic water into a reconstitution syringe.
- 03
Add slowly
Aim the stream down the inside vial wall; do not blast the powder.
- 04
Swirl, don't shake
Gently roll until fully dissolved; shaking can damage peptide.
- 05
Inspect
Solution should be clear. Discard if cloudy or full of particles.
- 06
Label
Write the ratio, date, and concentration on the vial.
- 07
Store
Refrigerate 2-8 C (35.6-46.4 F), protected from light.
Calculator
Use the PepPal calculator to recompute concentration and unit math for any vial size, ratio, or BAC-water volume.
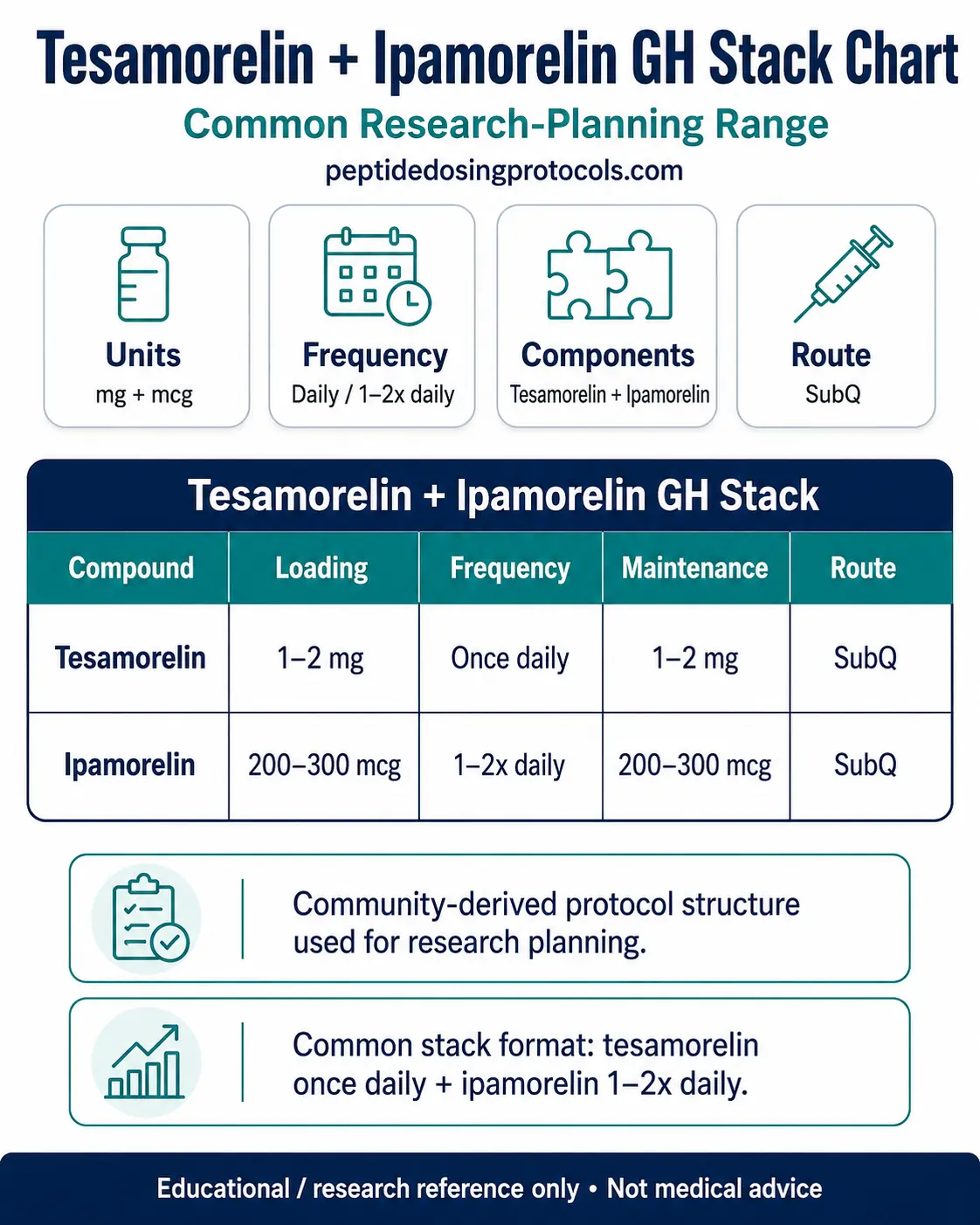
Tesamorelin + Ipamorelin Dosage Chart
This tesamorelin + ipamorelin dosage chart summarizes the common separate-vial research-planning range, with compound units, frequency, maintenance range, and route shown together.
Why the Blend Combines Tesamorelin and Ipamorelin
The two compounds hit growth hormone release through different receptors. Tesamorelin copies GHRH and binds GHRH receptors on the pituitary. Ipamorelin copies ghrelin and binds the GHS-R1a (ghrelin) receptor on the same gland.
Pairing a GHRH analog with a ghrelin-mimetic GH secretagogue is a long-standing idea in GH research. Combined GHRH + GHRP/ghrelin-mimetic administration has produced larger, amplified GH pulses than either agent alone in human secretagogue studies. The blend applies that same two-pathway logic.
- Tesamorelin: GHRH-receptor pathway, the FDA-studied driver of visceral fat reduction.
- Ipamorelin: GHS-R1a (ghrelin) pathway, selective for GH with little effect on cortisol or prolactin in animal studies.
- Main limitation: synergy is shown for GHRH + secretagogue classes in general, not for this exact blend in a human trial.
Tesamorelin + Ipamorelin Side Effects & Safety
Compound-level safety
From tesamorelin trials, the most commonly reported adverse events include injection-site reactions (redness, itching), joint pain (arthralgia), pain in the extremities, peripheral edema (fluid retention), and muscle aches. Tesamorelin has also been linked to glucose intolerance and a higher risk of type 2 diabetes, and is contraindicated in pregnancy.
Ipamorelin is generally well tolerated in animal studies and the limited human data; transient flushing or headache may occur. Because ipamorelin has not completed human trials, its long-term safety is not established.
Stack-specific unknowns
- Combined GH elevation could raise the chance of GH-related effects like water retention, joint discomfort, or numbness/tingling if pushed high.
- Blood sugar: GH lowers insulin sensitivity, so anyone with glucose issues should be especially cautious.
- No human trial has characterized the side-effect profile of the blend specifically.
Injection-site and quality risks
- Rotate sites (abdomen, thigh, upper arm) to avoid lumps (lipohypertrophy).
- Grey-market quality varies; verify a current COA for the exact batch before use.
Regulatory status
As of June 2026, tesamorelin is FDA-approved only for HIV-associated lipodystrophy (EGRIFTA WR / EGRIFTA SV); ipamorelin is not FDA-approved; the blend is not FDA-approved. Sold for research use only.
Tesamorelin + Ipamorelin Clinical Evidence Context
Direct stack evidence: none. No published human trial has tested the tesamorelin + ipamorelin blend as a single product. Everything below is compound-level evidence, presented so you can see what is and is not established.
Tesamorelin evidence
Tesamorelin is the stronger evidence anchor in this blend. It has randomized Phase 3 human data in adults with HIV-associated lipodystrophy, where daily tesamorelin reduced visceral abdominal fat. That is why tesamorelin carries FDA approval as EGRIFTA, EGRIFTA SV, and EGRIFTA WR for that specific use.
Ipamorelin evidence
Ipamorelin has a narrower evidence base. Early pharmacology work described it as a selective growth-hormone secretagogue, with GH release and little ACTH or cortisol signal in the foundational studies. Human clinical development was limited, and the postoperative ileus trial program did not establish an approved use.
Why the pairing is plausible
The logic for combining them comes from pathway biology: tesamorelin works through the GHRH receptor, while ipamorelin works through the ghrelin/GHS-R1a receptor. Those two signals can feed the same GH pulse from different angles. That supports the research rationale, but it still does not prove this specific pre-blended product is effective or safe in humans.
Tesamorelin + Ipamorelin Storage & Handling
Storage quick reference
Lyophilized (Powder Form)
Tesamorelin + Ipamorelin Blend
-4F (-20C) long-term; 2-8C (35.6-46.4F) short-term
Reconstituted (Liquid Form)
Tesamorelin + Ipamorelin Blend
35.6-46.4F (2-8C), protected from light
Appearance
Tesamorelin + Ipamorelin Blend
Clear after reconstitution
| Tesamorelin + Ipamorelin Blend | |
|---|---|
| Lyophilized (Powder Form) | -4F (-20C) long-term; 2-8C (35.6-46.4F) short-term |
| Reconstituted (Liquid Form) | 35.6-46.4F (2-8C), protected from light |
| Appearance | Clear after reconstitution |
Do not freeze reconstituted solution. Let vials reach room temperature before opening to limit condensation.
Reconstituted peptide is best used within a few weeks when refrigerated; discard sooner if the solution turns cloudy or shows particles. Keep a fresh, batch-matched COA on hand.
Tesamorelin + Ipamorelin vs Sermorelin and CJC-1295 Blends
How the blend compares to nearby GH options
Option
Tesamorelin + Ipamorelin
GHRH side
Tesamorelin (FDA-studied)
Secretagogue side
Ipamorelin
Note
Strongest GHRH evidence of the GHRH options here.
Option
Sermorelin + Ipamorelin
GHRH side
Sermorelin (shorter-acting)
Secretagogue side
Ipamorelin
Note
Sermorelin is a classic GHRH but less potent/stable than tesamorelin.
Option
CJC-1295 + Ipamorelin
GHRH side
CJC-1295 (longer-acting GHRH)
Secretagogue side
Ipamorelin
Note
CJC-1295 extends GHRH signaling; common alternative pairing.
| Option | GHRH side | Secretagogue side | Note |
|---|---|---|---|
| Tesamorelin + Ipamorelin | Tesamorelin (FDA-studied) | Ipamorelin | Strongest GHRH evidence of the GHRH options here. |
| Sermorelin + Ipamorelin | Sermorelin (shorter-acting) | Ipamorelin | Sermorelin is a classic GHRH but less potent/stable than tesamorelin. |
| CJC-1295 + Ipamorelin | CJC-1295 (longer-acting GHRH) | Ipamorelin | CJC-1295 extends GHRH signaling; common alternative pairing. |
These are not interchangeable. For the CJC-1295 pairing, see the dedicated stack page rather than substituting here.
Several CSV queries ask about adding CJC-1295 to make a triple blend. That is a different protocol; see the CJC-1295 + Ipamorelin stack rather than treating it as a variant here.
FAQ
Q1: What is the tesamorelin and ipamorelin blend?
It is a combination of two growth hormone compounds. Tesamorelin is a GHRH analog and ipamorelin is a ghrelin-mimetic GH secretagogue. Together they target two different receptors that feed the same growth hormone pulse. The blend is sold for research use only and is not FDA-approved as a combination product.
Q2: What is the tesamorelin ipamorelin blend dosage per day?
Common research-planning structures use one subcutaneous dose per day with gradual titration. For reference, tesamorelin's FDA label dose alone is 2 mg/day (or 1.28 mg/day for the EGRIFTA WR formulation), and ipamorelin has been studied around 100-300 mcg per dose. This is not a dosing recommendation. Use the calculator for your exact vial.
Q3: What is the difference between the 10/3 and 5/5 blend?
The 10/3 vial holds 10 mg tesamorelin and 3 mg ipamorelin (13 mg total), so it is GHRH-dominant. The 5/5 vial holds 5 mg of each (10 mg total) for a balanced 1:1 ratio. The ratio changes how much of each compound is in every draw, so reconstitute and measure with your specific ratio in mind.
Q4: How do you reconstitute the tesamorelin ipamorelin blend?
Add 3.0 mL bacteriostatic water to the 3 mL vial, aiming down the wall, then swirl gently until clear. A 10/3 vial becomes about 4.33 mg/mL total; a 5/5 vial becomes about 3.33 mg/mL total. See the reconstitution guide above for the per-unit math.
Q5: Can you take tesamorelin and ipamorelin together?
They are commonly combined in research planning because they act on two different GH pathways, and GHRH-plus-secretagogue pairings have amplified GH pulses in human secretagogue studies. However, no human trial has tested this specific blend, so the combined safety and effect profile is not established. This is educational information, not medical advice.
Q6: When is the blend usually taken?
Once-daily evening or bedtime dosing is the most common structure, chosen to track the body's natural nighttime GH release. Some separate-vial users place ipamorelin earlier in the day. Timing is a planning convention here, not a medical instruction.
Q7: How long is a typical cycle?
Research-planning cycles commonly run 8-16 weeks followed by 4-8 weeks off, a convention used to limit receptor desensitization. There is no established cycle length for the blend specifically.
Q8: Where do you inject it?
Both compounds are injected subcutaneously, just under the skin. Common sites are the abdomen, thigh, and upper arm. Rotate sites each day to reduce irritation and lumps. See the supplies and reconstitution sections above for technique basics.
Q9: What are the main side effects?
From tesamorelin trials: injection-site reactions, joint pain, fluid retention, muscle aches, and possible glucose intolerance. Ipamorelin is generally well tolerated in limited data, with occasional flushing or headache. The blend's combined profile has not been studied in humans.
Q10: Is the tesamorelin ipamorelin blend FDA-approved?
No. As of June 2026, tesamorelin is FDA-approved only for HIV-associated lipodystrophy (sold as EGRIFTA WR and EGRIFTA SV), ipamorelin is not FDA-approved, and the blend is not FDA-approved. It is sold for research use only.
Q11: Is this page medical advice?
No. This is an educational research reference covering dosing structure, reconstitution math, supplies, and safety context. It is not medical advice or a treatment plan. Talk to a qualified clinician before making health decisions.
Sources & Research
- 1. Falutz J, et al. Tesamorelin, a growth hormone-releasing factor analog, in HIV patients with abdominal fat accumulation (Phase 3). JAMA / New England Journal of Medicine (2010)
- 2. Theratechnologies Inc. FDA approval of EGRIFTA WR (tesamorelin F8) for excess visceral abdominal fat in adults with HIV and lipodystrophy. Theratechnologies / GlobeNewswire (FDA action) (2025)
- 3. U.S. Food and Drug Administration EGRIFTA (tesamorelin for injection) prescribing information / label. FDA Drugs@FDA (2010)
- 4. LiverTox (NIDDK) Tesamorelin: synthetic GHRH analog; 2 mg SC daily for HIV lipodystrophy. NCBI Bookshelf (LiverTox) (2018)
- 5. Spooner LM, Olin JL. Tesamorelin: a growth hormone-releasing factor analogue for HIV-associated lipodystrophy. Annals of Pharmacotherapy (2012)
- 6. Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology (1998)
- 7. Beck DE, Sweeney WB, McCarter MD, et al. Proof-of-concept study of the ghrelin mimetic ipamorelin for postoperative ileus (Phase 2, discontinued). International Journal of Colorectal Disease (2014)
- 8. Sinha DK, et al. The safety and efficacy of growth hormone secretagogues; GHRH + GHRP synergy and dual-pathway GH stimulation. PMC (PMC5632578) (2017)
- 9. Johansen PB, Nowak J, Skjaerbaek C, et al. Ipamorelin induces longitudinal bone growth in rats. Growth Hormone & IGF Research (1999)
- 10. Friedman SD, Baker LD, Borson S, et al. GHRH (tesamorelin) effects on brain GABA in mild cognitive impairment and healthy aging. JAMA Neurology (2013)
- 11. Dhillon S. Tesamorelin: a review of its use in HIV-associated lipodystrophy. Drugs (2011)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page