IGF-1 LR3 Quick Start
IGF-1 LR3 is a synthetic, longer-acting analog of insulin-like growth factor 1 (IGF-1). The body's own IGF-1 carries growth signals from the liver to muscle, bone, and other tissues. IGF-1 LR3 is engineered to do the same thing, but for a much longer period of time and without being captured by the proteins that normally limit IGF-1 activity.
Two structural changes drive the difference. The peptide has an arginine in place of glutamic acid at position 3, and an extra 13-amino-acid extension on the front (the N-terminus), making the full chain 83 amino acids instead of native IGF-1's 70. These modifications cut its affinity for IGF binding proteins and stretch the half-life to roughly 20-30 hours.
There is no oral or topical version of IGF-1 LR3 in research use. The only practical research format is a lyophilized (freeze-dried) powder reconstituted with bacteriostatic water and injected subcutaneously or intramuscularly. This page treats injection as the only route.
Route
Subcutaneous (SubQ) or intramuscular (IM) injection only. No validated oral or topical form.
Schedule
Once daily in research planning, due to the 20-30 hour half-life.
Dose context
20-100 mcg/day appears across community protocols. No human clinical trial has validated a dosing range for IGF-1 LR3.
Measuring
Insulin syringe (U-100). Concentration depends on vial size and BAC water volume.
Cycle structure
Most protocols cap on-time at 4-6 weeks with at least equal off-time before any subsequent cycle.
Status
Not FDA-approved for any human use. Banned at all times by WADA. Sold as a research reagent only.
Disclaimer
This page is an educational research reference and is not medical advice. IGF-1 LR3 is a research compound, not a medication. The hypoglycemia risk discussed below is real — preclinical and Increlex (mecasermin) human data both demonstrate it. Talk to a qualified clinician before considering use.
IGF-1 LR3 Dosing Protocol & Schedule
IGF-1 LR3 dosing is reported in micrograms (mcg), not milligrams. Doses are small, so syringe accuracy matters. Community protocols generally cluster between 20 and 100 mcg per day, given as one daily injection because of the long half-life. None of these ranges come from a published human clinical trial of IGF-1 LR3 — they are extrapolated from preclinical work, the Increlex (mecasermin) clinical record, and decades of community reporting.
Important evidence boundary
No formal human clinical trial has ever evaluated IGF-1 LR3 for any therapeutic or performance endpoint. Dose ranges below describe what appears in research-community protocols, not validated clinical dosing.
IGF-1 LR3 Protocol Formats
IGF-1 LR3 is only used as an injection. The two relevant routes are subcutaneous and intramuscular. Each tab walks through how the route is typically structured in research protocols.
The simpler and more commonly used research route. Distributes systemically.
Subcutaneous injection deposits IGF-1 LR3 into the fatty layer just under the skin (commonly the abdomen, around 2-3 inches from the navel, or the upper thigh). The peptide is absorbed gradually and circulates systemically. Because the half-life is 20-30 hours, one injection per day produces relatively stable receptor coverage.
Common IGF-1 LR3 SubQ dose context (research planning, not clinical guidance)
Phase
Assessment
Daily dose
20 mcg/day
Frequency
Once daily
Notes
Used to gauge tolerance and hypoglycemic response.
Phase
Low range
Daily dose
20-40 mcg/day
Frequency
Once daily
Notes
Most-cited beginner range. Women in community sources often stay 10-20 mcg/day.
Phase
Moderate range
Daily dose
40-80 mcg/day
Frequency
Once daily
Notes
Diminishing returns commonly reported above ~50-60 mcg/day.
Phase
High range
Daily dose
80-100 mcg/day
Frequency
Once daily
Notes
Reported by advanced users; side-effect frequency rises.
| Phase | Daily dose | Frequency | Notes |
|---|---|---|---|
| Assessment | 20 mcg/day | Once daily | Used to gauge tolerance and hypoglycemic response. |
| Low range | 20-40 mcg/day | Once daily | Most-cited beginner range. Women in community sources often stay 10-20 mcg/day. |
| Moderate range | 40-80 mcg/day | Once daily | Diminishing returns commonly reported above ~50-60 mcg/day. |
| High range | 80-100 mcg/day | Once daily | Reported by advanced users; side-effect frequency rises. |
These ranges are observational. They are not human clinical dosing guidance.
Most reported timing is post-workout on training days, which lines up the injection with elevated blood glucose and a planned meal — both of which reduce hypoglycemia risk. On rest days, morning with food is the common timing. Almost all sources advise against pre-bed dosing because hypoglycemia during sleep is harder to detect.
Often used for site-specific research interest. Still produces systemic effects.
Intramuscular injection delivers IGF-1 LR3 directly into a muscle belly (commonly the deltoid, vastus lateralis, or gluteus). Some research-community sources argue this creates a higher local concentration in the injected muscle. The 20-30 hour half-life means the peptide still distributes systemically regardless of site, so any local-only effect is partial at best.
Common IGF-1 LR3 IM dose context (research planning, not clinical guidance)
Phase
Assessment
Daily dose
20 mcg/day
Site
Trained muscle, post-workout
Notes
Identical glucose-monitoring rules apply as with SubQ.
Phase
Low-moderate
Daily dose
20-50 mcg/day
Site
Trained muscle, post-workout
Notes
Often used in research interest in localized hypertrophy signaling.
Phase
Moderate-high
Daily dose
50-100 mcg/day
Site
Trained muscle, post-workout
Notes
Side-effect frequency rises in the upper portion of the range.
| Phase | Daily dose | Site | Notes |
|---|---|---|---|
| Assessment | 20 mcg/day | Trained muscle, post-workout | Identical glucose-monitoring rules apply as with SubQ. |
| Low-moderate | 20-50 mcg/day | Trained muscle, post-workout | Often used in research interest in localized hypertrophy signaling. |
| Moderate-high | 50-100 mcg/day | Trained muscle, post-workout | Side-effect frequency rises in the upper portion of the range. |
Use a 25-27 gauge, ~1-inch needle for IM. Same hypoglycemia rules apply: never fasted, never pre-bed.
IM injections require more technique than SubQ and carry slightly more risk of nerve or blood-vessel contact at certain sites. Many research protocols default to SubQ for simplicity and reserve IM for specific site-based research questions.
Cycle structure
IGF-1 LR3 Cycle Structure
Approach
Conservative
On-cycle
3-4 weeks
Off-cycle
4-6 weeks
Best for
Lower-dose tolerance assessment in first cycles.
Approach
Standard
On-cycle
4 weeks
Off-cycle
4 weeks minimum
Best for
Most-cited research-community structure.
Approach
Extended
On-cycle
5-6 weeks
Off-cycle
6 weeks minimum
Best for
Used only after prior cycles confirmed glucose tolerance.
| Approach | On-cycle | Off-cycle | Best for |
|---|---|---|---|
| Conservative | 3-4 weeks | 4-6 weeks | Lower-dose tolerance assessment in first cycles. |
| Standard | 4 weeks | 4 weeks minimum | Most-cited research-community structure. |
| Extended | 5-6 weeks | 6 weeks minimum | Used only after prior cycles confirmed glucose tolerance. |
Continuous, multi-month use is widely discouraged because of progressive insulin resistance, organ-growth concerns, and IGF-1 receptor desensitization. The 6-week ceiling reflects observed risk patterns, not a clinical guideline.
Timing rules across both routes. Eat 30-50 grams of fast-acting carbohydrates within roughly 30 minutes of every injection. Never inject in a fasted state. Never inject within 2 hours of bedtime — overnight hypoglycemia is the highest-risk scenario. Skip a missed dose and resume on schedule the next day. Never double-dose to compensate.
IGF-1 LR3 Supplies Needed
Supply planning below is matched to a once-daily SubQ schedule with a 1 mg vial reconstituted in 2 mL of bacteriostatic water (500 mcg/mL). Adjust if you choose a different concentration.
Recommended USA Supply
Use discount code SAVE10 at Peptira checkout. See why we love Peptira.
IGF-1 LR3 Supply

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials
Most common research vial sizes are 1 mg (1,000 mcg) and 0.1 mg (100 mcg). Math below assumes a 1 mg vial reconstituted with 2 mL of BAC water at a typical 40 mcg/day dose (25 days per vial).
| Cycle length | Planning note |
|---|---|
4-5 weeks 2 vials | 4 weeks: 28 daily doses; second vial covers margin and fresh reconstitution.; 5 weeks: 35 daily doses; comfortable within 2 vials at 40 mcg/day. |
6 weeks 3 vials | 42 daily doses; reconstitute fresh vial as each is exhausted. |
4-5 weeks
2 vials
4 weeks: 28 daily doses; second vial covers margin and fresh reconstitution.; 5 weeks: 35 daily doses; comfortable within 2 vials at 40 mcg/day.
6 weeks
3 vials
42 daily doses; reconstitute fresh vial as each is exhausted.
Insulin Syringes (U-100)
0.3 mL or 0.5 mL U-100 insulin syringes are best because typical draw volumes are 0.04-0.20 mL. Use a fresh syringe for every injection.
| Cycle length | Planning note |
|---|---|
4 weeks 28 syringes | 1 syringe per daily injection. |
5 weeks 35 syringes | 1 syringe per daily injection. |
6 weeks 42 syringes | 1 syringe per daily injection. |
4 weeks
28 syringes
1 syringe per daily injection.
5 weeks
35 syringes
1 syringe per daily injection.
6 weeks
42 syringes
1 syringe per daily injection.
Bacteriostatic Water
Each 1 mg vial uses ~2 mL of BAC water at the 500 mcg/mL setup. 10 mL bottles are standard.
| Cycle length | Planning note |
|---|---|
4-6 weeks 1 x 10 mL bottle | 4 weeks: 2 vials use ~4 mL total; one bottle gives margin.; 5 weeks: Same as above; still under 5 mL used.; 6 weeks: 3 vials use ~6 mL total; one bottle is sufficient. |
4-6 weeks
1 x 10 mL bottle
4 weeks: 2 vials use ~4 mL total; one bottle gives margin.; 5 weeks: Same as above; still under 5 mL used.; 6 weeks: 3 vials use ~6 mL total; one bottle is sufficient.
Glucose source
A fast-acting carbohydrate source on hand is essential because of the hypoglycemia risk. Glucose tablets, fruit juice, or a planned post-injection meal all work.
| Cycle length | Planning note |
|---|---|
Per cycle Daily access | Available within 30 minutes of every injection without exception. |
Per cycle
Daily access
Available within 30 minutes of every injection without exception.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments. Concentration changes (1 mL or 3 mL BAC water instead of 2 mL) will change the per-dose draw volume but not the swab or syringe count.
Companion Supplies & Routine Support
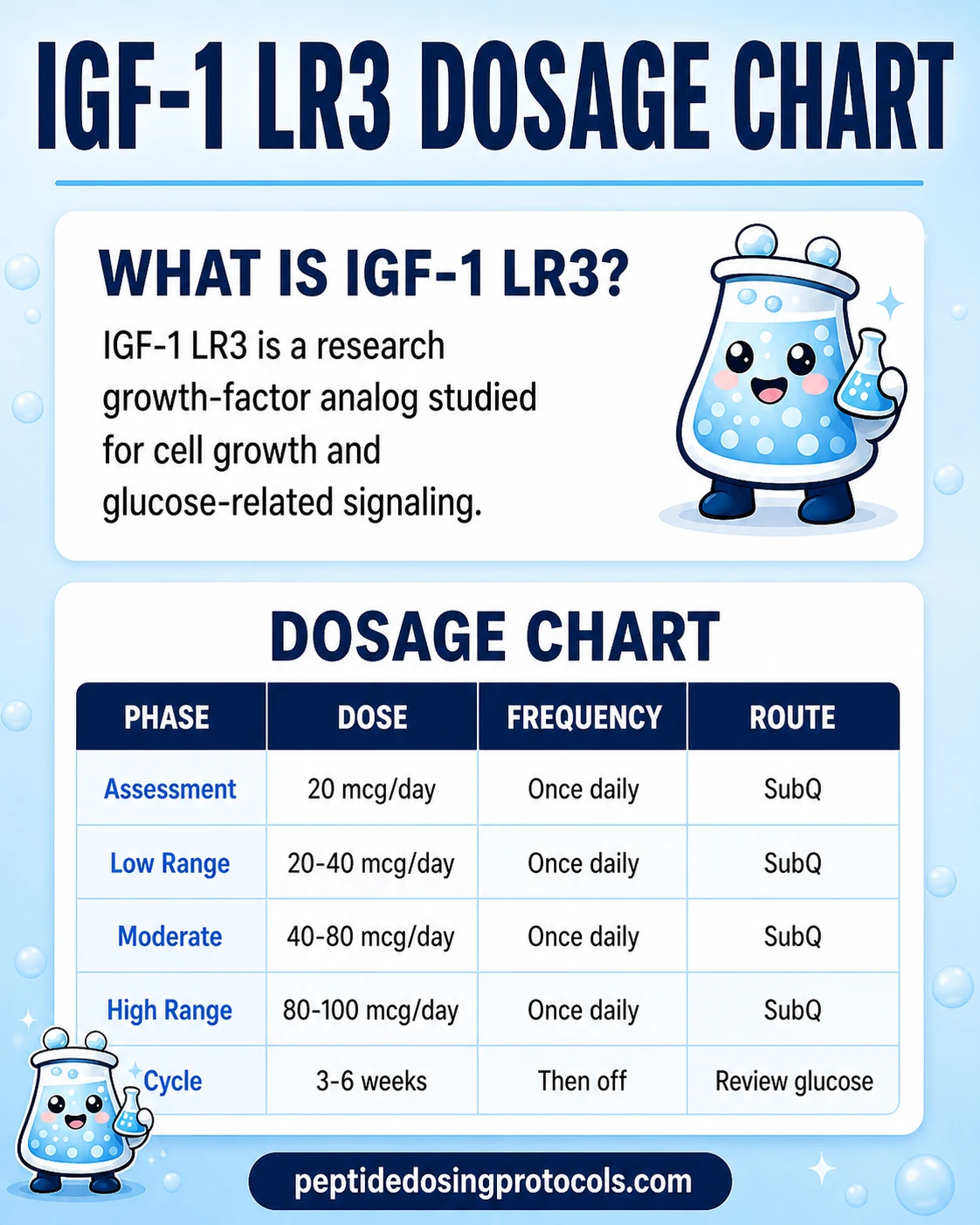
IGF-1 LR3 Dosage Chart
This IGF-1 LR3 dosage chart summarizes the SubQ research-planning ranges from 20 mcg to 100 mcg daily shown in the dosing section above.
IGF-1 LR3 Reconstitution Guide
IGF-1 LR3 ships as a freeze-dried powder. Before use it has to be dissolved in bacteriostatic water (BAC water) — water with 0.9% benzyl alcohol that prevents microbial growth. Plain saline or sterile water are not appropriate substitutes for multi-dose vials.
IGF-1 LR3 Reconstitution Reference (1 mg / 1,000 mcg vial)
BAC water added
1 mL
Concentration
1,000 mcg/mL
20 mcg dose
0.02 mL (2 units)
40 mcg dose
0.04 mL (4 units)
50 mcg dose
0.05 mL (5 units)
80 mcg dose
0.08 mL (8 units)
100 mcg dose
0.10 mL (10 units)
BAC water added
2 mL
Concentration
500 mcg/mL
20 mcg dose
0.04 mL (4 units)
40 mcg dose
0.08 mL (8 units)
50 mcg dose
0.10 mL (10 units)
80 mcg dose
0.16 mL (16 units)
100 mcg dose
0.20 mL (20 units)
BAC water added
3 mL
Concentration
333 mcg/mL
20 mcg dose
0.06 mL (6 units)
40 mcg dose
0.12 mL (12 units)
50 mcg dose
0.15 mL (15 units)
80 mcg dose
0.24 mL (24 units)
100 mcg dose
0.30 mL (30 units)
| BAC water added | Concentration | 20 mcg dose | 40 mcg dose | 50 mcg dose | 80 mcg dose | 100 mcg dose |
|---|---|---|---|---|---|---|
| 1 mL | 1,000 mcg/mL | 0.02 mL (2 units) | 0.04 mL (4 units) | 0.05 mL (5 units) | 0.08 mL (8 units) | 0.10 mL (10 units) |
| 2 mL | 500 mcg/mL | 0.04 mL (4 units) | 0.08 mL (8 units) | 0.10 mL (10 units) | 0.16 mL (16 units) | 0.20 mL (20 units) |
| 3 mL | 333 mcg/mL | 0.06 mL (6 units) | 0.12 mL (12 units) | 0.15 mL (15 units) | 0.24 mL (24 units) | 0.30 mL (30 units) |
Units refer to U-100 insulin syringe markings. 100 units = 1 mL. Many users find 2 mL of BAC water the most practical balance between draw accuracy and concentration. 0.1 mg (100 mcg) vials are also sold; the same math principles apply at 1/10 the scale.
IGF-1 LR3 Reconstitution Reference (0.1 mg / 100 mcg vial)
BAC water added
0.5 mL
Concentration
200 mcg/mL
20 mcg dose
0.10 mL (10 units)
40 mcg dose
0.20 mL (20 units)
50 mcg dose
0.25 mL (25 units)
BAC water added
1 mL
Concentration
100 mcg/mL
20 mcg dose
0.20 mL (20 units)
40 mcg dose
0.40 mL (40 units)
50 mcg dose
0.50 mL (50 units)
| BAC water added | Concentration | 20 mcg dose | 40 mcg dose | 50 mcg dose |
|---|---|---|---|---|
| 0.5 mL | 200 mcg/mL | 0.10 mL (10 units) | 0.20 mL (20 units) | 0.25 mL (25 units) |
| 1 mL | 100 mcg/mL | 0.20 mL (20 units) | 0.40 mL (40 units) | 0.50 mL (50 units) |
Smaller vials are typically used for short cycles or first-cycle assessment. Doses above 50 mcg become impractical from a 0.1 mg vial — switch to a 1 mg vial.
- 01
Wash and prepare
Wash hands thoroughly. Lay out a clean surface with the IGF-1 LR3 vial, BAC water, alcohol swabs, and a sterile syringe.
- 02
Swab both stoppers
Wipe the rubber stoppers of the IGF-1 LR3 vial and the BAC water vial with separate alcohol swabs. Let them air-dry for 10-15 seconds.
- 03
Draw bacteriostatic water
Pull the planned volume of BAC water (commonly 1-2 mL for a 1 mg vial) into a sterile mixing syringe.
- 04
Inject down the side wall
Slowly inject the BAC water against the inner wall of the IGF-1 LR3 vial — never directly onto the lyophilized powder cake.
- 05
Swirl, never shake
Gently swirl or roll the vial between your palms until the powder fully dissolves. Shaking introduces foam and can damage the peptide structure.
- 06
Inspect
The solution should be clear and free of particles before any draw. If cloudy or with visible debris, do not use.
- 07
Refrigerate
Store at 2-8°C (36-46°F). Use within roughly 28-30 days. Do not freeze the reconstituted solution.
Calculator
For exact draw volumes at custom vial sizes or BAC water amounts, use the Pep Pal reconstitution calculator.
How IGF-1 LR3 Works
IGF-1 LR3 binds to the IGF-1 receptor (IGF-1R), a tyrosine kinase receptor present on most tissues — skeletal muscle, bone, liver, kidney, nerve, and connective tissue. When the receptor is engaged, it kicks off intracellular signaling cascades that drive both protein-building activity and cell proliferation.
Two main downstream pathways
PI3K → Akt → mTOR. This is the protein-synthesis arm. It increases muscle protein synthesis, reduces protein breakdown, supports glucose and amino acid uptake, and suppresses programmed cell death. It is also the pathway that drives IGF-1 LR3's insulin-like glucose-lowering effect — the same mechanism that creates hypoglycemia risk.
RAS → RAF → MEK → ERK (MAPK). This is the proliferation arm. It supports cell division and tissue growth. In skeletal muscle this pathway can support satellite cell activation and possible hyperplasia (creation of new muscle fibers). The same mitogenic activity is the basis of long-term cancer concern, because IGF-1 signaling is one of the more well-documented growth pathways studied in tumor biology.
Why IGF-1 LR3 is more potent than native IGF-1
Native IGF-1 is largely sequestered in circulation by IGF binding proteins (IGFBPs) — a family of six proteins that escort IGF-1 around the body and limit how much is free to engage receptors. The structural changes in IGF-1 LR3 (the arginine substitution and 13-amino-acid extension) drop binding-protein affinity sharply. More peptide stays free, and the half-life stretches from roughly 12-15 hours for native IGF-1 to about 20-30 hours for IGF-1 LR3. Tomas et al. (1996) reported the analog was 1.5-2x more potent than equimolar IGF-1 in catabolic rat models, and broader pharmacology literature places it at roughly 3x potency overall.
These same pharmacology properties — direct receptor activation, reduced binding-protein clearance, and the long half-life — explain both the anabolic interest researchers have in IGF-1 LR3 and its primary safety liabilities.
Who IGF-1 LR3 Is For and Who Should Avoid It
IGF-1 LR3 has no FDA-approved human indication. It is studied as a research compound and used in research-community protocols only. The Increlex (mecasermin) FDA label, which covers native rhIGF-1 in pediatric severe primary IGFD, is the closest human reference and informs the contraindications below.
Settings where IGF-1 LR3 is widely contraindicated
Active or prior cancer, or strong family history of cancer. IGF-1 signaling is mitogenic and anti-apoptotic. The Increlex label explicitly contraindicates use in patients with active or suspected neoplasia and notes that active or suspected malignancy should prompt discontinuation. Epidemiological studies have repeatedly linked elevated circulating IGF-1 to risk of certain cancers (LeRoith & Roberts 2003; Pollak 2008).
Diabetes (type 1 or type 2) or any condition involving glucose dysregulation. IGF-1 LR3 lowers blood glucose. Adding it to existing insulin therapy or impaired glucose handling can produce unpredictable, severe hypoglycemia. The 2025 Increlex label requires meal/snack pairing and dose titration starting from a low dose specifically because hypoglycemia is so consistent.
Pregnancy and breastfeeding. No human safety data exists. The Increlex label specifies it should not be used by pregnant women.
Closed or near-closed epiphyses being a goal of approved use. Mecasermin loses approved indication once growth plates close. For IGF-1 LR3, that means there is no validated 'normal-adult' indication at all. Adolescents with open growth plates are not appropriate research subjects in unsupervised settings due to disproportionate-growth concerns.
Concurrent insulin or insulin secretagogue therapy. Combining IGF-1 LR3 with insulin or sulfonylureas produces additive hypoglycemia. Multiple research-community sources flag this combination as having been associated with hospitalizations. There is no protocol justification for combining the two outside direct clinician supervision.
Pre-existing cardiac, kidney, liver, or splenic conditions. IGF-1 supports growth in many organ systems. Increlex labeling notes rapid increases in renal and splenic length in some treated patients. Pre-existing organ disease is widely treated as a hard contraindication.
Competitive athletes in tested sports. IGF-1 LR3 is prohibited at all times by the World Anti-Doping Agency (WADA) and by all major professional sports organizations. Detection assays for LR3 have been published in peer-reviewed analytical literature (Mongongu et al. 2020).
IGF-1 LR3 Side Effects & Safety
There are no published human clinical trials of IGF-1 LR3 itself. The closest safety dataset is the Increlex (mecasermin) clinical program, which followed 71 pediatric patients with severe primary IGFD on twice-daily SubQ rhIGF-1 for a mean of 3.9 years (some patients up to 11.5 years). The figures below are from the FDA-approved Increlex labeling.
Hypoglycemia (the primary acute risk)
In the Increlex program, hypoglycemia was reported in 30 of 71 subjects (42%). Most events were mild or moderate. Five subjects had severe hypoglycemia requiring assistance, and four experienced hypoglycemic seizures or loss of consciousness on at least one occasion. The rate was highest in the first month of treatment. Symptoms include shakiness, sweating, hunger, anxiety, confusion, dizziness, blurred vision, and at the severe end, seizure or loss of consciousness.
Mitigation in the Increlex label is straightforward: administer with food, never on an empty stomach, monitor glucose during titration, and keep fast-acting carbohydrates available. The IGF-1 LR3 research community uses the same rule set, with the additional precaution of avoiding pre-bed dosing because of overnight hypoglycemia risk.
Tonsillar and lymphoid hypertrophy
Tonsillar hypertrophy was reported in roughly 15% of Increlex subjects. Adenoidal hypertrophy and snoring/sleep apnea were also documented. The mechanism is consistent with general lymphoid tissue growth under elevated IGF-1 exposure.
Intracranial hypertension (papilledema)
Intracranial hypertension occurred in 3 of the 71 Increlex subjects. The label recommends funduscopic examination at the start of therapy and periodically. New, severe, or persistent headache — especially with visual changes — warrants medical evaluation.
Organ growth and visceral hypertrophy
Increlex labeling notes rapid increases in renal and splenic length in some patients. In the research community, sustained or supraphysiologic IGF-1 exposure is associated with progressive abdominal distension (sometimes called 'GH gut') and concern for cardiac hypertrophy. Organ-growth changes are believed to be largely irreversible, which is the strongest argument behind the 4-6 week cycle ceiling.
Fluid retention, joint discomfort, headache
Mild edema, joint stiffness, and headaches are commonly reported in the IGF-1 pathway literature, including IGF-1 LR3 community reports. These are typically dose-dependent and reversible with dose reduction or cycle discontinuation.
Injection site reactions
Lipohypertrophy, irritation, redness, and bruising can occur at injection sites. Site rotation and proper technique reduce frequency. The Increlex label also identifies injection-site lipohypertrophy as a recognized adverse reaction.
Cancer-pathway concern
IGF-1 signaling is mitogenic and anti-apoptotic, two properties relevant to cancer biology. In 2-year rat carcinogenicity studies referenced in the Increlex label, increased mammary and skin tumor incidence occurred at high IGF-1 exposure. Tomas et al. (1997) reported that IGF-1 LR3 supported protein turnover in tumor-bearing rats but also increased tumor growth in that model. Broader epidemiology (LeRoith 2003; Pollak 2008) has linked higher circulating IGF-1 to elevated risk of certain cancers in human cohorts. This is not the same as proving short-term IGF-1 LR3 use causes cancer in healthy adults — it is a real biological-mechanism concern that supports cycle limits and absolute contraindication in anyone with cancer history.
Endogenous GH suppression
Exogenous IGF-1 can suppress pituitary GH secretion through hypothalamic-pituitary feedback. This is one reason most IGF-1 LR3 protocols avoid late-evening dosing — dosing close to bedtime is more likely to coincide with the natural overnight GH pulse.
IGF-1 LR3 Timeline & What to Monitor
There is no validated efficacy timeline for IGF-1 LR3 in humans. The framework below combines what the Increlex (mecasermin) program tracked and what research-community protocols routinely report. It is a monitoring framework, not a results promise.
Common observation framework across an IGF-1 LR3 cycle
Window
Week 1
What's commonly tracked
Fasting blood glucose, hypoglycemic symptoms, injection-site response
What it tells you
Hypoglycemia frequency was highest in the first month of Increlex treatment. Daily glucose checks in this window are the highest-yield monitoring.
Window
Weeks 2-3
What's commonly tracked
Resting weight, waist circumference, fasting glucose trend
What it tells you
Identifies early water retention or unusual abdominal expansion.
Window
Weeks 3-4
What's commonly tracked
Fasting insulin, fasting glucose, performance markers
What it tells you
Insulin trends are most informative around the 3-4 week mark in research-community reports.
Window
End of cycle
What's commonly tracked
Repeat fasting glucose, fasting insulin, waist circumference
What it tells you
Comparison vs. baseline. A clean off-cycle requires these to return to baseline before any subsequent cycle.
Window
Off-cycle (4+ weeks)
What's commonly tracked
Symptom resolution, fasting markers
What it tells you
Off-time is when insulin sensitivity and IGF-1 receptor sensitivity recover.
| Window | What's commonly tracked | What it tells you |
|---|---|---|
| Week 1 | Fasting blood glucose, hypoglycemic symptoms, injection-site response | Hypoglycemia frequency was highest in the first month of Increlex treatment. Daily glucose checks in this window are the highest-yield monitoring. |
| Weeks 2-3 | Resting weight, waist circumference, fasting glucose trend | Identifies early water retention or unusual abdominal expansion. |
| Weeks 3-4 | Fasting insulin, fasting glucose, performance markers | Insulin trends are most informative around the 3-4 week mark in research-community reports. |
| End of cycle | Repeat fasting glucose, fasting insulin, waist circumference | Comparison vs. baseline. A clean off-cycle requires these to return to baseline before any subsequent cycle. |
| Off-cycle (4+ weeks) | Symptom resolution, fasting markers | Off-time is when insulin sensitivity and IGF-1 receptor sensitivity recover. |
These are observational markers. None of them constitute clinical monitoring guidance — they describe what research-community protocols typically track.
Stopping points reported in research community protocols. Persistent or severe hypoglycemic episodes despite proper meal timing. Progressive abdominal distension or waist increase that cannot be explained by training/nutrition. New persistent headaches, especially with visual symptoms (consistent with intracranial-hypertension warning in the Increlex label). Any new or growing lump, mole, or skin lesion — IGF-1 LR3 is not advisable in any context that could be malignant.
IGF-1 LR3 Clinical Evidence Context
Direct human evidence on IGF-1 LR3
There are no published human clinical trials of IGF-1 LR3 itself. ClinicalTrials.gov does not list any active or completed IGF-1 LR3 efficacy or safety study. The evidence base is preclinical for IGF-1 LR3 specifically, with adjacent human data from native rhIGF-1 (mecasermin/Increlex).
Preclinical potency benchmark
Tomas et al. (1996, Journal of Endocrinology) reported IGF-1 LR3 was 1.5-2x more potent than equimolar native IGF-1 for body weight gain, organ growth, and anti-catabolic effects when continuously infused in normal and dexamethasone-treated rats.
Preclinical anabolic effect in catabolic states
Tomas et al. (1992, Biochemical Journal) showed IGF-1 LR3 produced larger anabolic responses than native IGF-1 in dexamethasone-induced muscle catabolism in rats.
Preclinical mitogenic concern
Tomas et al. (1997, Journal of Endocrinology) reported that IGF-1 LR3 supported protein turnover in tumor-bearing catabolic rats but also increased tumor growth in that model.
Vascular biology
von der Thusen et al. (2011, American Journal of Pathology) reported that IGF-1 had plaque-stabilizing effects in a mouse atherosclerosis model — useful as a half-life reference (~20-30 hours) and pathway marker.
Adjacent human safety: Increlex (mecasermin) FDA label
71 pediatric patients with severe primary IGFD treated for a mean of 3.9 years. Hypoglycemia in 42%, tonsillar hypertrophy in 15%, intracranial hypertension in 3 subjects. This is the closest human dataset informing IGF-1 LR3 risk.
Adjacent human efficacy in non-growth indications
Borasio et al. (1998, Neurology) and Sorenson et al. (2008, Neurology) tested SubQ native rhIGF-1 in adult ALS patients. Neither trial showed primary-endpoint benefit. These trials inform what native IGF-1 does in adults at clinical-grade doses, even though they target a different indication.
Cancer epidemiology context
LeRoith & Roberts (2003) and Pollak (2008) summarize the body of evidence linking elevated circulating IGF-1 to risk of certain cancers. Not specific to IGF-1 LR3 but pathway-relevant.
Anti-doping detection
Mongongu et al. (2020, Drug Testing and Analysis) developed an immunopurification + high-resolution mass spectrometry method to detect Long R3-IGF-I and Des(1-3)-IGF-I in athlete samples — establishing that IGF-1 LR3 is detectable by current anti-doping methods.
The pattern is consistent: strong mechanistic plausibility from preclinical data and adjacent human safety, no direct human efficacy or long-term safety data on IGF-1 LR3 itself. Any claim about expected human results in performance contexts goes beyond the published evidence.
IGF-1 LR3 Storage & Handling
IGF-1 LR3 Storage Reference
State
Lyophilized (powder)
Storage
-4°F (-20°C) freezer
Duration
Long-term storage, up to roughly 12 months.
State
Lyophilized (powder)
Storage
35.6-46.4°F (2-8°C) refrigerator
Duration
Several months.
State
Lyophilized (powder)
Storage
Room temperature
Duration
Tolerated for shipping/transit windows of weeks; minimize exposure.
State
Reconstituted (liquid)
Storage
35.6-46.4°F (2-8°C) refrigerator
Duration
Approximately 28-30 days.
State
Reconstituted (liquid)
Storage
-4°F (-20°C) freezer
Duration
Not recommended; freeze-thaw can damage the peptide.
| State | Storage | Duration |
|---|---|---|
| Lyophilized (powder) | -4°F (-20°C) freezer | Long-term storage, up to roughly 12 months. |
| Lyophilized (powder) | 35.6-46.4°F (2-8°C) refrigerator | Several months. |
| Lyophilized (powder) | Room temperature | Tolerated for shipping/transit windows of weeks; minimize exposure. |
| Reconstituted (liquid) | 35.6-46.4°F (2-8°C) refrigerator | Approximately 28-30 days. |
| Reconstituted (liquid) | -4°F (-20°C) freezer | Not recommended; freeze-thaw can damage the peptide. |
Manufacturer data for commercial Long R3 IGF-I research reagents may indicate different stability windows. Always defer to the supplier's actual COA and product label.
Protect from light, avoid freeze-thaw cycles on reconstituted solution, and inspect the vial for clarity and absence of particles before each draw. Use a fresh sterile syringe for every administration. Discard reconstituted vials at the end of the listed window even if liquid remains.
IGF-1 LR3 Protocol Mistakes & Troubleshooting
- 01
Hypoglycemic symptoms after injection
If shakiness, sweating, confusion, or rapid heartbeat appear, eat fast-acting carbohydrates immediately (juice, glucose tablets, white bread). Symptoms that don't resolve in 10-15 minutes warrant urgent medical attention. Reduce the next dose and consider returning to the assessment phase.
- 02
Missed dose
Skip the missed dose. Continue with the next regularly scheduled injection. Never double-dose to compensate — the additive hypoglycemia risk outweighs any signaling benefit.
- 03
Cloudy or particulate solution
Do not draw from a cloudy or visibly particulate vial. This can indicate microbial contamination or peptide degradation. Discard and reconstitute a new vial.
- 04
Wrong BAC water volume added
Recalculate concentration with the actual volume used and adjust draw volume accordingly. Use the reconstitution calculator to confirm units before injecting.
- 05
Persistent injection-site reactions
Rotate sites systematically (do not reuse the same square inch within a 7-day window). Persistent lumps may indicate lipohypertrophy — give that site a long break and report unusual changes to a clinician.
- 06
Progressive abdominal distension
If waist circumference rises despite stable body composition and training, discontinue the cycle. This is the warning sign for visceral organ growth, which is largely irreversible.
- 07
New or worsening headaches
Especially with visual symptoms, this can mirror intracranial hypertension reported in the Increlex label. Stop the cycle and seek medical evaluation.
- 08
Storage error (vial left at room temperature)
Lyophilized peptide tolerates short room-temperature exposure. Reconstituted solution exposed to room temperature for more than a few hours, or to direct heat or freeze-thaw cycles, should be discarded.
- 09
Unsure about a dose calculation
Do not estimate. Use the calculator linked above. Inaccurate draws are the most common avoidable cause of hypoglycemia at the higher end of the dose range.
If symptoms ever escalate beyond what oral glucose can manage, treat it as a medical emergency. Severe hypoglycemia caused 4 hospital-grade seizures or loss-of-consciousness events out of 71 patients in the Increlex program — it is not a theoretical risk.
IGF-1 LR3 Regulatory Status
United States (as of June 2026). IGF-1 LR3 is not FDA-approved for any human therapeutic indication. It has no approved drug application. It is sold as a research reagent (research chemical, not for human use) by suppliers operating in the gray-market peptide space. Native rhIGF-1 (mecasermin, brand name Increlex) is FDA-approved only for the long-term treatment of growth failure in pediatric patients with severe primary IGF-1 deficiency or with GH gene deletion who have developed neutralizing antibodies to GH. There is no FDA-approved adult or athletic indication for any IGF-1 product.
European Union (as of June 2026). Increlex (mecasermin) is authorized by the European Medicines Agency for the same pediatric severe primary IGFD indication. IGF-1 LR3 is not separately authorized.
WADA (as of June 2026). IGF-1 and its analogs — including IGF-1 LR3 — are listed under S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics) and are prohibited at all times, in and out of competition. Mongongu et al. (2020) published a validated detection assay specific to LongR3-IGF-I, Des(1-3)-IGF-I, and R3-IGF-I in athlete samples.
Compounding pharmacies. Mecasermin is the compound a 503A or 503B compounding pharmacy can dispense — and only with a prescription and a clinical indication. IGF-1 LR3 specifically is not a compoundable product through standard pharmacy channels.
IGF-1 LR3 vs IGF-1 DES vs HGH vs Mecasermin
These four compounds all touch the GH/IGF-1 axis, but they act at different points and behave very differently. The table below organizes the practical differences.
IGF-1 LR3 vs IGF-1 DES (1-3) vs HGH (Somatropin) vs Mecasermin (Native rhIGF-1)
Feature
Type
IGF-1 LR3
Synthetic IGF-1 analog
IGF-1 DES (1-3)
Truncated IGF-1 variant
HGH (Somatropin)
Recombinant growth hormone
Mecasermin (Increlex)
Recombinant native human IGF-1
Feature
Amino acids
IGF-1 LR3
83
IGF-1 DES (1-3)
67
HGH (Somatropin)
191
Mecasermin (Increlex)
70 (identical to endogenous IGF-1)
Feature
Half-life
IGF-1 LR3
20-30 hours
IGF-1 DES (1-3)
~20-30 minutes
HGH (Somatropin)
2-3 hours
Mecasermin (Increlex)
~5.8 hours
Feature
Receptor potency
IGF-1 LR3
~3x native IGF-1
IGF-1 DES (1-3)
~10x native IGF-1 (locally)
HGH (Somatropin)
Indirect (drives endogenous IGF-1)
Mecasermin (Increlex)
1x (it is native IGF-1)
Feature
Action
IGF-1 LR3
Systemic, long-acting
IGF-1 DES (1-3)
Localized, rapid
HGH (Somatropin)
Systemic upstream cascade
Mecasermin (Increlex)
Systemic, replacement therapy
Feature
Dosing frequency
IGF-1 LR3
Once daily
IGF-1 DES (1-3)
2-3x daily
HGH (Somatropin)
1-2x daily
Mecasermin (Increlex)
Twice daily SubQ
Feature
Common dose context
IGF-1 LR3
20-100 mcg/day (research)
IGF-1 DES (1-3)
50-150 mcg/day split (research)
HGH (Somatropin)
2-8 IU/day (research)
Mecasermin (Increlex)
0.04-0.12 mg/kg twice daily (clinical)
Feature
IGFBP binding
IGF-1 LR3
Very low
IGF-1 DES (1-3)
Very low
HGH (Somatropin)
N/A (acts upstream)
Mecasermin (Increlex)
Normal (full IGFBP affinity)
Feature
FDA status
IGF-1 LR3
Not approved
IGF-1 DES (1-3)
Not approved
HGH (Somatropin)
FDA-approved (multiple indications)
Mecasermin (Increlex)
FDA-approved (pediatric severe primary IGFD)
Feature
WADA status
IGF-1 LR3
Prohibited
IGF-1 DES (1-3)
Prohibited
HGH (Somatropin)
Prohibited
Mecasermin (Increlex)
Prohibited
Feature
Practical note
IGF-1 LR3
Long-acting IGF-1 analog with the most accumulated community data
IGF-1 DES (1-3)
Localized, rapid signaling; very short window
HGH (Somatropin)
Broadest endocrine effect; clinical-grade product
Mecasermin (Increlex)
The clinical reference compound for everything else in this column
| Feature | IGF-1 LR3 | IGF-1 DES (1-3) | HGH (Somatropin) | Mecasermin (Increlex) |
|---|---|---|---|---|
| Type | Synthetic IGF-1 analog | Truncated IGF-1 variant | Recombinant growth hormone | Recombinant native human IGF-1 |
| Amino acids | 83 | 67 | 191 | 70 (identical to endogenous IGF-1) |
| Half-life | 20-30 hours | ~20-30 minutes | 2-3 hours | ~5.8 hours |
| Receptor potency | ~3x native IGF-1 | ~10x native IGF-1 (locally) | Indirect (drives endogenous IGF-1) | 1x (it is native IGF-1) |
| Action | Systemic, long-acting | Localized, rapid | Systemic upstream cascade | Systemic, replacement therapy |
| Dosing frequency | Once daily | 2-3x daily | 1-2x daily | Twice daily SubQ |
| Common dose context | 20-100 mcg/day (research) | 50-150 mcg/day split (research) | 2-8 IU/day (research) | 0.04-0.12 mg/kg twice daily (clinical) |
| IGFBP binding | Very low | Very low | N/A (acts upstream) | Normal (full IGFBP affinity) |
| FDA status | Not approved | Not approved | FDA-approved (multiple indications) | FDA-approved (pediatric severe primary IGFD) |
| WADA status | Prohibited | Prohibited | Prohibited | Prohibited |
| Practical note | Long-acting IGF-1 analog with the most accumulated community data | Localized, rapid signaling; very short window | Broadest endocrine effect; clinical-grade product | The clinical reference compound for everything else in this column |
These compounds are not interchangeable. Mecasermin is the only FDA-approved IGF-1 product in the column.
IGF-1 LR3 Blood Tests & Monitoring
IGF-1 LR3 directly relates to the IGF pathway rather than simply nudging GH pulses. Monitoring focuses on glucose handling, IGF-axis context, cardiovascular risk, and symptoms that may suggest excessive pathway activity.
Blood test markers to discuss with a clinician
Marker
IGF-1
Why it matters
Provides IGF-axis context, although interpretation can be complex with IGF analog exposure.
Timing
Follow-up
Marker
Fasting glucose
Why it matters
IGF-related activity can affect glucose handling, so current glucose context matters.
Timing
Follow-up
Marker
A1c
Why it matters
Shows longer-term glucose control before and during IGF-related protocols.
Timing
Baseline
Marker
Lipid panel
Why it matters
Adds cardiometabolic context during body-composition or growth-pathway research.
Timing
Baseline
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver, kidney, electrolyte, and glucose context in one broad panel.
Timing
Baseline
| Marker | Why it matters | Timing |
|---|---|---|
| IGF-1 | Provides IGF-axis context, although interpretation can be complex with IGF analog exposure. | Follow-up |
| Fasting glucose | IGF-related activity can affect glucose handling, so current glucose context matters. | Follow-up |
| A1c | Shows longer-term glucose control before and during IGF-related protocols. | Baseline |
| Lipid panel | Adds cardiometabolic context during body-composition or growth-pathway research. | Baseline |
| Comprehensive metabolic panel (CMP) | Reviews liver, kidney, electrolyte, and glucose context in one broad panel. | Baseline |
Monitoring guidance is IGF-pathway-based because IGF-1 LR3 does not have established routine clinical monitoring standards.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with diabetes risk, cancer history, edema, nerve symptoms, or active growth-related medical concerns.
Follow-up
Re-check glucose markers and relevant metabolic markers after 4-8 weeks or sooner if symptoms change.
Longer term
For longer or repeated protocols, review trends every 3 months with a clinician.
How to interpret the labs
- IGF-related compounds require more caution than indirect GH-pulse support because the pathway is closer to growth signaling.
- Cancer history, abnormal growths, edema, nerve symptoms, and glucose issues need clinician-guided interpretation.
- A normal lab panel does not prove growth-pathway exposure is risk-free.
Do not wait for routine labs
Severe headaches, vision changes, fainting, chest pain, rapid swelling, or neurologic symptoms need medical review. Symptoms of low blood sugar, such as sweating, shakiness, confusion, or weakness, should be reviewed promptly.
FAQ
Q1: What is IGF-1 LR3?
IGF-1 LR3 (Long Arginine-3 IGF-1) is a synthetic, longer-acting analog of human insulin-like growth factor 1. It carries an arginine substitution at position 3 and a 13-amino-acid N-terminal extension, giving it 83 amino acids total versus 70 for native IGF-1. The structural changes lower its affinity for IGF binding proteins and stretch its half-life to roughly 20-30 hours. It is sold as a research reagent and is not FDA-approved for any human use.
Q2: What is the half-life of IGF-1 LR3?
Approximately 20-30 hours, compared to roughly 12-15 hours for native IGF-1. The longer half-life is the reason once-daily dosing is the standard schedule across research-community protocols.
Q3: What dose ranges appear in IGF-1 LR3 research protocols?
Research-community sources cluster between 20 and 100 mcg per day, given as one daily SubQ or IM injection. Lower-end ranges (20-40 mcg/day) are most commonly cited for tolerance assessment and women's protocols. Above roughly 50-60 mcg/day, side-effect frequency rises faster than the perceived signaling benefit. None of these ranges are validated clinical doses.
Q4: How is IGF-1 LR3 reconstituted?
Add bacteriostatic water to the lyophilized vial, pouring slowly down the inside wall — never directly onto the powder. Swirl gently, do not shake. Refrigerate immediately at 2-8°C. A 1 mg vial reconstituted with 2 mL of BAC water gives 500 mcg/mL; a 50 mcg dose at that concentration is 0.10 mL (10 units on a U-100 insulin syringe). For custom math, use the Pep Pal calculator.
Q5: What is the standard cycle length?
Most research-community protocols cap on-time at 4-6 weeks with at least equal time off between cycles. The ceiling reflects observed patterns of progressive insulin resistance, organ-growth concern, and IGF-1 receptor desensitization. Continuous multi-month use is widely discouraged.
Q6: How real is the hypoglycemia risk?
Very real. In the Increlex (native mecasermin) FDA-approved program, hypoglycemia was reported in 42% of subjects, with five subjects experiencing severe episodes requiring assistance and four experiencing seizures or loss of consciousness. The rate was highest in the first month. Mitigation is consistent across all sources: eat 30-50 grams of fast-acting carbohydrates within 30 minutes of every injection, never inject fasted, never inject before sleep, and keep glucose tablets accessible during cycles.
Q7: Should IGF-1 LR3 be injected SubQ or IM?
Both routes are used in research protocols. SubQ is simpler and is the most-cited default. IM injection into a freshly trained muscle is reported in research interest in localized hyperplasia signaling, though the long half-life means the peptide distributes systemically regardless of site. Same hypoglycemia rules apply to both routes.
Q8: Can IGF-1 LR3 be combined with insulin?
No. The combination produces additive hypoglycemia and has been associated with hospitalizations in research-community reporting. Both compounds lower blood glucose and the combined effect is unpredictable. This is treated as an absolute contraindication across virtually every published research-community source.
Q9: Does IGF-1 LR3 increase cancer risk?
IGF-1 signaling is mitogenic and anti-apoptotic — both relevant to cancer biology. The Increlex label cites preclinical 2-year rat carcinogenicity studies in which increased mammary and skin tumor incidence occurred at high IGF-1 exposure. Tomas et al. (1997) reported that IGF-1 LR3 increased tumor growth in tumor-bearing catabolic rats. Epidemiological literature (LeRoith 2003; Pollak 2008) has linked elevated circulating IGF-1 to higher risk of certain cancers in human cohorts. Anyone with active or prior cancer, or strong family history, should not use IGF-1 LR3.
Q10: Why never inject IGF-1 LR3 before bed?
Two reasons. First, hypoglycemic episodes during sleep are harder to detect and respond to. Second, exogenous IGF-1 can suppress the natural overnight GH pulse through hypothalamic-pituitary feedback. Most research protocols schedule injections at least 2-3 hours before bedtime.
Q11: What vial sizes are common?
1 mg (1,000 mcg) and 0.1 mg (100 mcg) lyophilized vials are the most common research-grade sizes. The 1 mg vial is more practical for full cycles; 0.1 mg vials are usually used for short cycles or first-time tolerance assessment.
Q12: Is IGF-1 LR3 FDA-approved?
No. IGF-1 LR3 is not FDA-approved for any human therapeutic use. The closest FDA-approved IGF-1 product is mecasermin (Increlex), native recombinant human IGF-1, approved only for the long-term treatment of growth failure in pediatric patients with severe primary IGF-1 deficiency or GH gene deletion with neutralizing antibodies. There is no adult or performance-related FDA indication for any IGF-1 product.
Q13: Is IGF-1 LR3 banned by WADA?
Yes. IGF-1 LR3 falls under the World Anti-Doping Agency's S2 category (peptide hormones, growth factors, related substances, and mimetics) and is prohibited at all times — both in and out of competition. Mongongu et al. (2020) published a validated detection method for IGF-1 LR3 in athlete samples.
Sources & Research
- 1. Tomas FM, Lemmey AB, Read LC, Ballard FJ. Superior potency of infused IGF-I analogues which bind poorly to IGF-binding proteins is maintained when administered by injection. Journal of Endocrinology (1996)
- 2. Tomas FM, Knowles SE, Owens PC, Chandler CS, Francis GL, Read LC, Ballard FJ. Insulin-like growth factor-I (IGF-I) and especially IGF-I variants are anabolic in dexamethasone-treated rats. Biochemical Journal (1992)
- 3. Mohan S, Baylink DJ. IGF-binding proteins are multifunctional and act via IGF-dependent and -independent mechanisms. Journal of Endocrinology (2002)
- 4. von der Thusen JH, Borensztajn KS, Moimas S, et al. IGF-1 has plaque-stabilizing effects in atherosclerosis by altering vascular smooth muscle cell phenotype. American Journal of Pathology (2011)
- 5. Ipsen Biopharmaceuticals. INCRELEX (mecasermin) injection — Highlights of Prescribing Information (2025 revision). FDA accessdata.fda.gov (2025)
- 6. European Medicines Agency. Increlex EPAR — Product Information (mecasermin). EMA (2024)
- 7. LeRoith D, Roberts CT Jr. The insulin-like growth factor system and cancer. Cancer Letters (2003)
- 8. Pollak M. Insulin and insulin-like growth factor signalling in neoplasia. Nature Reviews Cancer (2008)
- 9. Borasio GD, Robberecht W, Leigh PN, et al. A placebo-controlled trial of insulin-like growth factor-I in amyotrophic lateral sclerosis. Neurology (1998)
- 10. Sorenson EJ, Windbank AJ, Mandrekar JN, et al. Subcutaneous IGF-1 is not beneficial in 2-year ALS trial. Neurology (2008)
- 11. Mongongu C, Coudore F, Domergue V, et al. Detection of LongR3-IGF-I, Des(1-3)-IGF-I, and R3-IGF-I using immunopurification and high resolution mass spectrometry for antidoping purposes. Drug Testing and Analysis (2020)
- 12. Bailes J, Soloviev M. Insulin-Like Growth Factor-1 (IGF-1) and Its Monitoring in Medical Diagnostic and in Sports. Biomolecules (2021)
- 13. Velloso CP. Regulation of muscle mass by growth hormone and IGF-I. British Journal of Pharmacology (2008)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page