TB-500 Quick Start
TB-500 is a synthetic 7-amino-acid fragment of thymosin beta-4, a larger peptide found throughout the body. Its sequence is Ac-LKKTETQ, which matches amino acids 17-23 of thymosin beta-4 (Tbeta-4). The "Ac" prefix means one end is acetylated, a modification that can slow breakdown.
One point matters throughout this guide: TB-500 is not the same thing as full-length thymosin beta-4. Most human research used the full 43-amino-acid peptide, not the 7-amino-acid TB-500 fragment. The fragment keeps the actin-binding region, but it does not include the rest of the parent peptide.
Route
Most research-use protocols use subcutaneous injection. Some animal protocols use intramuscular or intraperitoneal.
Concentration
A 10 mg vial mixed with 2 mL bacteriostatic water gives 5 mg/mL. On a U-100 syringe, 10 units is 0.10 mL, or about 500 mcg.
Schedule
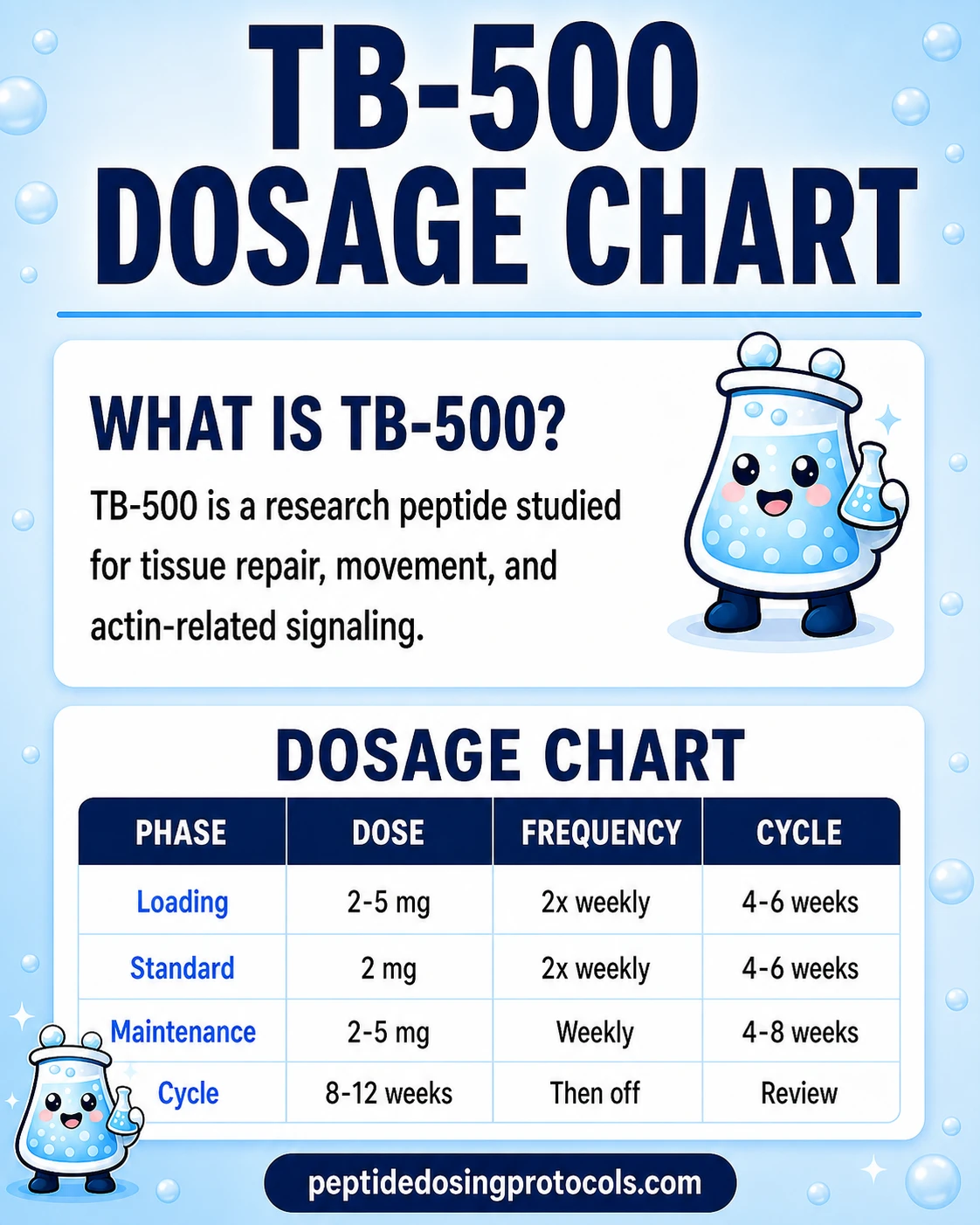
Community protocols typically use a loading phase (twice weekly) followed by a maintenance phase (once weekly).
Cycle length
Common research-use cycles are 4-12 weeks, with longer maintenance phases discussed less consistently.
Research status
Not FDA-approved. Removed from FDA 503A Category 2 on April 15, 2026; PCAC review scheduled for July 23, 2026 for potential 503A inclusion for wound healing.
Most of the practical research-use cycle planning for TB-500 (such as 2 mg twice weekly for 4-6 weeks then 2 mg once weekly) is community-derived and not validated by a published human RCT of the TB-500 fragment. Treat published cycle ranges as starting reference points for research planning, not personal dosing instructions.
Disclaimer
This page is an educational research reference and is not medical advice. TB-500 is not approved by the FDA for human use, is sold for research purposes only, and is on the World Anti-Doping Agency Prohibited List. Information about doses, cycles, and reconstitution is research-use planning information, not personal treatment guidance.
Use this protocol for TB-500 dosing, vial mixing, and cycle planning. For the wider research view, read the TB-500 repair peptide guide on how it works, studies, safety notes, and related peptides.
TB-500 Dosing Protocol & Schedule
There is no FDA-approved TB-500 dosing label. The closest human safety reference is a Phase 1 study of full-length thymosin beta-4, not TB-500. In that study, healthy volunteers received IV doses ranging from 42 mg to 1260 mg, followed by daily dosing for 14 days, with no dose-limiting toxicities. This is not a dosing recommendation. It does not prove injectable TB-500 is safe over weeks or months.
The numbers below are commonly referenced in research-use protocol planning by the community. They are not validated by human clinical trials of the TB-500 fragment.
TB-500 Dosing Patterns
Two patterns show up most often in research planning: a load-and-maintain schedule and a shorter acute-injury schedule.
Higher initial frequency for 4-6 weeks, then lower frequency for ongoing research-use cycles.
Loading phase (Weeks 1-6). A common research-use plan is approximately 2-2.5 mg subcutaneous twice weekly. At 5 mg/mL (10 mg vial in 2 mL), that is 0.4-0.5 mL per dose, or roughly 40-50 units on a U-100 insulin syringe. Twice weekly dosing produces about 4-5 mg per week.
Maintenance phase (Weeks 7+). Typical research-use plans drop to approximately 2-2.5 mg subcutaneous once weekly for ongoing cycles, or pause and re-evaluate. Some plans extend maintenance for 6-8 additional weeks; others stop after the loading phase. This is not a dosing recommendation.
Load + Maintenance research-use cycle planning (not a dosing recommendation)
Phase
Loading
Weekly amount
~4-5 mg/week
Frequency
Twice weekly
Duration
Weeks 1-6
Phase
Maintenance
Weekly amount
~2-2.5 mg/week
Frequency
Once weekly
Duration
Weeks 7-12
Phase
Off period
Weekly amount
0 mg
Frequency
None
Duration
4-8 weeks
| Phase | Weekly amount | Frequency | Duration |
|---|---|---|---|
| Loading | ~4-5 mg/week | Twice weekly | Weeks 1-6 |
| Maintenance | ~2-2.5 mg/week | Once weekly | Weeks 7-12 |
| Off period | 0 mg | None | 4-8 weeks |
These numbers come from community protocol references, not validated human TB-500 trial data.
Shorter pattern often referenced for soft-tissue research planning around an acute event.
Some research-use plans front-load the first two weeks at higher frequency, then taper. A pattern referenced in the community is roughly 2-2.5 mg every 2-3 days for 2 weeks, then 2-2.5 mg once weekly for 4-6 weeks. This is not a dosing recommendation.
Acute window research-use cycle planning (not a dosing recommendation)
Phase
Front-loading
Per-dose amount
~2-2.5 mg
Frequency
Every 2-3 days
Duration
Weeks 1-2
Phase
Taper
Per-dose amount
~2-2.5 mg
Frequency
Once weekly
Duration
Weeks 3-8
| Phase | Per-dose amount | Frequency | Duration |
|---|---|---|---|
| Front-loading | ~2-2.5 mg | Every 2-3 days | Weeks 1-2 |
| Taper | ~2-2.5 mg | Once weekly | Weeks 3-8 |
Front-loading patterns vary widely between research-use references. Use as a planning reference only.
Cycle Guidelines
Cycle structure references commonly used in research planning
Approach
Short cycle
Duration
4-6 weeks
Off period
4 weeks
Best for
Single research-question focus
Approach
Standard cycle
Duration
8-12 weeks
Off period
4-8 weeks
Best for
Most community-referenced plans
Approach
Maintenance after load
Duration
Once weekly, 6-12 weeks
Off period
Variable
Best for
Continuation after a 4-6 week loading phase
| Approach | Duration | Off period | Best for |
|---|---|---|---|
| Short cycle | 4-6 weeks | 4 weeks | Single research-question focus |
| Standard cycle | 8-12 weeks | 4-8 weeks | Most community-referenced plans |
| Maintenance after load | Once weekly, 6-12 weeks | Variable | Continuation after a 4-6 week loading phase |
There is no published human RCT of the TB-500 fragment establishing an optimal cycle length. Treat all cycle structures as research-use planning references.
Evidence boundary
The dosing ranges above reflect common research-use references. They have not been validated in a human RCT of TB-500 (Ac-LKKTETQ). The strongest human evidence is still for full-length thymosin beta-4 in topical (RGN-137) or ophthalmic (RGN-259) formulations, not injectable TB-500.
TB-500 Supplies Needed
Plan based on the standard load-and-maintenance schedule (about 2.5 mg twice weekly for 6 weeks, then 2.5 mg once weekly). Supplies math assumes 10 mg vials reconstituted with 2.0 mL bacteriostatic water (5 mg/mL). Affiliate disclosure: PDP may earn a commission when you use eligible supplier links, at no extra cost to you.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

TB-500 Supply

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials
Each 10 mg vial reconstituted with 2 mL BAC water = 5 mg/mL. About 4 doses of 2.5 mg per vial.
| Cycle length | Planning note |
|---|---|
4 weeks 2 vials | Loading only: 8 doses x 2.5 mg = 20 mg total. |
6 weeks 3 vials | Loading: 12 doses x 2.5 mg = 30 mg total. |
8 weeks 4 vials | 6-week loading + 2-week maintenance: 14 doses x 2.5 mg = 35 mg total; round up to 40 mg. |
12 weeks 5 vials | 6-week loading + 6-week maintenance: 18 doses x 2.5 mg = 45 mg total; round up to 50 mg. |
4 weeks
2 vials
Loading only: 8 doses x 2.5 mg = 20 mg total.
6 weeks
3 vials
Loading: 12 doses x 2.5 mg = 30 mg total.
8 weeks
4 vials
6-week loading + 2-week maintenance: 14 doses x 2.5 mg = 35 mg total; round up to 40 mg.
12 weeks
5 vials
6-week loading + 6-week maintenance: 18 doses x 2.5 mg = 45 mg total; round up to 50 mg.
Insulin Syringes (U-100)
Each 2.5 mg dose at 5 mg/mL is 0.5 mL = 50 units. Use 0.5 mL or 1 mL barrel U-100 syringes.
| Cycle length | Planning note |
|---|---|
4 weeks 8 syringes | 1 syringe per injection; recommend a 10-pack. |
6 weeks 12 syringes | 1 syringe per injection; recommend a 10-pack with 2 spare. |
8 weeks 14 syringes | 1 syringe per injection; recommend 1 x 10-pack plus extras. |
12 weeks 18 syringes | 1 syringe per injection; recommend 1 x 25-pack. |
4 weeks
8 syringes
1 syringe per injection; recommend a 10-pack.
6 weeks
12 syringes
1 syringe per injection; recommend a 10-pack with 2 spare.
8 weeks
14 syringes
1 syringe per injection; recommend 1 x 10-pack plus extras.
12 weeks
18 syringes
1 syringe per injection; recommend 1 x 25-pack.
Bacteriostatic Water
Use 2.0 mL per 10 mg vial. Each 10 mL bottle reconstitutes 5 vials.
| Cycle length | Planning note |
|---|---|
4-12 weeks 1 x 10 mL bottle | 4 weeks: 2 vials use 4 mL; 1 bottle has margin.; 6 weeks: 3 vials use 6 mL; 1 bottle has margin.; 8 weeks: 4 vials use 8 mL; 1 bottle has margin.; 12 weeks: 5 vials use 10 mL; 1 bottle covers the cycle exactly. |
4-12 weeks
1 x 10 mL bottle
4 weeks: 2 vials use 4 mL; 1 bottle has margin.; 6 weeks: 3 vials use 6 mL; 1 bottle has margin.; 8 weeks: 4 vials use 8 mL; 1 bottle has margin.; 12 weeks: 5 vials use 10 mL; 1 bottle covers the cycle exactly.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments. The supplies math above assumes 2.5 mg per dose from 10 mg vials. Adjust syringe draw volumes if planning a lower per-dose amount; BAC-water needs depend on vial count and chosen concentration.
Companion Supplies & Routine Support
TB-500 Reconstitution Guide
TB-500 ships as a lyophilized (freeze-dried) powder in a glass vial with a rubber stopper. It must be reconstituted with bacteriostatic water before drawing a dose. The amount of BAC water you add controls the final concentration, which determines how many syringe units equal each dose.
Reconstitution volumes for 10 mg TB-500 vials
Vial size
10 mg
BAC water
2.0 mL
Concentration
5.0 mg/mL
10 unit draw
0.10 mL = 500 mcg
100 unit draw
0.50 mL = 2.5 mg
Vial size
10 mg
BAC water
3.0 mL
Concentration
3.33 mg/mL
10 unit draw
0.10 mL = 333 mcg
100 unit draw
0.75 mL = 2.5 mg
| Vial size | BAC water | Concentration | 10 unit draw | 100 unit draw |
|---|---|---|---|---|
| 10 mg | 2.0 mL | 5.0 mg/mL | 0.10 mL = 500 mcg | 0.50 mL = 2.5 mg |
| 10 mg | 3.0 mL | 3.33 mg/mL | 0.10 mL = 333 mcg | 0.75 mL = 2.5 mg |
Pick a concentration that lets your typical research-use dose land on a clean unit mark. This page's default assumption is 10 mg in 2.0 mL because 50 units on a U-100 syringe equals 2.5 mg.
Reconstitution Steps
- 01
Inspect the vial
Confirm the label says TB-500, check the listed mass, and look for any cracks, contamination, or fluid in the powder vial.
- 02
Wipe both stoppers
Use a fresh alcohol swab on the BAC-water stopper and the TB-500 vial stopper. Let the alcohol air dry before piercing.
- 03
Draw the BAC water
Use a sterile syringe to draw the calculated BAC-water volume - 2.0 mL for the 10 mg / 5 mg/mL pairing.
- 04
Inject the BAC water slowly
Insert the needle through the TB-500 vial stopper and let the BAC water run down the inside wall of the vial. Avoid forceful streams onto the powder, which can foam the peptide.
- 05
Swirl to dissolve
Gently swirl or roll the vial. Do not shake. The solution should be clear and colorless within a minute or two. If it looks cloudy, do not use it.
- 06
Label and refrigerate
Write the reconstitution date on the vial. Store at 35.6-46.4 F (2-8 C). Use within 2-4 weeks; some references extend this to 30 days under proper refrigeration.
- 07
Draw the research dose
Use a fresh U-100 insulin syringe per session. Draw the planned volume, expel air bubbles, wipe the injection site, and inject subcutaneously. Rotate sites between sessions.
Reconstitution calculator
If your vial size or planned per-dose amount differs from the table above, use the PepPal reconstitution calculator to confirm the BAC-water volume and U-100 draw before mixing.
TB-500 Dosage Chart
This TB-500 dosage chart summarizes the common load-and-maintenance research schedule from 2-2.5 mg twice weekly to 2-2.5 mg once weekly, with dose escalation shown by phase.
How TB-500 Works
TB-500 research centers on actin, a structural protein cells use to move and change shape. The parent peptide, thymosin beta-4, helps regulate the pool of actin building blocks inside cells. That matters because wound repair depends on cells moving into the right area and rebuilding tissue in an organized way.
The important point: TB-500 keeps the actin-binding region of thymosin beta-4, but it does not include the rest of the parent peptide. That is why this page separates TB-500 fragment data from full-length thymosin beta-4 data.
Actin sequestration
Tbeta-4 binds G-actin monomers and is one of the major regulators of the monomeric actin pool. The TB-500 fragment retains this binding motif.
Cell migration
Preclinical work shows Tbeta-4 promotes migration of keratinocytes, endothelial cells, fibroblasts, myoblasts, and corneal epithelial cells in injury models.
Angiogenesis
In animal models, Tbeta-4 promotes new blood vessel formation in dermal wounds and ischemic cardiac tissue.
Anti-inflammatory effects
Tbeta-4 reduces inflammatory mediators in corneal injury models and reduces matrix metalloproteinase levels after alkali burn in animal eyes.
Boundary
Most of these mechanism findings are reported for full-length thymosin beta-4. Some are confirmed in fragment-only experiments; others are extrapolated.
Who TB-500 Research Is For and Who Should Avoid It
TB-500 is a research peptide with no FDA-approved clinical use. Decisions about personal use belong with a qualified clinician, not a research protocol page. The points below are general research-use boundaries, not a clinical eligibility list.
Athletes subject to drug testing
TB-500 and all thymosin beta-4 derivatives are explicitly prohibited by WADA under Section S0 (Non-Approved Substances), at all times. Detection windows are reported in the 30-45 day range. Athletes in WADA-tested sports, NCAA athletes, and military personnel under WADA-aligned testing should avoid use.
People with active or prior cancer
Tbeta-4 is associated with increased metastatic potential in some tumor models in the literature. This is a theoretical concern in active or prior cancer and is consistently flagged in research-use safety discussions, not a settled clinical risk.
Pregnancy and lactation
There are no human data establishing safety in pregnancy or lactation. Avoid in those contexts.
Allergies to peptide preparations or BAC-water preservatives
Benzyl alcohol (the preservative in bacteriostatic water) can cause allergic reactions in a small number of users. Confirm tolerance before research-use protocols that involve repeated injections.
Active infection at the planned injection site
Standard injection-site cautions apply: do not inject into broken, infected, inflamed, or recently bruised skin.
Anyone seeking treatment for a specific medical condition
TB-500 is not a treatment. People looking for clinical care for a wound, tendon injury, or cardiovascular condition should work with a clinician through approved care pathways.
TB-500 Side Effects & Safety
Direct human safety data for the 7-amino-acid TB-500 fragment is essentially absent. The closest reference is a Phase 1 study of full-length thymosin beta-4. In that study, 40 healthy volunteers received IV doses up to 1260 mg daily for 14 days, with no serious adverse events or dose-limiting toxicities. That safety signal does not automatically carry over to subcutaneous TB-500 fragment use over weeks or months.
Most commonly reported in research-use community
Mild injection-site discomfort, redness, and short-lived fatigue or head-pressure feelings in the first few days of a cycle.
Theoretical: cancer / unwanted angiogenesis
Tbeta-4 levels are elevated in some metastatic cancers and the peptide promotes angiogenesis. Whether sub-therapeutic injections of the fragment carry a meaningful risk in healthy adults has not been studied.
Theoretical: immune modulation
Tbeta-4 regulates inflammatory signaling. Long-term immune effects in repeated cycles are not characterized in humans.
Quality control risk
Research-use peptides are produced outside FDA-approved manufacturing pipelines. Purity, sterility, and identity vary between suppliers. A Certificate of Analysis specific to the lot is the minimum quality reference.
Injection-site issues
Standard subcutaneous injection risks: local irritation, lipohypertrophy from poor site rotation, infection from poor technique.
TB-500 Timeline & What to Monitor
The human timelines we have do not come from injectable TB-500. They come from topical thymosin beta-4 wound studies and eye-drop studies. In one venous-ulcer trial, healing was faster among responders, and about 25% of patients reached complete closure within 3 months. That does not translate directly to a subcutaneous TB-500 cycle.
Reported in research-use community
Some research-use planners describe perceived recovery improvements within the first 2-4 weeks of a loading cycle. These are anecdotal observations, not trial endpoints.
Reasonable to monitor
Injection site condition, sleep quality, cycle adherence, and any new or unusual symptoms. Baseline and end-of-cycle resting heart rate and blood pressure are simple references.
Cannot be promised
Faster healing of a specific injury, structural tendon repair, joint regeneration, or any specific clinical outcome.
When to stop
Any new chest, abdominal, or neurological symptom; persistent injection-site reactions; or any worrying systemic symptom. Stop and seek qualified medical care.
TB-500 Clinical Evidence Context
There is no published human RCT of injectable TB-500 (the 7-amino-acid fragment) for any indication. Human evidence belongs mostly to full-length thymosin beta-4, not TB-500. The strongest data are topical wound studies, ophthalmic studies, and one IV Phase 1 safety trial.
Full-length Tbeta-4, Phase 1 IV safety
Ruff et al. (2010), 40 healthy volunteers, single IV doses 42-1260 mg then daily x 14 days, no dose-limiting toxicities. Establishes that IV Tbeta-4 was tolerated short-term, not that the fragment is safe long-term subcutaneously.
Full-length Tbeta-4, Phase 2 dermal wound (venous ulcers)
Guarnera et al. (2010), 73 patients across 8 European sites, double-blind placebo-controlled topical 0.0001-0.03% Tbeta-4 over 12 weeks. Safety profile acceptable. About 25% complete healing in 3 months at the 0.03% dose, with stronger response in smaller wounds.
Full-length Tbeta-4, Phase 2 pressure ulcer
RegeneRx-sponsored Phase 2 trial (NCT00382174) of topical 0.01-0.1% Tbeta-4. Acceleration of healing reported in patients who responded.
Full-length Tbeta-4, Phase 3 ophthalmic (RGN-259)
SEER-1 Phase 3 trial of 0.1% topical Tbeta-4 ophthalmic solution in neurotrophic keratopathy stages 2-3. Reported faster complete healing at 4 weeks vs. placebo, no safety issues.
TB-500 fragment, preclinical only
The TB-500 fragment retains actin-binding behavior in cell-biology and in-vivo animal experiments. Specific human evidence for the fragment is absent.
Cardiac preclinical
Bock-Marquette et al. (2004) showed Tbeta-4 reduces infarct volume and preserves cardiac function in mouse coronary ligation models. Subsequent work in mice and a porcine MI model has reported similar effects. No human cardiac endpoint trial has been completed for systemic Tbeta-4.
Tendon and ligament preclinical
Kim & Bhatt (2013) reported improved collagen organization and fibril diameter at 4 weeks after fibrin-sealant Tbeta-4 delivery in a rat MCL transection model. No human trial.
Evidence boundary
The widespread research-use claim that injectable TB-500 fragment 'heals tendons and ligaments in humans' is not supported by a published human RCT. It rests on extrapolation from preclinical full-length Tbeta-4 work.
TB-500 Storage & Handling
TB-500 storage references
State
Lyophilized (powder)
Storage
-4 F (-20 C) long-term
Notes
Refrigerator (35.6-46.4 F / 2-8 C) is acceptable for shorter-term storage; freezer is preferred for longer storage.
State
Reconstituted (liquid)
Storage
35.6-46.4 F (2-8 C)
Notes
Use within 2-4 weeks. Some references extend to 30 days under proper refrigeration.
State
In transit
Storage
Cool and dark
Notes
Brief exposure to ambient temperature is generally tolerated by lyophilized peptide; check supplier guidance for the specific product.
State
Light exposure
Storage
Avoid
Notes
Store both lyophilized and reconstituted vials in the original carton or a dark drawer of the refrigerator.
| State | Storage | Notes |
|---|---|---|
| Lyophilized (powder) | -4 F (-20 C) long-term | Refrigerator (35.6-46.4 F / 2-8 C) is acceptable for shorter-term storage; freezer is preferred for longer storage. |
| Reconstituted (liquid) | 35.6-46.4 F (2-8 C) | Use within 2-4 weeks. Some references extend to 30 days under proper refrigeration. |
| In transit | Cool and dark | Brief exposure to ambient temperature is generally tolerated by lyophilized peptide; check supplier guidance for the specific product. |
| Light exposure | Avoid | Store both lyophilized and reconstituted vials in the original carton or a dark drawer of the refrigerator. |
Always defer to the supplier label and Certificate of Analysis for the specific stability data of the lot you have.
TB-500 Protocol Mistakes & Troubleshooting
- 01
Cloudy or discolored solution after reconstitution
Do not use. Cloudiness, particulates, or color changes can mean denatured peptide, contamination, or wrong diluent. Replace the vial.
- 02
Wrong BAC-water volume
If you added 3 mL to a 10 mg vial when planning 2 mL, the new concentration is 3.33 mg/mL. Recalculate the U-100 draw rather than re-mixing or 'topping off'.
- 03
Missed a scheduled session
Most research-use plans treat a single missed session as a skip rather than a double-dose. Resume the planned schedule at the next session.
- 04
Local injection-site reaction
Apply a clean cool compress, rotate sites, and pause if redness or swelling spreads or persists more than 48 hours. Do not inject into a reactive site.
- 05
Stronger-than-expected systemic effect
Stop dosing. Note the timing relative to the last injection. Seek qualified medical care for any chest, neurological, or persistent systemic symptom.
- 06
Storage mistake (left out at room temperature)
Brief room-temperature exposure of refrigerated reconstituted peptide is unlikely to ruin it. Extended exposure (many hours, especially warm) is a reason to discard and replace.
- 07
Confusion about vial concentration
Re-read the supplier label, the listed mass, and your reconstitution math. Do not draw based on memory; verify with the PepPal reconstitution calculator before injecting.
TB-500 Regulatory Status
As of June 2026. TB-500 is not approved by the FDA for any human use. It is sold as a research chemical, not a drug. The regulatory picture has changed materially in the past year and continues to evolve.
FDA 503A bulks list, September 2023
FDA placed 17 peptide bulk drug substances - including TB-500 - on Category 2 of the interim 503A bulks list, citing potential significant safety risks. 503A compounding pharmacies were not permitted to compound TB-500 from that point.
FDA 503A bulks list, April 15, 2026
FDA published an update removing 12 peptides from Category 2, including TB-500, because the original nominators withdrew their nominations. Removal took effect 7 days from notice. The peptides are not yet on Category 1 - removal from Category 2 is not approval and is not a green light for compounding.
FDA Pharmacy Compounding Advisory Committee, July 23, 2026
PCAC will discuss BPC-157, KPV, TB-500, and MOTs-C-related bulk drug substances for potential inclusion on the 503A Bulks List. The use FDA reviewed for TB-500 is wound healing. The committee meeting outcome will materially shape the legal compounding pathway.
WADA prohibited list
TB-500 and all thymosin beta-4 derivatives are prohibited under Section S0 (Non-Approved Substances) of the WADA Prohibited List, at all times. Detection windows reported are roughly 30-45 days.
Equine sport
TB-500 is also prohibited in horse racing under racing medication rules.
Internationally
Australia and New Zealand classify TB-500 as a prescription medicine. Many other countries treat it as an unapproved substance. Crossing borders with TB-500 carries customs risk.
Why this matters for research planning
Availability could change after the July 23, 2026 PCAC meeting. If a plan depends on compounding access, FDA decisions matter. If it depends on research suppliers, purity, customs, enforcement, and supplier reliability become the bigger risks.
TB-500 vs Thymosin Beta-4 vs BPC-157
TB-500 vs full-length Thymosin Beta-4
These are not the same molecule. TB-500 is a 7-amino-acid synthetic fragment (Ac-LKKTETQ, the 17-23 fragment of Tbeta-4). Full-length Tbeta-4 is a 43-amino-acid endogenous peptide. The fragment keeps the actin-binding motif but not the rest of the structure. Almost all human clinical evidence is on full-length Tbeta-4 (topical RGN-137 for ulcers, ophthalmic RGN-259 for ocular surface disease, IV synthetic Tbeta-4 for Phase 1 safety). Many research-use discussions treat them as interchangeable, but the evidence does not prove that.
TB-500 vs BPC-157
BPC-157 is a 15-amino-acid pentadecapeptide derived from a stable fragment of human gastric juice. TB-500 is a 7-amino-acid fragment of thymosin beta-4. Both have substantial preclinical animal-model evidence for tissue repair, but the proposed mechanisms are different: BPC-157 is associated with growth factor and angiogenic signaling; TB-500 is associated with actin-mediated cell migration. The two are commonly stacked in research-use cycles because the proposed mechanisms are described as complementary - this is a common community pattern, not a validated combined human protocol.
TB-500 vs full-length Tbeta-4 vs BPC-157 - quick comparison
Reference
Length
TB-500
7 amino acids
Thymosin beta-4 (full)
43 amino acids
BPC-157
15 amino acids
Reference
Source
TB-500
Synthetic fragment
Thymosin beta-4 (full)
Endogenous peptide
BPC-157
Synthetic, derived from gastric juice
Reference
Primary mechanism reference
TB-500
Actin binding (fragment)
Thymosin beta-4 (full)
Actin sequestration; broader signaling
BPC-157
Growth factor / angiogenic / cytoprotective signaling
Reference
Strongest human evidence
TB-500
None for the fragment specifically
Thymosin beta-4 (full)
Phase 2 wound, Phase 3 ocular (topical)
BPC-157
Small open-label and case series for joint pain
Reference
FDA status
TB-500
Not approved; PCAC review July 23 2026
Thymosin beta-4 (full)
Not approved; investigational in topical/ophthalmic formulations
BPC-157
Not approved; PCAC review July 23 2026
Reference
WADA status
TB-500
Prohibited (S0)
Thymosin beta-4 (full)
Prohibited (S0)
BPC-157
Prohibited (S0)
| Reference | TB-500 | Thymosin beta-4 (full) | BPC-157 |
|---|---|---|---|
| Length | 7 amino acids | 43 amino acids | 15 amino acids |
| Source | Synthetic fragment | Endogenous peptide | Synthetic, derived from gastric juice |
| Primary mechanism reference | Actin binding (fragment) | Actin sequestration; broader signaling | Growth factor / angiogenic / cytoprotective signaling |
| Strongest human evidence | None for the fragment specifically | Phase 2 wound, Phase 3 ocular (topical) | Small open-label and case series for joint pain |
| FDA status | Not approved; PCAC review July 23 2026 | Not approved; investigational in topical/ophthalmic formulations | Not approved; PCAC review July 23 2026 |
| WADA status | Prohibited (S0) | Prohibited (S0) | Prohibited (S0) |
Use this as a structural comparison. None of the three has an FDA-approved injectable human label.
The most common combined research-use plan pairs daily BPC-157 with twice-weekly (then weekly) TB-500. PDP covers the combined plan on the Wolverine stack page.
TB-500 Blood Tests & Monitoring
TB-500 is usually discussed in tissue-repair and connective-tissue research. Labs may help review broad health and inflammation context, but they do not directly prove tendon, ligament, or muscle repair.
Blood test markers to discuss with a clinician
Marker
CBC with differential
Why it matters
Screens blood-cell patterns that may flag infection, anemia, or immune context.
Timing
Baseline
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver, kidney, electrolyte, and glucose context in one broad panel.
Timing
Baseline
Marker
CRP
Why it matters
May help track systemic inflammation when injury or inflammatory symptoms are part of the picture.
Timing
Optional
Marker
ESR
Why it matters
Adds a slower-moving inflammation marker for chronic symptoms.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| CBC with differential | Screens blood-cell patterns that may flag infection, anemia, or immune context. | Baseline |
| Comprehensive metabolic panel (CMP) | Reviews liver, kidney, electrolyte, and glucose context in one broad panel. | Baseline |
| CRP | May help track systemic inflammation when injury or inflammatory symptoms are part of the picture. | Optional |
| ESR | Adds a slower-moving inflammation marker for chronic symptoms. | Optional |
Monitoring guidance is tissue-repair pathway-based because TB-500 lacks established human clinical monitoring standards.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with active injury, infection concern, immune disease, liver disease, kidney disease, or medication use.
Follow-up
Repeat broad markers after 6-12 weeks if symptoms change or inflammation tracking is part of the research context.
Longer term
For recurring injury protocols, review trends every 3-6 months with a clinician.
How to interpret the labs
- Local tissue response is often better evaluated by symptoms, function, exam, and imaging than by routine labs.
- Infection, clotting symptoms, and worsening injury signs should not be masked by normal labs.
- Avoid claiming that lab changes prove tissue regeneration.
Do not wait for routine labs
Severe swelling, fever, spreading redness, chest pain, shortness of breath, or one-sided leg swelling needs medical review.
FAQ
Q1: What is TB-500?
TB-500 is a synthetic 7-amino-acid fragment of thymosin beta-4, a larger peptide found throughout the body. Its sequence is Ac-LKKTETQ, which matches amino acids 17-23 of thymosin beta-4 (Tbeta-4). The fragment keeps the actin-binding region of the parent molecule but is not the same molecule as full-length Tbeta-4.
Q2: Is TB-500 the same as thymosin beta-4?
No. TB-500 is a 7-amino-acid synthetic fragment of the 43-amino-acid full-length thymosin beta-4. Most published human clinical evidence is on full-length Tbeta-4, not the TB-500 fragment. Many research-use discussions treat them as interchangeable, but the evidence does not prove that.
Q3: What is TB-500 commonly researched for?
TB-500 is most often referenced in research-use contexts focused on actin-mediated cell migration and tissue repair signaling. Preclinical animal work on the parent peptide thymosin beta-4 covers dermal wound healing, corneal injury, cardiac ischemia, and tendon/ligament repair models. Direct human clinical trials of the TB-500 fragment specifically are absent.
Q4: What is a typical TB-500 dosing pattern in research planning?
Community-referenced research planning frequently uses about 2 to 2.5 mg subcutaneous twice weekly during a 4-6 week loading phase, then about 2 to 2.5 mg once weekly for ongoing maintenance. These numbers are not validated by a human RCT of the TB-500 fragment, and they are not a personal dosing recommendation.
Q5: How is TB-500 reconstituted?
Most planners reconstitute a 10 mg vial with 2.0 mL of bacteriostatic water, which gives 5 mg/mL. On a U-100 insulin syringe, 1 unit equals 0.01 mL or about 50 mcg, and 50 units (0.5 mL) equals 2.5 mg. Add the BAC water slowly down the wall of the vial, swirl rather than shake, and refrigerate. Use the PepPal reconstitution calculator for other vial sizes.
Q6: How long is a typical TB-500 cycle?
Common research-use cycles run 4-12 weeks. The most-referenced structure is a 4-6 week loading phase at higher frequency followed by a maintenance phase at once-weekly dosing. There is no human RCT of TB-500 establishing an optimal cycle length.
Q7: Can BPC-157 and TB-500 be used together?
The BPC-157 + TB-500 combination - sometimes called the Wolverine stack - is the most common pairing in the research-use community because the proposed mechanisms are described as complementary. The combined research-use plan is detailed on the Wolverine stack page. Combined safety in humans is not established.
Q8: Is TB-500 FDA-approved?
No. TB-500 is not approved by the FDA for any human use. It was placed on Category 2 of the FDA's interim 503A bulks list in September 2023, removed from Category 2 on April 15, 2026 because nominators withdrew their nominations, and is scheduled for Pharmacy Compounding Advisory Committee review on July 23, 2026 for potential inclusion on the 503A Bulks List for wound healing. Reclassification away from Category 2 is not the same as FDA approval.
Q9: Is TB-500 banned in sport?
Yes. The World Anti-Doping Agency lists TB-500 and all thymosin beta-4 derivatives under Section S0 (Non-Approved Substances), at all times. Reported detection windows in urine and blood are around 30-45 days. NCAA, military, and most professional sport testing programs apply WADA-aligned rules. TB-500 is also prohibited in horse racing.
Q10: What are the main TB-500 side effects?
Direct human safety data on the TB-500 fragment is essentially absent. The closest reference is a Phase 1 study of full-length thymosin beta-4 at IV doses up to 1260 mg per day for 14 days in healthy volunteers, which reported no dose-limiting toxicities. Community-reported effects with subcutaneous TB-500 are mostly mild injection-site discomfort, short-lived fatigue, or head-pressure feelings. Theoretical concerns include effects on cancer angiogenesis and long-term immune modulation, neither of which has been characterized in humans.
Q11: Who should avoid TB-500 research?
Athletes subject to drug testing should avoid TB-500 because of the WADA prohibition. People with active or prior cancer, anyone pregnant or lactating, and anyone with allergies to peptide preparations or BAC-water preservatives should avoid it. People seeking treatment for a specific medical condition should work with a clinician through approved care pathways rather than a research peptide.
Q12: Is this medical advice?
No. This page is an educational research reference. It is not medical advice, diagnosis, or treatment guidance. TB-500 is a research peptide, not an approved medication.
Sources & Research
- 1. Ruff D, Crockford D, Girardi G, Zhang Y A randomized, placebo-controlled, single and multiple dose study of intravenous thymosin beta4 in healthy volunteers. Annals of the New York Academy of Sciences (2010)
- 2. Guarnera G, DeRosa A, Camerini R; 8 European sites The effect of thymosin treatment of venous ulcers. Annals of the New York Academy of Sciences (2010)
- 3. Malinda KM, Sidhu GS, Mani H, et al. Thymosin beta4 accelerates wound healing. Journal of Investigative Dermatology (1999)
- 4. Bock-Marquette I, Saxena A, White MD, DiMaio JM, Srivastava D Thymosin beta4 activates integrin-linked kinase and promotes cardiac cell migration, survival and cardiac repair. Nature (2004)
- 5. Kim S, Bhatt KH Thymosin beta4 enhances the healing of medial collateral ligament injury in rat. Regulatory Peptides (2013)
- 6. Sosne G, Dunn SP, Kim C Thymosin beta4 significantly improves signs and symptoms of severe dry eye in a phase 2 randomized trial. Cornea (2015)
- 7. Sosne G, Ousler GW, Kim K, Kang S, Yang J, Kleinman HK 0.1% RGN-259 (Thymosin beta4) Ophthalmic Solution Promotes Healing and Improves Comfort in Neurotrophic Keratopathy Patients in a Randomized, Placebo-Controlled, Double-Masked Phase III Clinical Trial. International Journal of Molecular Sciences (2023)
- 8. Goldstein AL, Hannappel E, Sosne G, Kleinman HK Thymosin beta4: A multi-functional regenerative peptide. Basic properties and clinical applications. Expert Opinion on Biological Therapy (2012)
- 9. Xue B, Robinson RC Progress on the Function and Application of Thymosin beta4. Frontiers in Endocrinology (2021)
- 10. World Anti-Doping Agency Investigation of in vitro/ex vivo TB-500 metabolism, synthesis of relevant metabolites and detection limits in urine and plasma. WADA Scientific Research (2017)
- 11. U.S. Food and Drug Administration Bulk Drug Substances Nominated for Use in Compounding Under Section 503A of the Federal Food, Drug, and Cosmetic Act. FDA (2026)
- 12. U.S. Food and Drug Administration July 23-24, 2026 Meeting of the Pharmacy Compounding Advisory Committee - Notice of Meeting. FDA Advisory Committee Calendar (2026)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page