BPC-157 Quick Start
BPC-157 stands for Body Protection Compound 157. It is a synthetic 15-amino-acid peptide derived from a sequence first identified in human gastric juice in the 1990s. Researchers most often study it in animal models of tendon, ligament, gut, and vessel injury.
BPC-157 research planning splits into two main formats. The most common is subcutaneous injection from a reconstituted vial. The peptide is also unusually stable in stomach acid for a peptide, so an oral capsule format exists and is sometimes used in gut-focused research planning. This page treats both formats as research-context references, not personal use guidance.
Routes studied
SubQ injection is most common; oral, IM, and IV have all appeared in published research.
Schedule shape
Typical published research planning splits a daily total into one or two doses.
Measurement
Use vial concentration math and U-100 insulin syringe units for injectable format.
Supplies basics
BAC water, U-100 insulin syringes, alcohol swabs, and a refrigerated storage spot.
Research status
Mostly preclinical evidence; not FDA-approved as of June 2026.
Disclaimer
This page is an educational research reference and is not medical advice. It does not diagnose, treat, or prescribe. Speak with a licensed clinician before starting any peptide protocol.
Use this page for dose steps, vial mixing, timing, and supplies. For the bigger research picture, read the BPC-157 research guide on how it works, key studies, safety notes, and common comparisons.
BPC-157 Dosing Protocol & Schedule
BPC-157 has been studied in two main research formats. Choose the tab that matches the format being researched. The numbers shown are research-planning ranges drawn from published preclinical protocols and community-derived references, not personal medical recommendations.
BPC-157 Protocol Formats
Choose the format you are researching to see route-specific notes.
Reconstituted lyophilized vial, drawn into a U-100 insulin syringe.
Subcutaneous injection is the most commonly referenced research format. The peptide pharmacokinetics paper by He et al. (Frontiers in Pharmacology, 2022) reports a half-life under 30 minutes after IM or IV administration in rodent and dog models, which is why split-dose schedules appear in the literature.
Common research-planning ranges (subcutaneous)
Planning band
Low
Per-dose range
~250 mcg
Frequency
Once daily
Typical context
Maintenance / general research planning
Planning band
Standard
Per-dose range
~250 mcg
Frequency
Twice daily
Typical context
Most published preclinical protocols and community references
Planning band
High
Per-dose range
~500 mcg
Frequency
Twice daily
Typical context
Short-term acute-injury research planning
| Planning band | Per-dose range | Frequency | Typical context |
|---|---|---|---|
| Low | ~250 mcg | Once daily | Maintenance / general research planning |
| Standard | ~250 mcg | Twice daily | Most published preclinical protocols and community references |
| High | ~500 mcg | Twice daily | Short-term acute-injury research planning |
These ranges reflect community-derived research planning. Direct human dose-finding trials are limited; a 2025 IV pilot in two adults used 10 mg and 20 mg single infusions and reported no adverse effects (Lee et al., Alternative Therapies in Health and Medicine). This is not a dosing recommendation.
Cycle Guidelines
Approach
Standard
Duration
4-6 weeks
Review point
Week 4
Best for
General research planning
Approach
Extended
Duration
6-8 weeks
Review point
Week 6
Best for
Stubborn-injury research models
Approach
Long
Duration
8-12 weeks
Review point
Week 8
Best for
Slow-remodeling tissue research planning
| Approach | Duration | Review point | Best for |
|---|---|---|---|
| Standard | 4-6 weeks | Week 4 | General research planning |
| Extended | 6-8 weeks | Week 6 | Stubborn-injury research models |
| Long | 8-12 weeks | Week 8 | Slow-remodeling tissue research planning |
Off periods of 2-4 weeks between cycles are common in research planning. There is no published human cycling RCT.
Oral or capsule format. BPC-157 is unusually stable in human gastric juice.
Sikiric et al. (Current Pharmaceutical Design, 2011) reported that BPC-157 remains stable in human gastric juice for more than 24 hours, which is unusual for a peptide. This is the basis for oral and capsule research formats, especially in gut-focused models.
Oral research-planning ranges are usually higher than the subcutaneous ranges to account for lower absorption across the gut lining. Published preclinical work used a wide range of oral doses; community-derived planning often references ~250-500 mcg once or twice daily. Direct human oral dose-finding trials are limited. This is not a dosing recommendation.
Format note
Capsule products are commercial supplements, not FDA-approved drugs. Capsule potency depends on the manufacturer and is not standardized. Verify any product against a third-party Certificate of Analysis.
Evidence boundary
BPC-157 has no published human Phase 2 or Phase 3 dose-finding trial. Reported research-planning ranges are derived from animal protocols and community usage. Use this page as research context, not as a treatment plan.
BPC-157 Supplies Needed
Affiliate disclosure: PDP may earn a commission when you use eligible supplier links, at no extra cost to you. The numbers below assume the standard research-planning band of about 250 mcg twice daily from 10 mg vials reconstituted with 2 mL bacteriostatic water.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

BPC-157 Supply

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials
Math assumes 10 mg vials reconstituted with 2 mL BAC water (concentration 5,000 mcg/mL). At 250 mcg twice daily, one 10 mg vial covers roughly 20 days.
| Cycle length | Planning note |
|---|---|
4 weeks 2 x 10 mg vials | 56 doses needed at 250 mcg 2x/day; round up for priming losses. |
6-8 weeks 3 x 10 mg vials | 6 weeks: 84 doses needed; three vials cover 120 doses before losses.; 8 weeks: 112 doses needed; three vials gives a small margin. |
12 weeks 5 x 10 mg vials | 168 doses needed; build in margin for storage limits. |
4 weeks
2 x 10 mg vials
56 doses needed at 250 mcg 2x/day; round up for priming losses.
6-8 weeks
3 x 10 mg vials
6 weeks: 84 doses needed; three vials cover 120 doses before losses.; 8 weeks: 112 doses needed; three vials gives a small margin.
12 weeks
5 x 10 mg vials
168 doses needed; build in margin for storage limits.
Insulin Syringes (U-100)
Use 0.3 mL / 30-unit syringes for small daily draws. At 5,000 mcg/mL, 250 mcg = 0.05 mL = 5 units.
| Cycle length | Planning note |
|---|---|
4 weeks 56 syringes | 1 syringe per injection; recommend 1 x 100-count box. |
6 weeks 84 syringes | 1 syringe per injection; recommend 1 x 100-count box. |
8 weeks 112 syringes | Recommend 2 x 100-count boxes. |
12 weeks 168 syringes | Recommend 2 x 100-count boxes. |
4 weeks
56 syringes
1 syringe per injection; recommend 1 x 100-count box.
6 weeks
84 syringes
1 syringe per injection; recommend 1 x 100-count box.
8 weeks
112 syringes
Recommend 2 x 100-count boxes.
12 weeks
168 syringes
Recommend 2 x 100-count boxes.
Bacteriostatic Water
2 mL BAC water per vial. 10 mL bottles are standard; once opened, follow supplier beyond-use guidance.
| Cycle length | Planning note |
|---|---|
4-12 weeks 1 x 10 mL bottle | 4 weeks: 2 vials use 4 mL total; one bottle gives margin.; 6 weeks: 3 vials use 6 mL total; one bottle gives margin.; 8 weeks: 3 vials use 6 mL total; one bottle gives margin.; 12 weeks: 5 vials use 10 mL total. |
4-12 weeks
1 x 10 mL bottle
4 weeks: 2 vials use 4 mL total; one bottle gives margin.; 6 weeks: 3 vials use 6 mL total; one bottle gives margin.; 8 weeks: 3 vials use 6 mL total; one bottle gives margin.; 12 weeks: 5 vials use 10 mL total.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments. Math assumes 10 mg vials reconstituted with 2 mL BAC water unless otherwise noted.
Companion Supplies & Routine Support
BPC-157 Reconstitution Guide
BPC-157 ships as a freeze-dried (lyophilized) powder. Reconstitution mixes that powder with bacteriostatic water (BAC water) to create an injectable solution. The amount of BAC water added sets the final concentration, which sets the draw volume per dose.
10 mg Vial Reconstitution
BAC water added
2 mL
Concentration
5,000 mcg/mL
250 mcg dose volume
0.05 mL = 5 units
500 mcg dose volume
0.10 mL = 10 units
Doses per vial at 250 mcg
40
BAC water added
3 mL
Concentration
3,333 mcg/mL
250 mcg dose volume
0.075 mL = ~7.5 units
500 mcg dose volume
0.15 mL = 15 units
Doses per vial at 250 mcg
40
| BAC water added | Concentration | 250 mcg dose volume | 500 mcg dose volume | Doses per vial at 250 mcg |
|---|---|---|---|---|
| 2 mL | 5,000 mcg/mL | 0.05 mL = 5 units | 0.10 mL = 10 units | 40 |
| 3 mL | 3,333 mcg/mL | 0.075 mL = ~7.5 units | 0.15 mL = 15 units | 40 |
Units shown are U-100 insulin syringe units (where 100 units = 1.0 mL). The 2 mL option is the default assumption used throughout this page; larger volumes make small draws easier to read.
- 01
Inspect the vial
Check the label, expected milligram amount, and that the powder looks dry and intact before opening.
- 02
Wipe the stopper
Use an alcohol swab on the rubber stopper of both the BAC water and the peptide vial.
- 03
Draw BAC water
Use a U-100 insulin syringe to draw 2 mL BAC water for the default 10 mg vial setup, usually across two draws.
- 04
Inject down the wall
Insert the needle into the peptide vial and slowly release the BAC water down the inside wall, not directly onto the powder.
- 05
Swirl, do not shake
Roll the vial gently between your palms until the solution looks clear. Shaking can damage the peptide.
- 06
Verify clarity
The solution should be clear and colorless. Cloudy or particulate solutions should not be used.
- 07
Refrigerate
Store reconstituted BPC-157 at refrigerator temperature (35.6-46.4F / 2-8C). Do not freeze the reconstituted solution.
Calculator
Use a research-context reconstitution calculator to confirm draw volumes any time you change vial size or BAC water volume. Always confirm against the supplier label.
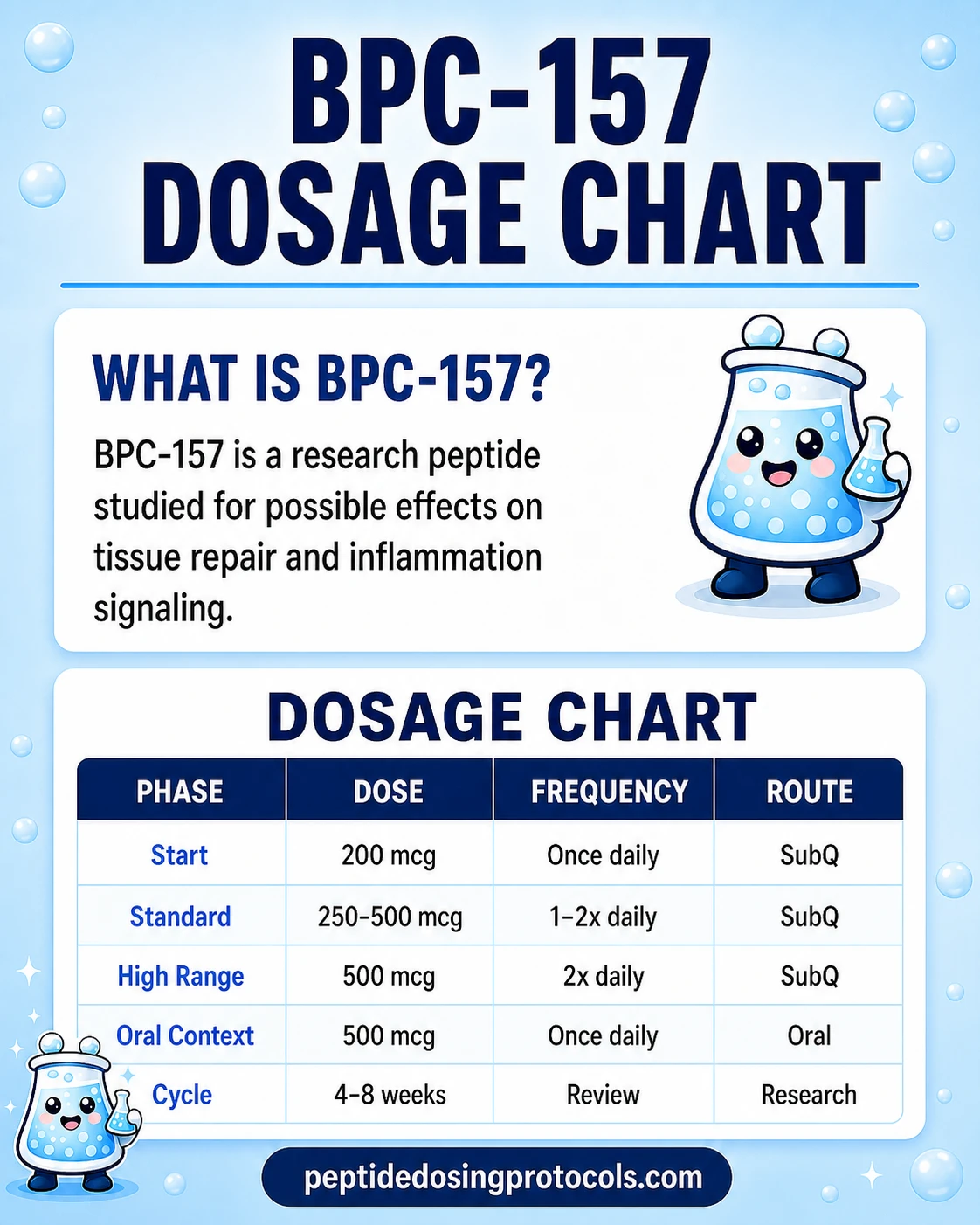
BPC-157 Dosage Chart
This BPC-157 dosage chart summarizes common community-derived research-planning ranges from ~250 mcg once daily up to ~500 mcg twice daily, with route and context shown side by side.
How BPC-157 Works
In plain English, animal studies suggest BPC-157 helps damaged tissue grow new blood supply and signals cells to migrate into injured areas. This makes it a recurring research tool for tendon, gut, and vessel-injury models. The technical details follow.
BPC-157 has been reported to upregulate VEGFR2 (vascular endothelial growth factor receptor 2) and activate the Akt-eNOS pathway, which raises nitric oxide production in blood-vessel walls (Hsieh et al., Journal of Molecular Medicine, 2017; Hsieh et al., Scientific Reports, 2020). The downstream effect is more dilated vessels and improved local blood flow in injury models.
Other reported mechanisms include activation of FAK-paxillin complexes (which help cells migrate and attach to surfaces during wound healing), JAK-2 signaling, and ERK1/2 pathway activity (Sikiric et al., Current Neuropharmacology, 2016; Vukojevic et al., Neural Regeneration Research, 2022). These are preclinical findings, not human clinical proofs.
Angiogenesis
Promotes new blood vessel formation in animal models. This is the central mechanism most reviews focus on.
Cell migration
Reported to support fibroblast and endothelial cell migration into injured tissue.
Inflammation balance
Animal data report downregulation of NF-kB and Nos2 in injury settings.
Open question
Whether the same mechanisms are clinically meaningful in humans is not yet established.
Who BPC-157 Is For and Who Should Avoid It
Because BPC-157 is not FDA-approved and human safety data is limited, eligibility decisions should always involve a licensed clinician. The points below summarize categories where caution is most consistently flagged in reviews and regulator notices.
Active or prior cancer
BPC-157 promotes angiogenesis in animal models. Because tumor growth also depends on new blood vessels, several reviews describe this as a theoretical concern that has not been resolved in humans (Sehgal et al., Pharmaceuticals, 2025).
Pregnancy and lactation
No published human reproductive or lactation safety data exists.
Competitive or tested athletes
BPC-157 has been on the World Anti-Doping Agency Prohibited List under category S0 since 2022 and remains on the 2025 list. Use of BPC-157 will result in an anti-doping rule violation.
Anyone on blood-pressure-active medications
BPC-157 affects nitric oxide signaling in animal models. Anyone on medications that act on nitric oxide or vascular tone should review with a clinician.
Anyone seeking a regulated medical treatment
BPC-157 is not an FDA-approved drug. As of April 22, 2026, it was removed from FDA Category 2, but the FDA's Pharmacy Compounding Advisory Committee will not consider it for the 503A bulks list until the July 23, 2026 meeting.
BPC-157 Side Effects & Safety
Reported side effects fall into three buckets: directly observed effects in pilot studies, theoretical risks based on mechanism, and route-specific issues.
Observed in pilot human work
A 2025 IV infusion pilot of BPC-157 in two adults at 10 mg and 20 mg reported no adverse effects on cardiac, hepatic, renal, thyroid, or glucose biomarkers (Lee et al., Alternative Therapies in Health and Medicine, 2025). A 2024 pilot in interstitial cystitis and a 2021 case series in knee pain reported it as well-tolerated within those small samples.
Theoretical mechanism risk
The same pathway that supports tissue repair (angiogenesis) also supports tumor growth. Reviews flag this as an unresolved question, especially in patients with current or prior cancer (Sehgal et al., Pharmaceuticals, 2025).
Injection-site reactions
Mild redness or small bumps at the injection site are the most commonly reported short-term issues in community usage. Site rotation is the standard answer.
Blood pressure
BPC-157 affects nitric oxide signaling, which influences vessel tone. Anyone monitoring blood pressure should track readings during a research cycle.
Quality control risk
Most BPC-157 sold in the U.S. is research-use grey-market material. Contamination, mis-dosing, and degradation are real practical risks separate from the molecule itself.
BPC-157 Timeline & What to Monitor
Most preclinical work measures injury-model endpoints over days to weeks rather than longer windows. Human pilot studies have measured short-term symptom reports and basic safety labs; they have not measured long-term outcomes.
Timeline reference points (research planning)
Timeframe
Days 1-7
Commonly tracked
Acute pain reports, injection-site response
Notes
Anti-doping rule violation begins immediately for tested athletes.
Timeframe
Weeks 1-2
Commonly tracked
Range-of-motion and functional self-report in case series
Notes
Reflects symptom-level changes, not structural healing.
Timeframe
Weeks 4-6
Commonly tracked
Tendon and ligament endpoints in animal models
Notes
Rodent tendon papers commonly assess at this window.
Timeframe
Weeks 6-12
Commonly tracked
Extended-cycle community reports
Notes
No human RCT covers this duration.
| Timeframe | Commonly tracked | Notes |
|---|---|---|
| Days 1-7 | Acute pain reports, injection-site response | Anti-doping rule violation begins immediately for tested athletes. |
| Weeks 1-2 | Range-of-motion and functional self-report in case series | Reflects symptom-level changes, not structural healing. |
| Weeks 4-6 | Tendon and ligament endpoints in animal models | Rodent tendon papers commonly assess at this window. |
| Weeks 6-12 | Extended-cycle community reports | No human RCT covers this duration. |
These reference points come from preclinical literature and small pilots. They are not predictions of personal outcomes.
Reasonable markers to track during a research cycle include a basic metabolic panel, complete blood count, and blood pressure. None of these is a peptide-specific test. The 2025 IV pilot measured cardiac, hepatic, renal, thyroid, and glucose biomarkers and reported no abnormalities (Lee et al., 2025), which gives a sense of what those investigators considered worth checking.
BPC-157 Clinical Evidence Context
Direct human evidence for BPC-157 is limited to a small number of pilot studies. Animal evidence is much larger and has been the basis for almost all of the published mechanism work.
Human pilot evidence
Three small pilots: a 12-patient knee-pain case series (Lee & Padgett, Alternative Therapies in Health and Medicine, 2021); a 12-woman interstitial cystitis pilot (Lee, Walker & Ayadi, 2024); and a two-adult IV safety pilot at 10 mg and 20 mg (Lee, Walker & Ayadi, 2025). Combined sample size is roughly 30 patients.
Systematic review (sports medicine)
Vasireddi et al. published a 2025 systematic review on BPC-157 in orthopedic sports medicine (HSS Journal). It concluded that human evidence remains insufficient to support clinical recommendations.
Mechanism literature
Multiple peer-reviewed papers describe VEGFR2 activation, eNOS/NO signaling, and tendon-cell behavior in cultured cells and rodent models (Chang et al., Journal of Applied Physiology, 2011; Hsieh et al., 2017; Hsieh et al., 2020).
Pharmacokinetics
He et al. (Frontiers in Pharmacology, 2022) reported pharmacokinetics and tissue distribution in rats and dogs, including a rapid plasma half-life under 30 minutes after IM or IV dosing.
Regulatory toxicology
Xu et al. (Regulatory Toxicology and Pharmacology, 2020) reported a preclinical safety package designed to support potential drug development.
Open question
No published Phase 2 or Phase 3 human RCT exists. The community-derived planning ranges should not be read as clinically validated doses.
BPC-157 Storage & Handling
Storage Reference
State
Lyophilized (powder form)
Storage
-4F (-20C) long-term; refrigerator short-term
Notes
Follow supplier label; powder is more stable than reconstituted solution.
State
Reconstituted (liquid form)
Storage
35.6-46.4F (2-8C)
Notes
Use within roughly 3-4 weeks per common community planning. Do not freeze the reconstituted vial.
State
Appearance after recon
Storage
Clear, colorless solution
Notes
Cloudy or particulate solutions should not be used.
| State | Storage | Notes |
|---|---|---|
| Lyophilized (powder form) | -4F (-20C) long-term; refrigerator short-term | Follow supplier label; powder is more stable than reconstituted solution. |
| Reconstituted (liquid form) | 35.6-46.4F (2-8C) | Use within roughly 3-4 weeks per common community planning. Do not freeze the reconstituted vial. |
| Appearance after recon | Clear, colorless solution | Cloudy or particulate solutions should not be used. |
Always defer to the specific supplier label and any beyond-use information they publish.
BPC-157 Protocol Mistakes & Troubleshooting
- 01
Cloudy vial after reconstitution
Do not use it. Cloudiness can mean contamination, agitation damage, or product issues. Discard and replace.
- 02
Wrong BAC water volume
Check the actual concentration on the supplier label and recalculate dose volume before drawing. The published vial math on this page assumes 10 mg vials.
- 03
Missed scheduled dose
Skip and continue at the next scheduled time. Do not double-dose.
- 04
Persistent injection-site reaction
Rotate sites within and between abdomen quadrants. Use a fresh syringe and swab every session. Persistent or expanding reactions warrant clinician review.
- 05
Storage mistake (left out overnight)
Treat as compromised and discard. Reconstituted peptides are not designed for room-temperature storage.
- 06
Confused about route
If you are unsure whether to use injectable or oral material, stop and review the supplier label. Capsules and reconstituted vials are not interchangeable on a milligram-for-milligram basis.
- 07
Severe or unexplained symptoms
Stop the protocol and seek qualified medical care. This page cannot replace clinician evaluation.
BPC-157 Regulatory Status
BPC-157 is not an FDA-approved drug for any indication. As of June 2026, the regulatory picture has three moving parts.
FDA 503A Category 2 (April 2026)
On April 15, 2026, the FDA published a 503A bulks list update. Effective April 22, 2026, BPC-157 was removed from Category 2 (the bulks substances list flagged as raising significant safety concerns). The reason given was withdrawal of the original Category 2 nominations, not a positive safety determination.
PCAC review (July 2026)
The FDA stated it intends to consult the Pharmacy Compounding Advisory Committee on July 23, 2026 regarding inclusion of BPC-157 acetate and BPC-157 (free base) on the 503A bulks list. Removal from Category 2 is not the same as listing on 503A.
WADA prohibited substance
BPC-157 has been on the World Anti-Doping Agency Prohibited List under category S0 (non-approved substances) since 2022 and remains on the 2025 list.
International scheduling
Australia's Therapeutic Goods Administration (interim decision, April 2024) and New Zealand's Medsafe (Medicines Classification Committee, June 2025) have moved to schedule BPC-157 as a prescription-only medicine, despite its unavailability through legitimate prescription.
Branded approval status
There is no FDA-approved branded BPC-157 product. Compounded preparations are not the same as FDA-approved drugs.
BPC-157 vs TB-500 vs Wolverine Stack
Search demand consistently pairs BPC-157 with TB-500 and the informal Wolverine stack. The compounds are not interchangeable.
Compound Comparison
Feature
Class
BPC-157
15-amino-acid synthetic pentadecapeptide
TB-500
Synthetic 17-amino-acid Thymosin Beta-4 fragment
Feature
Common research focus
BPC-157
Tendon, gut, vessel models; gut-stable for oral research
TB-500
Cell migration; soft-tissue and muscle models
Feature
Most common research route
BPC-157
SubQ; oral capsules also used
TB-500
SubQ; longer dose intervals than BPC-157
Feature
Half-life pattern
BPC-157
Short plasma half-life (<30 min) in animal PK studies
TB-500
Longer signaling-relevant action; less frequent dosing
Feature
Combined references
BPC-157
Often paired with TB-500 in community planning ('Wolverine stack')
TB-500
Same pairing
Feature
Regulatory status
BPC-157
Removed from FDA Category 2 April 22, 2026; not approved
TB-500
Also removed from FDA Category 2 April 22, 2026; not approved
| Feature | BPC-157 | TB-500 |
|---|---|---|
| Class | 15-amino-acid synthetic pentadecapeptide | Synthetic 17-amino-acid Thymosin Beta-4 fragment |
| Common research focus | Tendon, gut, vessel models; gut-stable for oral research | Cell migration; soft-tissue and muscle models |
| Most common research route | SubQ; oral capsules also used | SubQ; longer dose intervals than BPC-157 |
| Half-life pattern | Short plasma half-life (<30 min) in animal PK studies | Longer signaling-relevant action; less frequent dosing |
| Combined references | Often paired with TB-500 in community planning ('Wolverine stack') | Same pairing |
| Regulatory status | Removed from FDA Category 2 April 22, 2026; not approved | Also removed from FDA Category 2 April 22, 2026; not approved |
For the combined research planning context, see the Wolverine Stack guide.
BPC-157 Blood Tests & Monitoring
BPC-157 is usually discussed for tissue repair, gut, tendon, and injury research. Labs may help review general health, but they do not directly prove local tissue healing.
Blood test markers to discuss with a clinician
Marker
CBC with differential
Why it matters
Screens blood-cell patterns that may flag infection, anemia, or immune changes before interpreting repair symptoms.
Timing
Baseline
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver enzymes, kidney markers, electrolytes, and glucose in one broad safety panel.
Timing
Baseline
Marker
CRP
Why it matters
May help track broader inflammation when injury, gut symptoms, or systemic inflammation are part of the picture.
Timing
Optional
Marker
ESR
Why it matters
Adds a slower-moving inflammation marker that may be useful when symptoms are chronic.
Timing
Optional
Marker
Urinalysis
Why it matters
Can add basic kidney and hydration context when there are urinary symptoms or kidney concerns.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| CBC with differential | Screens blood-cell patterns that may flag infection, anemia, or immune changes before interpreting repair symptoms. | Baseline |
| Comprehensive metabolic panel (CMP) | Reviews liver enzymes, kidney markers, electrolytes, and glucose in one broad safety panel. | Baseline |
| CRP | May help track broader inflammation when injury, gut symptoms, or systemic inflammation are part of the picture. | Optional |
| ESR | Adds a slower-moving inflammation marker that may be useful when symptoms are chronic. | Optional |
| Urinalysis | Can add basic kidney and hydration context when there are urinary symptoms or kidney concerns. | Optional |
Monitoring guidance is pathway-based because BPC-157 lacks established human clinical lab-monitoring standards.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially if there is active injury, gut symptoms, infection concern, liver disease, kidney disease, or medication use.
Follow-up
Repeat broad markers after 6-12 weeks if symptoms change, inflammation is part of the context, or the protocol continues.
Longer term
For recurring injury protocols, review trends every 3-6 months with a clinician.
How to interpret the labs
- Routine labs may look normal even when a tendon, ligament, or gut issue is still present.
- Medication use, infection risk, imaging, and physical exam findings matter more than labs alone.
- Avoid presenting symptom improvement as proof of tissue regeneration.
Do not wait for routine labs
Fever, spreading redness, severe wound pain, or drainage needs medical review. Sudden chest pain, shortness of breath, or one-sided leg swelling should not be treated as routine soreness.
FAQ
Q1: What is BPC-157?
BPC-157 is a synthetic 15-amino-acid peptide. The sequence was identified from a protein found in human gastric juice in the 1990s. It is most often studied in animal models of tendon, gut, and vessel injury, and is not an FDA-approved drug.
Q2: What does BPC-157 do?
In animal studies, BPC-157 supports new blood vessel growth, helps cells migrate into injury sites, and balances inflammation. The most consistently reported pathway involves VEGFR2 and the Akt-eNOS nitric oxide cascade. Translation to humans has not been confirmed in large clinical trials.
Q3: Is BPC-157 FDA-approved?
No. BPC-157 is not an FDA-approved drug. On April 15, 2026, the FDA announced the removal of BPC-157 from its 503A Category 2 list, effective April 22, 2026, because the original nominations were withdrawn. The Pharmacy Compounding Advisory Committee is scheduled to review BPC-157 on July 23, 2026 for possible inclusion on the 503A bulks list.
Q4: Why is BPC-157 banned by WADA?
The World Anti-Doping Agency added BPC-157 to its Prohibited List under category S0 (non-approved substances) in 2022. WADA bans substances that lack regulatory approval for human use even if they are not specifically performance-enhancing. BPC-157 remains on the 2025 Prohibited List.
Q5: How is BPC-157 commonly dosed in research planning?
Published preclinical protocols and community-derived references typically use about 250 mcg once or twice daily by subcutaneous injection. A higher band of about 500 mcg twice daily appears in short-term acute-injury research planning. These ranges are research planning, not personal dosing recommendations, and no published human Phase 2 or Phase 3 dose-finding trial exists.
Q6: Can BPC-157 be taken orally?
Yes, in research-context terms. BPC-157 is unusually stable in human gastric juice for a peptide, which is why oral and capsule formats appear in research planning, especially for gut models. Oral research-planning amounts are usually higher than subcutaneous amounts to account for absorption differences. Capsule products are commercial supplements, not FDA-approved drugs.
Q7: How is BPC-157 reconstituted?
A 10 mg vial reconstituted with 2 mL bacteriostatic water yields 5,000 mcg/mL. At that concentration, 250 mcg equals 0.05 mL, or 5 units on a U-100 insulin syringe. A 500 mcg draw equals 0.10 mL, or 10 units. Always confirm against the supplier label.
Q8: What are the main side effects of BPC-157?
Most commonly reported short-term effects are injection-site redness or small bumps. Theoretical concerns include angiogenesis-related risk in patients with current or prior cancer, and effects on nitric oxide signaling that could matter for blood pressure. Severe adverse events have not been a pattern in community usage, but human safety data is limited to a few pilot studies.
Q9: Is BPC-157 dangerous?
Pilot human studies have reported BPC-157 as well-tolerated in small samples, and large adverse-event signals have not appeared in community usage. The honest summary is that long-term human safety data is missing and the angiogenesis mechanism is an unresolved theoretical concern. Quality control of grey-market material is also a real practical risk, separate from the molecule itself.
Q10: How does BPC-157 compare to TB-500?
BPC-157 is a 15-amino-acid pentadecapeptide most often studied in tendon, gut, and vessel models. TB-500 is a synthetic fragment of Thymosin Beta-4, more often studied in cell-migration and soft-tissue models. They are sometimes referenced together in informal 'Wolverine stack' planning. They are not interchangeable. See the Wolverine Stack guide for combined research-planning context.
Q11: How long is a typical BPC-157 research cycle?
Community-derived planning most often references 4-6 week cycles, with extended 6-8 or 8-12 week cycles for slower-remodeling tissue research models. Off periods of 2-4 weeks between cycles are common. There is no published human cycling RCT, so these durations are research-planning conventions rather than clinically validated regimens.
Q12: Is this BPC-157 page medical advice?
No. This page is an educational research reference. It does not diagnose, treat, or prescribe. Speak with a licensed clinician before starting any peptide protocol, and review the regulatory status section before assuming legal availability.
Sources & Research
- 1. Chang CH, Tsai WC, Lin MS, Hsu YH, Pang JH The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. Journal of Applied Physiology (2011)
- 2. Hsieh MJ, Liu HT, Wang CN, et al. Therapeutic potential of pro-angiogenic BPC157 is associated with VEGFR2 activation and up-regulation. Journal of Molecular Medicine (2017)
- 3. Hsieh MJ, Lee CH, Chueh HY, et al. Modulatory effects of BPC 157 on vasomotor tone and the Src-Cav-1-eNOS signaling pathway in rats. Scientific Reports (2020)
- 4. He L, Feng D, Guo H, et al. Pharmacokinetics, distribution, metabolism, and excretion of body-protective compound 157 in rats and dogs. Frontiers in Pharmacology (2022)
- 5. Sikiric P, Seiwerth S, Rucman R, et al. Stable gastric pentadecapeptide BPC 157: novel therapy in gastrointestinal tract. Current Pharmaceutical Design (2011)
- 6. Vukojevic J, Milavic M, Perovic D, et al. Pentadecapeptide BPC 157 and the central nervous system. Neural Regeneration Research (2022)
- 7. Vasireddi N, Hahamyan H, Salata MJ, et al. Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. HSS Journal (2025)
- 8. Lee E, Padgett B Intra-Articular Injection of BPC 157 for Multiple Types of Knee Pain. Alternative Therapies in Health and Medicine (2021)
- 9. Lee E, Walker C, Ayadi B Effect of BPC-157 on Symptoms in Patients with Interstitial Cystitis: A Pilot Study. Alternative Therapies in Health and Medicine (2024)
- 10. Lee E, Walker C, Ayadi B Safety of Intravenous Infusion of BPC157 in Humans: A Pilot Study. Alternative Therapies in Health and Medicine (2025)
- 11. Xu C, Sun L, Ren F, et al. Preclinical safety evaluation of body protective compound-157, a potential drug for treating various wounds. Regulatory Toxicology and Pharmacology (2020)
- 12. Sehgal P, Gupta R, Choudhary K, Singh R BPC 157: A Promising Candidate for Cytoprotection and Tissue Repair. Pharmaceuticals (2025)
- 13. U.S. Food and Drug Administration Updated 503A bulk drug substances list (Category 2 revision, effective April 22, 2026). FDA.gov (2026)
- 14. World Anti-Doping Agency World Anti-Doping Code International Standard Prohibited List 2025. WADA (2025)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page