Tesofensine Quick Start
Tesofensine is an oral tablet first developed for Parkinson's and Alzheimer's disease. In those early trials, people lost weight without trying. That finding shifted the program toward obesity.
It works in the brain by blocking the reuptake of three signaling chemicals: dopamine, norepinephrine, and serotonin. Blocking reuptake means more of each signal stays active in the gap between brain cells. The practical result studied in trials is lower appetite and a small bump in resting energy use.
This page is a research reference for the doses studied in trials. It is not a treatment plan. It is also not a recommendation to take tesofensine.
Route
Oral tablet, taken once daily. No injection. No reconstitution.
Doses studied
0.25 mg and 0.5 mg once daily were the main doses in Phase 2 and Phase 3.
Half-life
About 9 days, so the drug builds up over the first 4-6 weeks before levels stabilize.
Cycle in trials
24-week treatment periods in both Phase 2 (Astrup 2008) and the Mexican Phase 3 study.
Status
Not FDA approved in the US as of June 2026. Investigational only.
Educational reference, not medical advice
Tesofensine is not FDA approved. This guide reports what was studied in published trials. It is not a dosing recommendation, not a prescription, and not a personal protocol.
Tesofensine Dosing Protocol & Schedule
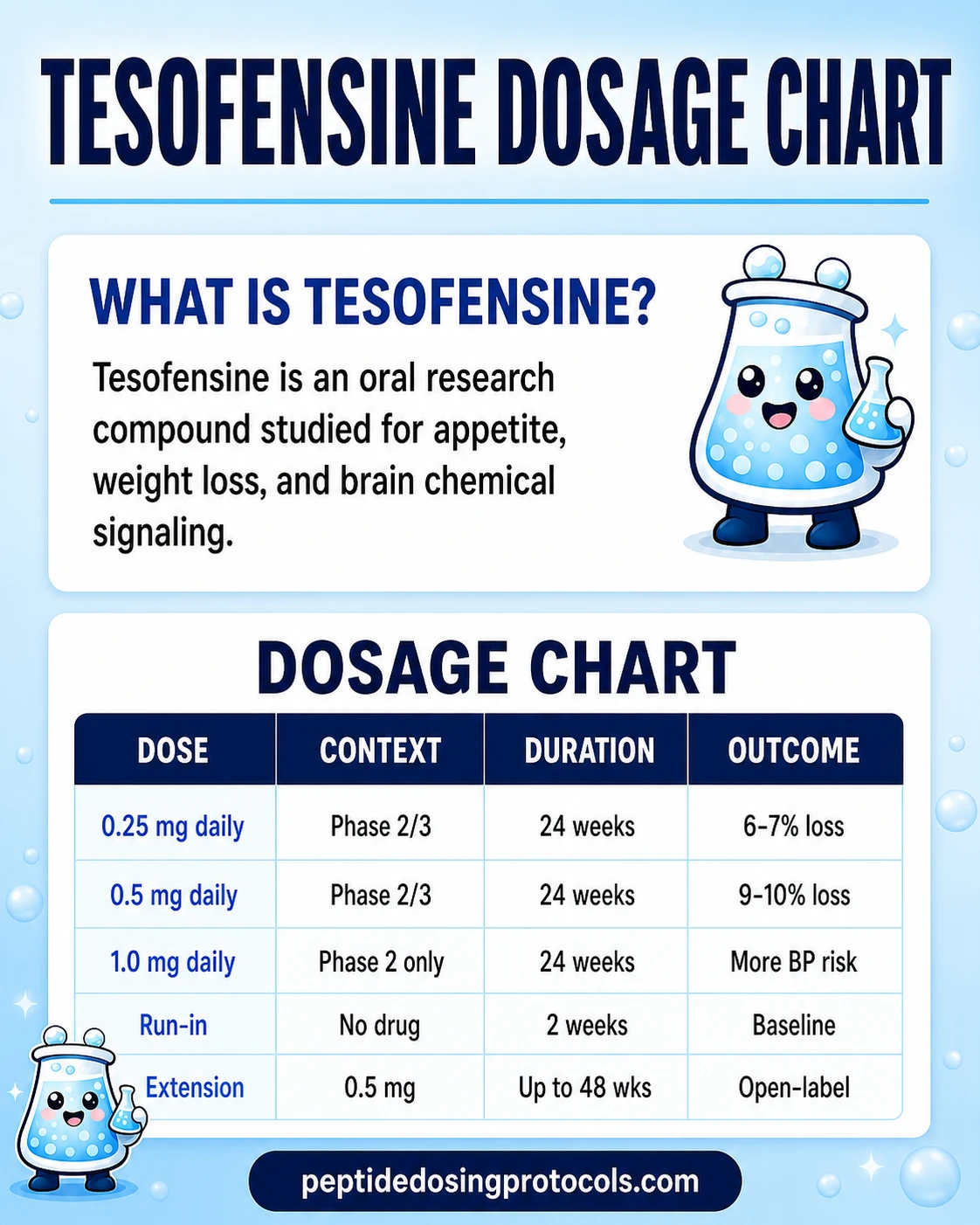
The two doses studied most often are 0.25 mg and 0.5 mg, taken as a single oral tablet once a day. A 1.0 mg dose was tested in the original Phase 2 trial but was associated with higher blood pressure and a higher dropout rate. The Phase 3 program in Mexico dropped 1.0 mg and only tested 0.25 mg and 0.5 mg.
In the Astrup 2008 Phase 2 study, patients took the tablet once daily for 24 weeks alongside a calorie-restricted diet. The 0.5 mg arm showed a placebo-subtracted weight loss of about 9.2% (around 9.1 kg). The 0.25 mg arm showed about 6.5%. Placebo lost about 2.0%. This is not a dosing recommendation.
Why dose timing matters less than people think
Tesofensine has a half-life of about 9 days. That means a single tablet does not really wear off between doses the way a short-acting drug would. Blood levels build up slowly over the first 4-6 weeks. After that the body reaches steady state, where the amount taken each day matches what is cleared each day.
In practice, trial protocols still asked patients to take the tablet in the morning. The reason is simple: the drug raises norepinephrine and dopamine, which can disrupt sleep. Morning dosing kept the highest signal during the day. This is not a dosing recommendation.
Doses studied in tesofensine clinical trials
Dose
0.25 mg daily
Trial context
Phase 2 (Astrup 2008) and Phase 3 (Mexico)
Duration
24 weeks
Outcome reported
About 6-7% placebo-subtracted weight loss
Dose
0.5 mg daily
Trial context
Phase 2 (Astrup 2008) and Phase 3 (Mexico)
Duration
24 weeks
Outcome reported
About 9-10% placebo-subtracted weight loss
Dose
1.0 mg daily
Trial context
Phase 2 only (Astrup 2008)
Duration
24 weeks
Outcome reported
Highest weight loss but more blood pressure issues and dropouts; dropped from later trials
| Dose | Trial context | Duration | Outcome reported |
|---|---|---|---|
| 0.25 mg daily | Phase 2 (Astrup 2008) and Phase 3 (Mexico) | 24 weeks | About 6-7% placebo-subtracted weight loss |
| 0.5 mg daily | Phase 2 (Astrup 2008) and Phase 3 (Mexico) | 24 weeks | About 9-10% placebo-subtracted weight loss |
| 1.0 mg daily | Phase 2 only (Astrup 2008) | 24 weeks | Highest weight loss but more blood pressure issues and dropouts; dropped from later trials |
These are trial endpoints, not a dosing plan. The 1.0 mg dose was not advanced to Phase 3.
Cycle structure used in trials
Trial-protocol cycle structure
Phase
Run-in
Duration
2 weeks
Notes
Diet stabilization, no tesofensine; used to baseline weight and labs
Phase
Treatment
Duration
24 weeks
Notes
Once-daily tablet at the assigned dose, alongside calorie-restricted diet
Phase
Open-label extension (TIPO-4)
Duration
Up to 48 additional weeks
Notes
Continued 0.5 mg with optional up-titration to 1.0 mg in some patients
| Phase | Duration | Notes |
|---|---|---|
| Run-in | 2 weeks | Diet stabilization, no tesofensine; used to baseline weight and labs |
| Treatment | 24 weeks | Once-daily tablet at the assigned dose, alongside calorie-restricted diet |
| Open-label extension (TIPO-4) | Up to 48 additional weeks | Continued 0.5 mg with optional up-titration to 1.0 mg in some patients |
Most published efficacy comes from the 24-week treatment window. Long-term data past 1 year is limited.
For protocol math beyond what trials reported
Peptide Dosing Protocols only summarizes the trial dosing record. It does not provide personal-use cycle plans, titration schedules, or stacking advice.
Tesofensine Supplies Needed
Tesofensine is an oral tablet, not an injectable peptide, so it does not require BAC water, syringes, or swabs. The math below shows how many tablets a 24-week trial-style schedule would use at the two doses tested. The injection-supplies card is included only for readers comparing injectable protocols elsewhere.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

Orbitrex Peptides Shop

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Tablets at 0.5 mg daily (one 0.5 mg tablet per day)
Some suppliers package tesofensine as 500 mcg (0.5 mg) tablets. One tablet per day matches the higher-dose Phase 2 and Phase 3 arms.
| Cycle length | Planning note |
|---|---|
4 weeks 28 tablets | 1 tablet per day x 28 days |
8 weeks 56 tablets | 1 tablet per day x 56 days |
12 weeks 84 tablets | 1 tablet per day x 84 days |
24 weeks 168 tablets | Matches the 24-week Phase 2/Phase 3 treatment window |
4 weeks
28 tablets
1 tablet per day x 28 days
8 weeks
56 tablets
1 tablet per day x 56 days
12 weeks
84 tablets
1 tablet per day x 84 days
24 weeks
168 tablets
Matches the 24-week Phase 2/Phase 3 treatment window
Tablets at 0.25 mg daily (half a 0.5 mg tablet, or one 0.25 mg tablet)
Supplier tablets are commonly scored at 0.5 mg. A 0.25 mg target means either a 0.25 mg tablet from a supplier that stocks that size, or half of a scored 0.5 mg tablet. Pill-splitter accuracy is imperfect; this is a planning note, not a recommendation.
| Cycle length | Planning note |
|---|---|
4 weeks 28 half-tablets (14 x 0.5 mg) | Half a 0.5 mg tablet per day x 28 days = 14 full tablets |
8 weeks 56 half-tablets (28 x 0.5 mg) | 28 full 0.5 mg tablets if splitting |
12 weeks 84 half-tablets (42 x 0.5 mg) | 42 full 0.5 mg tablets if splitting |
24 weeks 168 half-tablets (84 x 0.5 mg) | Matches the full 24-week 0.25 mg arm of Phase 2/Phase 3 |
4 weeks
28 half-tablets (14 x 0.5 mg)
Half a 0.5 mg tablet per day x 28 days = 14 full tablets
8 weeks
56 half-tablets (28 x 0.5 mg)
28 full 0.5 mg tablets if splitting
12 weeks
84 half-tablets (42 x 0.5 mg)
42 full 0.5 mg tablets if splitting
24 weeks
168 half-tablets (84 x 0.5 mg)
Matches the full 24-week 0.25 mg arm of Phase 2/Phase 3
Round up slightly for travel days, dropped tablets, and any schedule changes. Tesofensine has no reconstitution math because it is not an injectable peptide.
Companion Supplies & Routine Support
Tesofensine Dosage Chart
This Tesofensine dosage chart summarizes the oral clinical-trial doses from 0.25 mg to 1.0 mg daily shown in the dosing section above.
Tesofensine Reconstitution Guide
Tesofensine is an oral tablet. There is no reconstitution. The compound is not a peptide in the structural sense — it is a small molecule that survives the stomach and is absorbed after swallowing.
Why this section is short
Most PDP protocol pages cover bacteriostatic water, vial concentration, and syringe-unit math. Tesofensine does not need any of that. If you reached this page from a peptide protocol, the steps you are used to do not apply here.
If a supplier sells a powder
A small number of research suppliers list tesofensine as a powder for laboratory analytical use rather than as a finished tablet. Powder form is not a research-protocol equivalent of the trial tablet. Trial efficacy and safety numbers came from manufactured oral tablets dosed at 0.25 mg or 0.5 mg with known purity, fill, and dissolution. Powder formats do not have those guarantees.
How Tesofensine Works
Tesofensine increases the brain levels of three signaling chemicals at the same time: dopamine, norepinephrine, and serotonin. It does this by blocking the transporters that normally pull these chemicals back into the cell after they are released. With less reuptake, more signal stays in the synapse — the small gap between two brain cells.
The drug was first studied for Parkinson's and Alzheimer's disease because dopamine signaling matters in both. The neurological results were weaker than the developer hoped. The unexpected finding was weight loss. Patients lost weight in a dose-dependent way without anyone telling them to diet. That observation moved the program into obesity.
Two ways the brain pushes weight down
In animal and human studies, two effects show up. The first is reduced appetite, driven by higher dopamine and norepinephrine signaling in the hypothalamus, the part of the brain that helps regulate hunger. The second is a small rise in resting energy use, driven by higher norepinephrine signaling in peripheral tissues. Together these create the calorie gap that pushes weight down.
Half-life and steady state in plain language
Half-life is the time it takes for half of a dose to leave the body. For tesofensine that is about 9 days. Most drugs have half-lives measured in hours. A 9-day half-life means each daily tablet adds onto what is still in the body from prior days. Levels keep rising for about 4-6 weeks before they level off.
Two practical effects fall out of this. First, the full appetite effect builds gradually over the first month, not in the first 24 hours. Second, side effects that show up at week 5 or week 6 are not random — they often track steady state, not the most recent tablet.
Main mechanism
Inhibits the reuptake of dopamine, norepinephrine, and serotonin in the brain (a triple monoamine reuptake inhibitor, or SNDRI).
Active metabolite
Tesofensine is metabolized by CYP3A4 to a single metabolite (M1, or NS2360). M1 has a longer half-life — about 16 days — but contributes a smaller share of the overall pharmacologic effect.
Where it acts
Central nervous system, with downstream effects on appetite regulation and resting energy expenditure.
What it is not
Not a GLP-1 like semaglutide or tirzepatide. Not a stimulant in the amphetamine sense, though norepinephrine signaling overlaps.
Who Tesofensine Was Studied In and Who Should Avoid It
The Phase 2 and Phase 3 trials enrolled adults with obesity, generally defined as a body mass index of 30-40 kg/m². Patients with significant cardiovascular disease, uncontrolled high blood pressure, and active psychiatric disease were excluded. That matters when reading the safety numbers — the trial population was healthier than the general population that would actually seek the drug.
Groups where caution flags are highest
- People with uncontrolled high blood pressure or known cardiovascular disease. Tesofensine raises heart rate, and the 1.0 mg dose raised blood pressure as well.
- People with anxiety disorders, bipolar disorder, or a history of psychosis. The drug increases monoamine signaling and may worsen these conditions.
- People taking MAO inhibitors. The combination raises the risk of serotonin syndrome and severe blood pressure spikes.
- People taking SSRIs, SNRIs, or other serotonergic drugs. The combined load on the serotonin system is a real concern even though no formal interaction study exists.
- People taking strong CYP3A4 inhibitors (some antifungals, some antibiotics, grapefruit juice in large amounts). These can raise tesofensine levels.
- People who are pregnant, planning pregnancy, or breastfeeding. Tesofensine has not been studied in these groups.
- Adolescents and children. Trial data in obesity is in adults only.
Oversight is not optional
Tesofensine is an investigational drug in the United States. In Mexico, it is undergoing a delayed approval process. Any clinical use should involve qualified medical oversight including baseline cardiovascular and mental-health evaluation.
Tesofensine Side Effects & Safety
The most common side effects reported across trials were dry mouth, nausea, dizziness, abdominal pain, constipation, and insomnia. In the original Phase 2 study, about 71% of patients in the 0.5 mg arm completed the 24-week treatment and roughly 20% withdrew due to adverse events. Dry mouth was the single most reported symptom.
Cardiovascular signal
This is the most discussed safety topic. In the Phase 2 trial, heart rate rose by an average of 7.4 beats per minute in the 0.5 mg arm versus placebo. Blood pressure did not rise meaningfully at 0.25 mg or 0.5 mg, but it did rise at 1.0 mg. This pattern is why the 1.0 mg dose was dropped from Phase 3 and why US and EU regulators have been reluctant to advance the program without a dedicated cardiovascular outcomes study.
Psychiatric signal
Because tesofensine raises serotonin, dopamine, and norepinephrine, mood and sleep effects are biologically expected. Insomnia is one of the more common reasons people stop. Anxiety, irritability, and mood changes have been reported. In the Phase 2 paper there was no clear depression signal, but a letter to the editor in The Lancet noted that the trial excluded patients with psychiatric histories, which makes the safety estimate look better than it might be in a general population.
Quality-control risk for non-trial product
Trial efficacy and safety came from manufactured tablets with verified content and uniformity. Research-use product from grey-market suppliers does not carry those guarantees. Variable tablet content is a major source of unexpected adverse events. Verify any certificate of analysis before assuming a research product matches trial dosing.
Most reported tesofensine adverse events by category
Category
Dry mouth and GI
Examples reported
Dry mouth, nausea, constipation, abdominal pain, diarrhea
Comment
Most frequent; usually mild but can drive dropout
Category
Sleep
Examples reported
Insomnia, vivid dreams, reduced sleep duration
Comment
Tied to norepinephrine and dopamine signaling; morning dosing helps in trials
Category
Cardiovascular
Examples reported
Heart rate increase of 5-10 bpm typical at 0.5 mg, blood pressure rise mostly at 1.0 mg
Comment
Main reason the US and EU programs stalled
Category
Psychiatric
Examples reported
Anxiety, irritability, mood changes
Comment
Trials excluded active psychiatric disease; real-world rate may be higher
Category
Other
Examples reported
Headache, dizziness, fatigue
Comment
Generally less common
| Category | Examples reported | Comment |
|---|---|---|
| Dry mouth and GI | Dry mouth, nausea, constipation, abdominal pain, diarrhea | Most frequent; usually mild but can drive dropout |
| Sleep | Insomnia, vivid dreams, reduced sleep duration | Tied to norepinephrine and dopamine signaling; morning dosing helps in trials |
| Cardiovascular | Heart rate increase of 5-10 bpm typical at 0.5 mg, blood pressure rise mostly at 1.0 mg | Main reason the US and EU programs stalled |
| Psychiatric | Anxiety, irritability, mood changes | Trials excluded active psychiatric disease; real-world rate may be higher |
| Other | Headache, dizziness, fatigue | Generally less common |
Source numbers are from Astrup 2008 (Lancet) and the Doggrell 2009 evaluation of that trial.
Tesofensine Timeline & What to Monitor
Because of the 9-day half-life, the appetite-suppression effect builds over the first 4-6 weeks. Some people notice a reduction in cravings within the first week. The full effect typically takes longer.
Trial-reported timeline at 0.5 mg daily
Time point
Week 1-2
What the trials reported
Early appetite suppression in many patients
Time point
Week 4-6
What the trials reported
Steady-state plasma levels reached; effect more stable
Time point
Week 12
What the trials reported
Around half of the 24-week weight loss usually observed by this point
Time point
Week 24
What the trials reported
Phase 2 primary endpoint: about 10-11% body weight loss at 0.5 mg; about 6-7% at 0.25 mg
Time point
Beyond 24 weeks
What the trials reported
Long-term data is thinner; the TIPO-4 extension followed some patients for an additional 48 weeks
| Time point | What the trials reported |
|---|---|
| Week 1-2 | Early appetite suppression in many patients |
| Week 4-6 | Steady-state plasma levels reached; effect more stable |
| Week 12 | Around half of the 24-week weight loss usually observed by this point |
| Week 24 | Phase 2 primary endpoint: about 10-11% body weight loss at 0.5 mg; about 6-7% at 0.25 mg |
| Beyond 24 weeks | Long-term data is thinner; the TIPO-4 extension followed some patients for an additional 48 weeks |
These are trial population averages. Individual response varies.
What clinicians watched in trials
- Resting heart rate and blood pressure at baseline, then at regular intervals.
- Body weight and waist circumference.
- Mood, sleep, and anxiety screening, especially in the first few weeks.
- Any signs of fluid changes (dry mouth, constipation patterns).
- Routine labs in some studies (glucose, lipids, electrolytes).
Why monitoring is not optional in trial-style research
The trial safety database is built on the assumption that someone was checking blood pressure and heart rate at regular visits. The numbers people quote (about 10% weight loss, about 7 bpm heart rate rise) only mean something when paired with that monitoring.
Tesofensine Clinical Evidence Context
Tesofensine has more human evidence than most research-use peptide compounds. The two main human data sources are the 2008 Phase 2 Lancet trial led by Astrup and colleagues, and the Mexican Phase 3 program led by Medix in 372 patients.
Phase 2 (Astrup 2008, Lancet)
Design
Randomized, double-blind, placebo-controlled trial in 203 obese adults across five Danish centers. 24-week treatment, four arms: placebo, 0.25 mg, 0.5 mg, and 1.0 mg.
Result
Mean weight loss above placebo: about 4.5% at 0.25 mg, about 9.2% at 0.5 mg, about 10.6% at 1.0 mg. About 87% of 0.5 mg patients lost more than 5 kg.
Caveat
An Expression of Concern was later issued by The Lancet about two of the five trial sites. The authors responded; the trial conclusions remain in the published record but the audit history is worth knowing.
Phase 3 (Medix, Mexico)
Design
Randomized, double-blind, placebo-controlled, 372 patients in three arms (placebo, 0.25 mg, 0.5 mg). 24-week treatment period. Sponsored by Medix in Mexico under license from Saniona.
Result
Confirmed the Phase 2 efficacy pattern: significant weight loss at both 0.25 mg and 0.5 mg compared to placebo, with about 10% mean weight loss at the higher dose over 24 weeks. Heart rate showed a small but statistically significant rise; blood pressure showed no significant change at the tested doses.
Other supporting work
- TIPO-1 (the Phase 2 trial) and TIPO-4 (its open-label extension) are the original NeuroSearch trial set.
- Earlier observation: weight loss was noticed as a side effect when tesofensine was tested in Parkinson's and Alzheimer's disease.
- Animal and preclinical work supports the appetite and energy expenditure mechanisms.
- Combined trial safety database across the program includes about 1,600 patients exposed at therapeutic doses.
Tesofensine Storage & Handling
Tablets are typically stable at room temperature in a closed container away from light, moisture, and heat. Specific shelf-life and storage instructions depend on the supplier and the product formulation. Tablets generally do not need refrigeration the way reconstituted peptides do.
General oral-tablet storage guidance
Format
Sealed tablet bottle
Storage
59-77F (15-25C), dry, dark
Notes
Check the supplier label for any specific deviation
Format
Out-of-bottle tablets in a pill organizer
Storage
Same range; minimize humidity
Notes
Less ideal for long-term storage; refill weekly
Format
Powder format (analytical use only)
Storage
Per supplier instructions, often refrigerated or frozen
Notes
Powder form does not match trial dosing context
| Format | Storage | Notes |
|---|---|---|
| Sealed tablet bottle | 59-77F (15-25C), dry, dark | Check the supplier label for any specific deviation |
| Out-of-bottle tablets in a pill organizer | Same range; minimize humidity | Less ideal for long-term storage; refill weekly |
| Powder format (analytical use only) | Per supplier instructions, often refrigerated or frozen | Powder form does not match trial dosing context |
Confirm the exact storage requirements on the supplier's certificate of analysis before assuming.
Tesofensine Protocol Mistakes & Troubleshooting
Most issues come from misunderstanding the 9-day half-life. Common confusions, and what the trial record suggests:
Missed a dose
Because the half-life is so long, a single missed dose has almost no effect on plasma levels at steady state. In trial protocols, patients were generally instructed to take the next scheduled dose and not double up.
Insomnia at night
This is one of the most common reasons people stop tesofensine. Trial protocols recommended morning dosing for this reason. Late-day caffeine, late-day stimulants, and late-day blue light can stack with the drug's signal.
Resting heart rate creeping up
A 5-10 bpm rise was expected in the 0.5 mg trial arm. A rise larger than that, especially with chest discomfort or shortness of breath, is a stopping signal. This is one of the strongest reasons clinical use needs blood pressure and heart rate tracking.
Appetite suppression returned
Some people notice the appetite effect wears off after several months. The trials did not extend long enough at this dose to fully characterize this. The TIPO-4 extension allowed up-titration to 1.0 mg, but as noted that dose carried more cardiovascular signal.
Mood changes
Anxiety, irritability, or new low mood that started after beginning the drug is a meaningful signal, not a personality issue. Pause and reassess. Combining tesofensine with SSRIs, SNRIs, or MAOIs is specifically discouraged.
Mixed up tesofensine with a peptide
Tesofensine is a small molecule taken orally, not an injectable peptide. There is no reconstitution, no BAC water, no insulin syringe math. If you are reading this page after looking for peptide injection technique, you are in the wrong place — try the BPC-157 protocol or semaglutide protocol instead.
Tesofensine Regulatory Status
As of June 2026, tesofensine is not FDA approved in the United States for any indication. It is not in any active US new drug application pipeline. The FDA's published novel drug approval lists for 2024, 2025, and 2026 do not include tesofensine.
Mexico
Medix, the Mexican partner of Saniona, ran the 372-patient Phase 3 program. Medix filed a New Drug Application with COFEPRIS (the Mexican equivalent of the FDA) in December 2019. In February 2023, COFEPRIS's technical committee on new molecules issued a favorable opinion, which is not the same as final market authorization. In late 2024, Saniona reported that Medix had not received approval and was in dialogue with the agency. As of June 2026, full Mexican market authorization remains unresolved.
European Union and other regions
There is no active EU submission. EU regulators, like the FDA, would likely require a dedicated cardiovascular outcomes trial before considering approval. That study has not been conducted.
Tesomet and Nupenta
Tesomet is a combination product: tesofensine plus the beta-blocker metoprolol, designed to counter the heart rate signal. Saniona has been developing Tesomet for hypothalamic obesity and Prader-Willi syndrome. Nupenta is a separate combination product associated with the Mexican program. Neither is FDA approved.
Status changes faster than this page
Regulatory status for tesofensine can change with any COFEPRIS update or Saniona pipeline announcement. Verify current status before assuming what is in this section is current.
Tesofensine vs Semaglutide vs Tirzepatide
Tesofensine, semaglutide, and tirzepatide all reduce body weight, but they work in completely different ways and have different regulatory profiles. They are not interchangeable.
Tesofensine vs semaglutide vs tirzepatide at a glance
Mechanism
Tesofensine
Triple monoamine reuptake inhibitor (dopamine, norepinephrine, serotonin)
Semaglutide
GLP-1 receptor agonist
Tirzepatide
Dual GIP and GLP-1 receptor agonist
Route
Tesofensine
Oral tablet, once daily
Semaglutide
Weekly injection (Ozempic/Wegovy); oral daily (Rybelsus)
Tirzepatide
Weekly injection (Mounjaro/Zepbound)
Trial weight loss
Tesofensine
About 10% at 0.5 mg over 24 weeks (Phase 2 and Phase 3)
Semaglutide
About 15% over 68 weeks (STEP trials)
Tirzepatide
About 21% over 72 weeks (SURMOUNT trials)
FDA status (June 2026)
Tesofensine
Not approved for any indication
Semaglutide
Approved (Wegovy for obesity, Ozempic for type 2 diabetes)
Tirzepatide
Approved (Zepbound for obesity, Mounjaro for type 2 diabetes)
Main safety concern
Tesofensine
Heart rate rise, insomnia, mood
Semaglutide
Nausea, GI upset, rare pancreatitis
Tirzepatide
Nausea, GI upset, rare pancreatitis
| Tesofensine | Semaglutide | Tirzepatide | |
|---|---|---|---|
| Mechanism | Triple monoamine reuptake inhibitor (dopamine, norepinephrine, serotonin) | GLP-1 receptor agonist | Dual GIP and GLP-1 receptor agonist |
| Route | Oral tablet, once daily | Weekly injection (Ozempic/Wegovy); oral daily (Rybelsus) | Weekly injection (Mounjaro/Zepbound) |
| Trial weight loss | About 10% at 0.5 mg over 24 weeks (Phase 2 and Phase 3) | About 15% over 68 weeks (STEP trials) | About 21% over 72 weeks (SURMOUNT trials) |
| FDA status (June 2026) | Not approved for any indication | Approved (Wegovy for obesity, Ozempic for type 2 diabetes) | Approved (Zepbound for obesity, Mounjaro for type 2 diabetes) |
| Main safety concern | Heart rate rise, insomnia, mood | Nausea, GI upset, rare pancreatitis | Nausea, GI upset, rare pancreatitis |
Direct head-to-head trials between tesofensine and GLP-1 drugs have not been run.
Tesofensine vs Tesomet
Tesomet is tesofensine plus metoprolol, a beta-blocker. The reason to add metoprolol is to blunt the heart rate rise that comes with tesofensine. Tesomet is being studied for hypothalamic obesity and Prader-Willi syndrome, not general obesity.
Tesofensine vs phentermine
Phentermine is a short-acting stimulant that mostly affects norepinephrine release. Tesofensine is a long-acting reuptake inhibitor affecting three transmitters. Phentermine is FDA approved for short-term obesity use; tesofensine is not approved anywhere in the US.
Tesofensine Blood Tests & Monitoring
Tesofensine is usually discussed as a monoamine reuptake inhibitor research compound for appetite and weight loss. Monitoring focuses on cardiovascular context, metabolic trends, and psychiatric or medication-interaction risk.
Blood test markers to discuss with a clinician
Marker
Blood pressure and resting heart rate
Why it matters
Tesofensine’s stimulant-like pathway makes cardiovascular monitoring especially relevant.
Timing
Baseline
Marker
A1c
Why it matters
Shows longer-term glucose control during weight-loss or appetite-change protocols.
Timing
Baseline
Marker
Lipid panel
Why it matters
Tracks cardiometabolic changes during weight-loss phases.
Timing
Follow-up
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver, kidney, electrolyte, and glucose context before interpreting appetite or energy changes.
Timing
Baseline
Marker
TSH and free T4
Why it matters
Thyroid imbalance can mimic or worsen stimulant-like symptoms such as palpitations, anxiety, and weight change.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| Blood pressure and resting heart rate | Tesofensine’s stimulant-like pathway makes cardiovascular monitoring especially relevant. | Baseline |
| A1c | Shows longer-term glucose control during weight-loss or appetite-change protocols. | Baseline |
| Lipid panel | Tracks cardiometabolic changes during weight-loss phases. | Follow-up |
| Comprehensive metabolic panel (CMP) | Reviews liver, kidney, electrolyte, and glucose context before interpreting appetite or energy changes. | Baseline |
| TSH and free T4 | Thyroid imbalance can mimic or worsen stimulant-like symptoms such as palpitations, anxiety, and weight change. | Optional |
Monitoring guidance is pathway-based and informed by monoamine and weight-loss drug safety considerations.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline review before starting, especially with high blood pressure, arrhythmia, anxiety, stimulant use, antidepressants, diabetes, or cardiovascular disease.
Follow-up
Re-check blood pressure, resting heart rate, and metabolic markers after 4-8 weeks or sooner if symptoms change.
Longer term
For longer protocols, review cardiovascular and mood-related context periodically with a clinician.
How to interpret the labs
- Medication interactions are important, especially with stimulants, antidepressants, or blood-pressure medications.
- Anxiety, insomnia, palpitations, and mood changes should be tracked clinically.
- Weight-loss labs do not replace cardiovascular and psychiatric review.
Do not wait for routine labs
Chest pain, fainting, severe headache, severe anxiety, mania symptoms, or suicidal thoughts need medical review. Fast or irregular heartbeat should not be treated as routine appetite-suppression discomfort.
FAQ
Q1: Is tesofensine FDA approved?
No. As of June 2026, tesofensine is not approved by the FDA for any indication. It is not in any active US new drug application pipeline. The drug has been studied in human trials, including a Phase 2 trial published in The Lancet in 2008 and a Phase 3 trial in 372 patients in Mexico, but a dedicated cardiovascular outcomes trial that US and EU regulators would expect has not been run.
Q2: What dose of tesofensine was studied in clinical trials?
The two doses most studied are 0.25 mg and 0.5 mg, taken once daily as an oral tablet. The original Phase 2 trial also included a 1.0 mg arm, but that dose was dropped from the Phase 3 program because it raised blood pressure and increased dropouts. This is research-protocol context, not a dosing recommendation.
Q3: How long does tesofensine take to work?
Some appetite reduction is reported in the first 1-2 weeks. Because tesofensine has a half-life of about 9 days, the drug builds up over the first 4-6 weeks before reaching steady state. Most of the 24-week trial weight loss accumulates after that point.
Q4: Why does tesofensine have such a long half-life?
Tesofensine is metabolized slowly by the liver enzyme CYP3A4 to a single active metabolite called M1 (also called NS2360). Both the parent compound and its metabolite are eliminated slowly, with the parent at about 9 days and M1 at about 16 days. That is why daily dosing leads to steady accumulation for the first month.
Q5: What time of day should tesofensine be taken?
Trial protocols generally used morning dosing. The reason is that tesofensine increases norepinephrine and dopamine signaling, which can disrupt sleep if peak signaling lands during the evening. This is a trial-protocol pattern, not a personal dosing instruction.
Q6: Does tesofensine raise blood pressure or heart rate?
It raises heart rate in a dose-dependent way. The Phase 2 0.5 mg arm showed an average heart rate rise of about 7 beats per minute. Blood pressure was largely unchanged at 0.25 mg and 0.5 mg, but rose at 1.0 mg. The cardiovascular signal is the main reason US and EU regulators have not advanced the drug.
Q7: Can tesofensine be combined with semaglutide or tirzepatide?
No combination trial has been published. Tesofensine works on brain neurotransmitter pathways and the GLP-1 drugs work on gut hormone pathways, so they are mechanistically different. That does not mean they are safe to combine; layering appetite suppressants increases the risk of side effects, dehydration, electrolyte issues, and cardiovascular strain. Any combined use should involve qualified medical oversight.
Q8: What is the difference between tesofensine, Tesomet, and Nupenta?
Tesofensine is the single active compound. Tesomet is tesofensine plus the beta-blocker metoprolol, designed to blunt the heart rate signal; it is being studied for hypothalamic obesity and Prader-Willi syndrome. Nupenta is a Mexican combination product also derived from the tesofensine program. Saniona retains rights outside Mexico and Argentina, where Medix holds local rights.
Q9: Is tesofensine the same as a peptide?
Chemically, no. Tesofensine is a small molecule from the phenyltropane family, not a peptide. Some research-use suppliers list it in their peptide catalog because that is how their store is organized, but the molecule itself is not a peptide. There is also no reconstitution because it is an oral tablet, not an injectable.
Q10: How does tesofensine compare to phentermine?
Phentermine is a short-acting stimulant that mostly affects norepinephrine release. Tesofensine is a long-acting reuptake inhibitor that affects dopamine, norepinephrine, and serotonin. Phentermine is FDA approved for short-term obesity treatment in the United States; tesofensine is not approved for any indication. The cardiovascular and sleep side-effect profiles overlap but are not identical.
Q11: Is this page medical advice?
No. This page is an educational research reference describing the doses and outcomes reported in published tesofensine trials. It is not a prescription, not a treatment plan, and not a recommendation. Any clinical decision about tesofensine should involve qualified medical oversight including baseline cardiovascular and mental-health evaluation.
Sources & Research
- 1. Astrup A, Madsbad S, Breum L, Jensen TJ, Kroustrup JP, Larsen TM Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients: a randomised, double-blind, placebo-controlled trial. The Lancet (2008)
- 2. Doggrell SA Tesofensine — a novel potent weight loss medicine. Evaluation of Astrup et al. (Lancet 2008). Expert Opinion on Investigational Drugs (2009)
- 3. The Lancet Editors Expression of concern — Effect of tesofensine on bodyweight loss, body composition, and quality of life in obese patients. The Lancet (2014)
- 4. Lehr T, Staab A, Tillmann C, et al. Contribution of the active metabolite M1 to the pharmacological activity of tesofensine in vivo: a pharmacokinetic-pharmacodynamic modelling approach. British Journal of Pharmacology (2008)
- 5. Appel L, Bergstrom M, Buus Lassen J, Langstrom B Tesofensine, a novel triple monoamine re-uptake inhibitor with anti-obesity effects: dopamine transporter occupancy as measured by PET. European Neuropsychopharmacology (2014)
- 6. Saniona AB Saniona's tesofensine meets primary and secondary endpoints in Phase 3 obesity registration trial (Viking study). Saniona corporate press release / Euroland Investor (2018)
- 7. Saniona AB Saniona's partner Medix receives favorable opinion for tesofensine for the treatment of obesity in Mexico. Saniona / Nasdaq News (2023)
- 8. Saniona AB Mexican application for tesofensine not yet approved — Saniona update. Inderes / Saniona (2024)
- 9. Perez CI, Luis-Islas J, Lopez A, et al. Tesofensine, a novel antiobesity drug, silences GABAergic hypothalamic neurons. PLOS ONE (2024)
- 10. Onakpoya IJ, Lee JJ, Mahtani KR, Aronson JK, Heneghan CJ Neuropsychiatric adverse effects of centrally acting antiobesity drugs: a systematic review of randomized controlled trials. PMC / Frontiers (2019)
- 11. Saniona AB Tesofensine pipeline page. Saniona corporate site (2024)
- 12. US Food and Drug Administration Novel Drug Approvals for 2026. FDA.gov (2026)
Related Dosing Protocols
Educational use only
This guide is an educational research reference, not medical advice or a treatment plan. Tesofensine is not FDA approved and its long-term safety profile is not fully characterized.
Compare GLP-1 alternatives
If you arrived here researching weight-loss options, the FDA-approved GLP-1 protocols are a sensible next reference point.
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page