SLU-PP-332 Quick Start
Disclaimer
This page is an educational research reference and is not medical advice. SLU-PP-332 is not FDA-approved and has no human clinical trial program as of June 2026. No information on this page is intended as a personal dosing recommendation.
SLU-PP-332 is a synthetic small-molecule pan-agonist of the estrogen-related receptors (ERRα, ERRβ, and ERRγ). ERRs are nuclear receptors that sit upstream of mitochondrial biogenesis, fatty acid oxidation, and the aerobic gene program activated by endurance exercise. In plain English, SLU-PP-332 flips many of the same intracellular switches that training flips, which is why it is often described as an exercise mimetic.
Despite the "peptide" label used in many product listings, SLU-PP-332 is not a peptide at all. It is a small organic molecule (C18H14N2O2, MW 290.3 g/mol, CAS 303760-60-3) built on a benzohydrazide scaffold. We include it on PDP because the research community treats it as a peptide-adjacent metabolic tool and frequently compares it to peptides like MOTS-c and AOD-9604.
Research-grade suppliers carry SLU-PP-332 in two main formats: 50 mg oral tablets (commonly sold as a 60-count bottle) and injectable vials at 5 mg or 10 mg strengths. The tablet form is now the most common consumer-research presentation; the vial form is what published animal studies used (intraperitoneal injection in mice).
Format
Primary research format is a 50 mg oral tablet (60-count bottle). Injection vials of 5 mg and 10 mg are also available.
Schedule
Mouse studies used twice daily intraperitoneal injection. Community oral protocols are typically once daily; no human dosing schedule has been clinically validated.
Measure
For tablets, dose count and bottle count drive supplies math. For vials, use vial concentration and U-100 syringe units.
Supplies
Tablet route needs only the bottle. Vial route adds bacteriostatic water, U-100 insulin syringes, and alcohol swabs.
Research status
Preclinical only. Four published in-vivo mouse studies. No registered or completed human trial as of June 2026.
Need to convert vial concentration to syringe units? Use the Pep Pal reconstitution calculator to lock in draw volume.
How SLU-PP-332 Works
Short version: SLU-PP-332 binds to ERRα, and to a lesser extent ERRβ and ERRγ. These are transcription factors in the cell nucleus that control how many mitochondria a cell builds, how efficiently those mitochondria burn fat, and how much oxidative capacity the cell has. When you run, muscle cells upregulate these same receptors. SLU-PP-332 does it pharmacologically. Think of ERRα as the master volume knob for a cell's aerobic machinery — SLU-PP-332 turns that knob up.
ERRα agonism — the primary driver
ERRα is highly expressed in energy-demanding tissues such as skeletal muscle, heart, brown adipose tissue, and liver. When activated, it switches on genes for mitochondrial biogenesis, oxidative phosphorylation, the TCA cycle, and fatty acid β-oxidation. In the Billon 2023 paper, a single 25 mg/kg intraperitoneal dose in mice was enough to induce an acute aerobic exercise transcriptional signature in muscle within hours.
Cell assays show SLU-PP-332 activates all three ERR isoforms but is roughly four-fold more potent at ERRα than ERRγ, with ERRβ in between (ERRα EC50 ≈ 98 nM, ERRγ EC50 ≈ 430 nM).
PGC-1α and mitochondrial biogenesis
ERRα works in partnership with PGC-1α, the master coactivator of mitochondrial biogenesis. Together they drive expression of nuclear-encoded mitochondrial genes, increasing both the number and efficiency of mitochondria in muscle and cardiac tissue. In the Billon 2023 study, 50 mg/kg twice daily for 28 days increased succinate dehydrogenase-positive oxidative muscle fibers and raised OXPHOS complex protein levels.
Fatty acid oxidation
In diet-induced obese mice and ob/ob mice, 50 mg/kg twice daily for 28 days increased whole-body energy expenditure and fatty acid oxidation, reduced fat mass, lowered cholesterol and triglycerides, and improved insulin sensitivity without changing food intake. That is a metabolic-rate mechanism, not an appetite-suppression mechanism like Semaglutide or Tirzepatide.
ERRγ and cardiac metabolism
In a pressure-overload heart-failure mouse model, six weeks of SLU-PP-332 improved ejection fraction, reduced fibrosis, and increased survival. The authors attributed the effect mainly to ERRγ engagement in cardiomyocytes, which normalized fatty acid metabolism and mitochondrial function without reversing hypertrophy itself. The practical takeaway is that ERRα appears to drive most skeletal-muscle effects, while ERRγ carries more of the cardiac signal.
Put together, SLU-PP-332 reproduces many of the cellular adaptations of endurance training at the transcriptional level. What it does not reproduce is the mechanical loading of actual exercise, so tendon, bone, and connective-tissue adaptations are not part of the promise. It is a metabolic research tool, not a substitute for training.
SLU-PP-332 Dosing Protocol & Schedule
Before any numbers: every published in-vivo dose for SLU-PP-332 is a mouse dose. There is no human titration schedule, no human pharmacokinetic study, no human safety margin, and no FDA-approved label. Human dosing figures circulating in the research community are either human-equivalent-dose extrapolations from mouse protocols or vendor-driven tablet/capsule suggestions with no primary-source backing.
The dosing guide below is split into the two formats actually available from research suppliers: oral tablets (the most common consumer-research format) and injectable vials (the format used in published animal studies).
SLU-PP-332 Format Tabs
Choose the format you are researching to see route-specific notes.
For the 50 mg / 60-count oral tablet form sold by research suppliers.
Oral tablets are the most common consumer-research format. The current featured supplier carries SLU-PP-332 as a 50 mg tablet in a 60-tablet bottle. Oral bioavailability in humans has not been formally published, so any dose number here is a community-pattern reference, not a clinically validated dose.
Community Oral Tablet Dosing Patterns
Pattern
Low-dose / micro-dose
Daily Dose
≤1.5 mg
Tablet Math (50 mg)
Not practical with a 50 mg tablet — typically uses smaller-strength vendor capsules instead
Frequency
Once daily
Notes
Common starting pattern in community oral protocols.
Pattern
Mid-dose
Daily Dose
25 mg (½ tablet)
Tablet Math (50 mg)
0.5 tablet/day → ~120 days from one 60-tablet bottle
Frequency
Once daily
Notes
Splitting a scored tablet; community-derived only.
Pattern
Standard supplier-tablet dose
Daily Dose
50 mg (1 tablet)
Tablet Math (50 mg)
1 tablet/day → ~60 days from one bottle
Frequency
Once daily
Notes
Anchored to the supplier's 50 mg tablet strength.
Pattern
Higher community pattern
Daily Dose
100 mg (2 tablets)
Tablet Math (50 mg)
2 tablets/day → ~30 days from one bottle
Frequency
Once or split twice daily
Notes
Reported informally; no controlled data.
Pattern
HED extrapolation ceiling
Daily Dose
~650 mg/day
Tablet Math (50 mg)
13 tablets/day — included only to show the gap with vendor doses
Frequency
n/a
Notes
Allometric scaling from 100 mg/kg/day mouse dose to 80 kg human. Not a recommendation; no human safety data exists at any dose.
| Pattern | Daily Dose | Tablet Math (50 mg) | Frequency | Notes |
|---|---|---|---|---|
| Low-dose / micro-dose | ≤1.5 mg | Not practical with a 50 mg tablet — typically uses smaller-strength vendor capsules instead | Once daily | Common starting pattern in community oral protocols. |
| Mid-dose | 25 mg (½ tablet) | 0.5 tablet/day → ~120 days from one 60-tablet bottle | Once daily | Splitting a scored tablet; community-derived only. |
| Standard supplier-tablet dose | 50 mg (1 tablet) | 1 tablet/day → ~60 days from one bottle | Once daily | Anchored to the supplier's 50 mg tablet strength. |
| Higher community pattern | 100 mg (2 tablets) | 2 tablets/day → ~30 days from one bottle | Once or split twice daily | Reported informally; no controlled data. |
| HED extrapolation ceiling | ~650 mg/day | 13 tablets/day — included only to show the gap with vendor doses | n/a | Allometric scaling from 100 mg/kg/day mouse dose to 80 kg human. Not a recommendation; no human safety data exists at any dose. |
All oral tablet doses are community patterns. No published human trial supports any specific oral dose for SLU-PP-332. This is not a dosing recommendation.
Tablet timing and missed-dose notes
Most community oral protocols use morning dosing because of circadian metabolic effects. With no published human half-life, there is no validated missed-dose rule. Community oral users typically skip a missed dose rather than doubling up on the next one. Food effects on absorption have not been characterized in humans.
Capsule vs injection — which format?
Oral tablets are easier to handle and require no reconstitution. The trade-off is unknown oral bioavailability — in animal studies, every efficacy dose was delivered by intraperitoneal injection, not by mouth. If oral bioavailability in humans is low, oral tablet doses may need to be higher than the IP-injection-equivalent dose to achieve the same systemic exposure. There is no clinical data resolving that question.
For 5 mg or 10 mg injection vials reconstituted with bacteriostatic water.
Injection vials are the format used in every published animal study, but those studies used intraperitoneal injection in mice — not subcutaneous injection in humans. Community injectable users typically use subcutaneous injection of bacteriostatic-water-reconstituted vials. Bioavailability and pharmacokinetics for subcutaneous human administration are not published.
Published Murine Regimens (Reference Only)
Study
Billon 2023 — endurance
Duration
15 days
Dose & Route
25 mg/kg IP once daily
Outcome (Mouse)
Increased treadmill endurance; acute aerobic exercise transcriptional signature in muscle.
Study
Billon 2023 — chronic
Duration
28 days
Dose & Route
50 mg/kg IP twice daily
Outcome (Mouse)
Raised oxidative muscle fibers and OXPHOS proteins; longer running distance before exhaustion.
Study
Billon 2024 — DIO mice
Duration
28 days
Dose & Route
50 mg/kg IP twice daily
Outcome (Mouse)
Reduced fat mass; improved glucose tolerance; lower triglycerides.
Study
Billon 2024 — ob/ob mice
Duration
12 days
Dose & Route
50 mg/kg IP twice daily
Outcome (Mouse)
Improved metabolic markers in the ob/ob model.
Study
Xu 2024 — heart failure
Duration
6 weeks
Dose & Route
IP dosing (Burris-lab standard)
Outcome (Mouse)
Improved ejection fraction; reduced fibrosis; increased survival in the TAC model.
Study
Wang 2023 — aging kidney
Duration
8 weeks
Dose & Route
25 mg/kg IP once daily
Outcome (Mouse)
Reduced albuminuria; preserved podocin; restored mitochondrial function.
| Study | Duration | Dose & Route | Outcome (Mouse) |
|---|---|---|---|
| Billon 2023 — endurance | 15 days | 25 mg/kg IP once daily | Increased treadmill endurance; acute aerobic exercise transcriptional signature in muscle. |
| Billon 2023 — chronic | 28 days | 50 mg/kg IP twice daily | Raised oxidative muscle fibers and OXPHOS proteins; longer running distance before exhaustion. |
| Billon 2024 — DIO mice | 28 days | 50 mg/kg IP twice daily | Reduced fat mass; improved glucose tolerance; lower triglycerides. |
| Billon 2024 — ob/ob mice | 12 days | 50 mg/kg IP twice daily | Improved metabolic markers in the ob/ob model. |
| Xu 2024 — heart failure | 6 weeks | IP dosing (Burris-lab standard) | Improved ejection fraction; reduced fibrosis; increased survival in the TAC model. |
| Wang 2023 — aging kidney | 8 weeks | 25 mg/kg IP once daily | Reduced albuminuria; preserved podocin; restored mitochondrial function. |
These doses are accurate for the published mouse models. They are not human dosing recommendations and have not been validated in any clinical setting.
Community subcutaneous protocols typically use 250 mcg to 1.5 mg per day from a reconstituted 5 mg vial. There is no primary-source efficacy data supporting those human doses. See the reconstitution section below for exact draw volumes by vial size and concentration.
Cycle Guidelines (Both Routes)
Approach
Short reference
Duration
4 weeks
Review Point
Week 4
Best For
Initial research planning window aligned with the shortest published mouse studies.
Approach
Standard
Duration
6-8 weeks
Review Point
Week 6
Best For
Matches Billon 2023/2024 chronic mouse exposure windows.
Approach
Extended
Duration
12 weeks
Review Point
Week 8 and Week 12
Best For
Longest community oral pattern; no human safety data beyond preclinical exposures.
| Approach | Duration | Review Point | Best For |
|---|---|---|---|
| Short reference | 4 weeks | Week 4 | Initial research planning window aligned with the shortest published mouse studies. |
| Standard | 6-8 weeks | Week 6 | Matches Billon 2023/2024 chronic mouse exposure windows. |
| Extended | 12 weeks | Week 8 and Week 12 | Longest community oral pattern; no human safety data beyond preclinical exposures. |
Community oral protocols often use 8-12 weeks on and 4 weeks off, but the rationale for cycling is theoretical because long-term receptor desensitization has not been measured in humans.
SLU-PP-332 Supplies Needed
Supplies math below assumes the supplier's 50 mg oral tablet (60-count bottle) for the tablet route, and a 5 mg injectable vial reconstituted with 2 mL of bacteriostatic water for the injectable route. Affiliate disclosure: PDP may earn a commission when you use eligible supplier links, at no extra cost to you.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

SLU-PP-332

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Oral Tablet — Bottle Math (50 mg × 60-count)
Counts assume one 50 mg tablet per day from the supplier's 60-tablet bottle. Adjust for split-tablet (25 mg) or two-tablet (100 mg) community patterns by halving or doubling the bottle count.
| Cycle length | Planning note |
|---|---|
4-8 weeks 1 bottle | 4 weeks: 28 tablets needed; one 60-count bottle covers a 4-week cycle with margin.; 6 weeks: 42 tablets needed; one 60-count bottle still covers it.; 8 weeks: 56 tablets needed; one bottle just fits — order a second to avoid a gap. |
12 weeks 2 bottles | 84 tablets needed; two 60-count bottles cover the full cycle with buffer. |
4-8 weeks
1 bottle
4 weeks: 28 tablets needed; one 60-count bottle covers a 4-week cycle with margin.; 6 weeks: 42 tablets needed; one 60-count bottle still covers it.; 8 weeks: 56 tablets needed; one bottle just fits — order a second to avoid a gap.
12 weeks
2 bottles
84 tablets needed; two 60-count bottles cover the full cycle with buffer.
Injectable Vials (Reference)
Counts assume a 5 mg vial reconstituted with 2 mL BAC water (2,500 mcg/mL) and a daily 500 mcg subcutaneous draw — a common community pattern, not a clinically validated dose.
| Cycle length | Planning note |
|---|---|
4 weeks 3 vials | 28 daily 500 mcg doses ≈ 14 mg total → at least 3 × 5 mg vials. |
6 weeks 5 vials | 42 daily 500 mcg doses ≈ 21 mg total → 5 × 5 mg vials with margin. |
8 weeks 6 vials | 56 daily 500 mcg doses ≈ 28 mg total → 6 × 5 mg vials. |
12 weeks 9 vials | 84 daily 500 mcg doses ≈ 42 mg total → 9 × 5 mg vials. Two 10 mg vials per month can replace four 5 mg vials. |
4 weeks
3 vials
28 daily 500 mcg doses ≈ 14 mg total → at least 3 × 5 mg vials.
6 weeks
5 vials
42 daily 500 mcg doses ≈ 21 mg total → 5 × 5 mg vials with margin.
8 weeks
6 vials
56 daily 500 mcg doses ≈ 28 mg total → 6 × 5 mg vials.
12 weeks
9 vials
84 daily 500 mcg doses ≈ 42 mg total → 9 × 5 mg vials. Two 10 mg vials per month can replace four 5 mg vials.
Insulin Syringes (U-100) — Injectable Route
Use 0.3 mL / 30-unit syringes for small daily draws (20 units for a 500 mcg dose at 2,500 mcg/mL). Add a few extras for priming losses and dropped syringes.
| Cycle length | Planning note |
|---|---|
4 weeks 30 syringes | 1 syringe per daily injection plus 2 spares. |
6 weeks 45 syringes | 1 syringe per daily injection plus 3 spares. |
8 weeks 60 syringes | 1 syringe per daily injection plus 4 spares. |
12 weeks 90 syringes | 1 syringe per daily injection plus 6 spares. |
4 weeks
30 syringes
1 syringe per daily injection plus 2 spares.
6 weeks
45 syringes
1 syringe per daily injection plus 3 spares.
8 weeks
60 syringes
1 syringe per daily injection plus 4 spares.
12 weeks
90 syringes
1 syringe per daily injection plus 6 spares.
Bacteriostatic Water — Injectable Route
Use 2 mL per 5 mg vial. Round up so a single 10 mL bottle covers the cycle with margin.
| Cycle length | Planning note |
|---|---|
4-6 weeks 1 × 10 mL bottle | 4 weeks: 3 vials × 2 mL = 6 mL; one bottle gives margin for replacement draws.; 6 weeks: 5 vials × 2 mL = 10 mL; order a second bottle to avoid running short. |
8-12 weeks 2 × 10 mL bottles | 8 weeks: 6 vials × 2 mL = 12 mL; two bottles give margin.; 12 weeks: 9 vials × 2 mL = 18 mL; two bottles cover the cycle with buffer. |
4-6 weeks
1 × 10 mL bottle
4 weeks: 3 vials × 2 mL = 6 mL; one bottle gives margin for replacement draws.; 6 weeks: 5 vials × 2 mL = 10 mL; order a second bottle to avoid running short.
8-12 weeks
2 × 10 mL bottles
8 weeks: 6 vials × 2 mL = 12 mL; two bottles give margin.; 12 weeks: 9 vials × 2 mL = 18 mL; two bottles cover the cycle with buffer.
Alcohol Swabs — Injectable Route
Use one swab for the vial stopper and one for the injection site, per injection.
| Cycle length | Planning note |
|---|---|
4 weeks 56 swabs | 2 per daily injection; recommend 1 × 100-count box. |
6 weeks 84 swabs | 2 per daily injection; recommend 1 × 100-count box. |
8 weeks 112 swabs | 2 per daily injection; recommend 2 × 100-count boxes. |
12 weeks 168 swabs | 2 per daily injection; recommend 2 × 100-count boxes. |
4 weeks
56 swabs
2 per daily injection; recommend 1 × 100-count box.
6 weeks
84 swabs
2 per daily injection; recommend 1 × 100-count box.
8 weeks
112 swabs
2 per daily injection; recommend 2 × 100-count boxes.
12 weeks
168 swabs
2 per daily injection; recommend 2 × 100-count boxes.
Round up for priming losses, dropped syringes, damaged swabs, missed doses, and any protocol adjustments. No supplies math here is a personal medical recommendation.
Companion Supplies & Routine Support
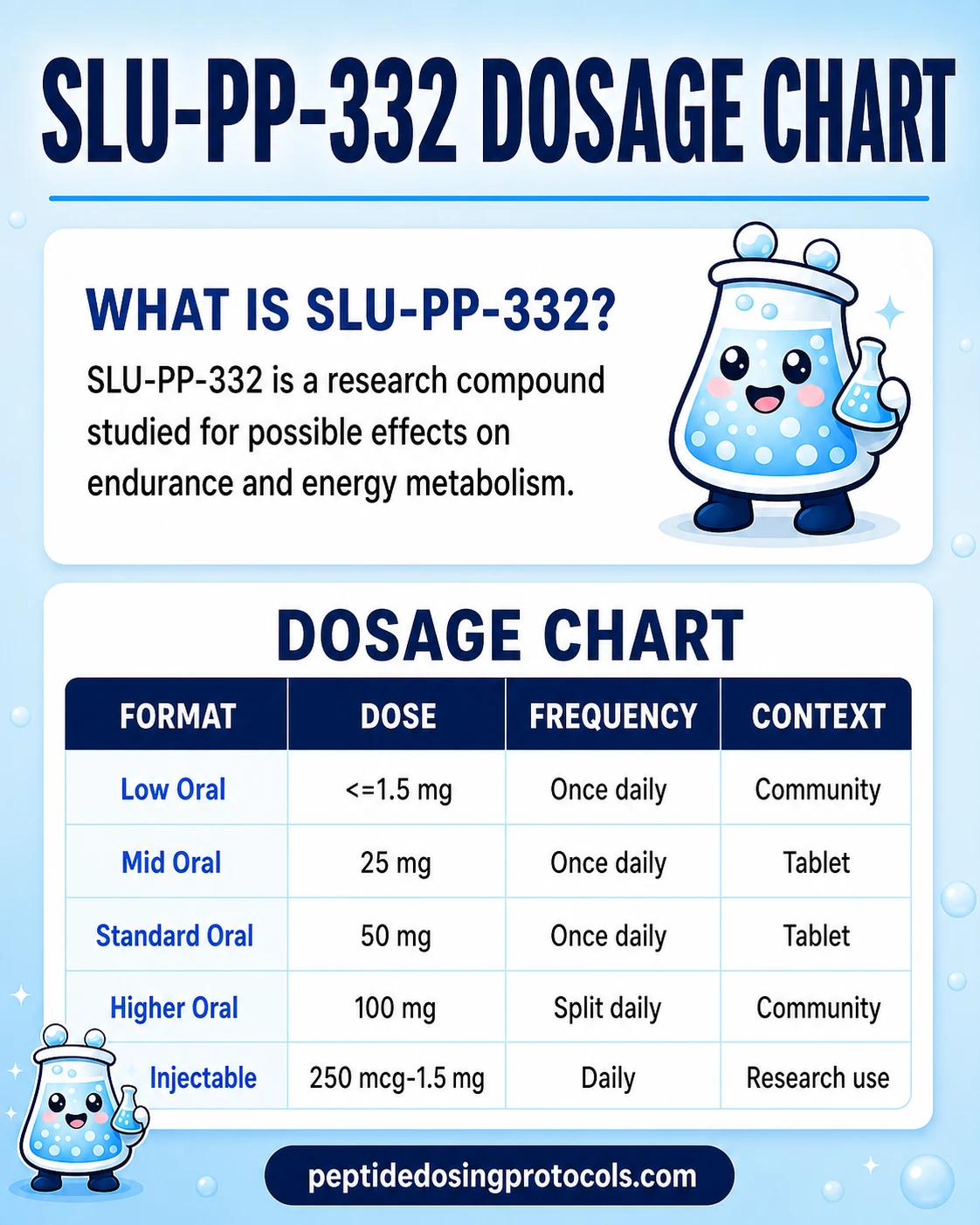
SLU-PP-332 Dosage Chart
This SLU-PP-332 dosage chart summarizes the oral tablet and injectable research-use dose patterns shown in the dosing section above.
SLU-PP-332 Reconstitution Guide
Oral tablets do not require reconstitution — skip this section if you are researching the 50 mg tablet form. The math below applies only to the injectable vial format.
SLU-PP-332 is a small molecule, not a peptide, so it behaves somewhat differently in solution than a typical lyophilized peptide. Published lab preparations often used DMSO-containing vehicles for animal work; community reconstitution protocols typically use bacteriostatic water for subcutaneous research use.
Math shown: Concentration in mcg/mL = total compound in mcg divided by water volume in mL. U-100 syringe units = volume in mL × 100. Example: 5 mg vial + 2 mL water = 5,000 mcg ÷ 2 mL = 2,500 mcg/mL. A 500 mcg dose is 500 ÷ 2,500 = 0.20 mL = 20 units on a U-100 insulin syringe.
Reconstitution Reference — 5 mg, 10 mg, and 20 mg Injection Vials
Vial Size
5 mg
BAC Water
1.0 mL
Concentration
5,000 mcg/mL
250 mcg
5 units (0.05 mL)
500 mcg
10 units (0.10 mL)
1 mg
20 units (0.20 mL)
5 mg
100 units (1.00 mL)
Vial Size
5 mg
BAC Water
2.0 mL
Concentration
2,500 mcg/mL
250 mcg
10 units (0.10 mL)
500 mcg
20 units (0.20 mL)
1 mg
40 units (0.40 mL)
5 mg
Full vial
Vial Size
5 mg
BAC Water
3.0 mL
Concentration
1,667 mcg/mL
250 mcg
15 units (0.15 mL)
500 mcg
30 units (0.30 mL)
1 mg
60 units (0.60 mL)
5 mg
—
Vial Size
10 mg
BAC Water
2.0 mL
Concentration
5,000 mcg/mL
250 mcg
5 units (0.05 mL)
500 mcg
10 units (0.10 mL)
1 mg
20 units (0.20 mL)
5 mg
100 units (1.00 mL)
Vial Size
10 mg
BAC Water
5.0 mL
Concentration
2,000 mcg/mL
250 mcg
12.5 units (0.125 mL)
500 mcg
25 units (0.25 mL)
1 mg
50 units (0.50 mL)
5 mg
—
Vial Size
20 mg
BAC Water
5.0 mL
Concentration
4,000 mcg/mL
250 mcg
6 units (0.06 mL)
500 mcg
12.5 units (0.125 mL)
1 mg
25 units (0.25 mL)
5 mg
125 units (1.25 mL)
| Vial Size | BAC Water | Concentration | 250 mcg | 500 mcg | 1 mg | 5 mg |
|---|---|---|---|---|---|---|
| 5 mg | 1.0 mL | 5,000 mcg/mL | 5 units (0.05 mL) | 10 units (0.10 mL) | 20 units (0.20 mL) | 100 units (1.00 mL) |
| 5 mg | 2.0 mL | 2,500 mcg/mL | 10 units (0.10 mL) | 20 units (0.20 mL) | 40 units (0.40 mL) | Full vial |
| 5 mg | 3.0 mL | 1,667 mcg/mL | 15 units (0.15 mL) | 30 units (0.30 mL) | 60 units (0.60 mL) | — |
| 10 mg | 2.0 mL | 5,000 mcg/mL | 5 units (0.05 mL) | 10 units (0.10 mL) | 20 units (0.20 mL) | 100 units (1.00 mL) |
| 10 mg | 5.0 mL | 2,000 mcg/mL | 12.5 units (0.125 mL) | 25 units (0.25 mL) | 50 units (0.50 mL) | — |
| 20 mg | 5.0 mL | 4,000 mcg/mL | 6 units (0.06 mL) | 12.5 units (0.125 mL) | 25 units (0.25 mL) | 125 units (1.25 mL) |
Concentrations rounded for the table. This is research-context math, not a personal dosing recommendation.
- 01
Warm the vial
Let the lyophilized vial reach room temperature for 5-10 minutes.
- 02
Wipe the stoppers
Use an alcohol swab on both the SLU-PP-332 vial and the bacteriostatic water vial.
- 03
Draw BAC water
Pull the target volume of bacteriostatic water into a sterile syringe based on the reconstitution table.
- 04
Inject slowly
Inject the water down the inside wall of the vial — do not blast diluent directly onto the powder.
- 05
Swirl to dissolve
Swirl gently until fully dissolved. Do not shake vigorously.
- 06
Label the vial
Note the reconstitution date and final concentration on the vial label.
- 07
Refrigerate and protect from light
Store at 2-8°C (35.6-46.4°F) protected from light.
Need exact syringe units?
Use the free Pep Pal reconstitution calculator — enter vial size, water volume, and target dose to get the exact U-100 unit mark.
Who SLU-PP-332 Is For and Who Should Avoid It
SLU-PP-332 is currently a preclinical research compound, so the honest answer is that no group has been formally cleared for use. The list below identifies populations where the risk-benefit picture is especially unclear and where independent research planning should err on the side of avoidance.
Avoid or use extra caution
Pregnant or breastfeeding individuals; people under 18; people with active or recent cancer (ERRα participates in some cancer-metabolism pathways); people with known cardiovascular disease, arrhythmia, or uncontrolled hypertension (chronic high-dose human data do not exist); people with significant liver or kidney impairment; people on stimulants, hormone modulators, or experimental metabolic compounds without clinician oversight; competitive athletes subject to WADA testing (ERR agonists fall under WADA class S4.5 metabolic modulators as a class, even though SLU-PP-332 is not separately named).
Clinician oversight
Because SLU-PP-332 has no human safety profile, any research planning that involves human exposure should be done under qualified clinician oversight. PDP does not provide medical advice, and nothing on this page substitutes for individualized clinical evaluation.
SLU-PP-332 Side Effects & Safety
Bottom line: there is no human safety data for SLU-PP-332. No Phase 1 trial has been conducted, no human pharmacokinetic study has been published, and no incidence percentages for human side effects exist. Everything below comes from either mouse studies at preclinical doses or uncontrolled community observations.
Mouse-study observations
In the Billon 2023 and Billon 2024 studies, mice dosed at 25-50 mg/kg IP for up to 28 days showed no overt toxicity, no sickness-related weight loss, no liver-enzyme signal at the doses tested, and no cardiac dysfunction. In the Xu 2024 heart-failure study the compound improved cardiac function rather than worsening it; in the Wang 2023 kidney study it was renoprotective rather than nephrotoxic.
Theoretical and community-reported concerns
Broad tissue exposure
ERR receptors are widely expressed across heart, brain, kidney, liver, adipose tissue, and gut, so systemic pan-ERR agonism is not tissue-selective.
Appetite changes
Some community users report appetite changes, though food intake was not significantly altered in the DIO mouse studies.
Sleep disturbance and stimulation
Informal reports describe a more stimulatory feeling and sleep disruption; no controlled data exist.
Resting heart rate
A subset of community users report increased resting heart rate. There is no controlled human data confirming or quantifying this effect.
Cardiovascular unknowns
Chronic high-dose human data do not exist, even though preclinical agonist data looks cardioprotective in heart-failure models.
Oncology unknowns
ERRα participates in some cancer-metabolism pathways, leaving long-term cancer-risk questions open.
Drug interactions
Hepatic metabolism and CYP-pathway interactions in humans are uncharacterized.
Serious adverse events
No serious adverse events have been reported in any published rodent study of SLU-PP-332 at the doses and durations tested. No long-term toxicology study beyond 12 weeks has been published in any species. Washout in mice appears relatively fast given the short exposure window, but that is an animal-PK inference, not a human fact.
For a cross-class safety comparison, see the PepPal peptide side effects guide.
SLU-PP-332 Timeline & What to Monitor
All timeline numbers below come from mouse studies. None of them have been validated in humans, and individual responses in any research-use setting will vary.
Mouse-Study Timeline Reference
Window
Hours
What Was Measured
Acute aerobic exercise transcriptional signature in skeletal muscle after a single 25 mg/kg IP dose.
Where
Billon 2023.
Window
15 days
What Was Measured
Increased treadmill endurance at 25 mg/kg IP daily.
Where
Billon 2023.
Window
28 days
What Was Measured
Raised oxidative muscle fibers and OXPHOS proteins; ~25-30% fat-mass reduction in DIO mice at 50 mg/kg BID.
Where
Billon 2023 / Billon 2024.
Window
6 weeks
What Was Measured
Improved ejection fraction, reduced fibrosis, and increased survival in pressure-overload heart failure.
Where
Xu 2024.
Window
8 weeks
What Was Measured
Reduced albuminuria, preserved podocin, restored mitochondrial function in aging kidney tissue.
Where
Wang 2023.
| Window | What Was Measured | Where |
|---|---|---|
| Hours | Acute aerobic exercise transcriptional signature in skeletal muscle after a single 25 mg/kg IP dose. | Billon 2023. |
| 15 days | Increased treadmill endurance at 25 mg/kg IP daily. | Billon 2023. |
| 28 days | Raised oxidative muscle fibers and OXPHOS proteins; ~25-30% fat-mass reduction in DIO mice at 50 mg/kg BID. | Billon 2023 / Billon 2024. |
| 6 weeks | Improved ejection fraction, reduced fibrosis, and increased survival in pressure-overload heart failure. | Xu 2024. |
| 8 weeks | Reduced albuminuria, preserved podocin, restored mitochondrial function in aging kidney tissue. | Wang 2023. |
These are mouse endpoints, not human results.
Reasonable monitoring
Resting heart rate and blood pressure
Track baseline and periodic measurements given community reports of heart-rate changes.
Basic metabolic panel and lipid panel
Baseline plus periodic review at 4-week and 8-week marks.
Liver enzymes (ALT, AST)
Hepatic metabolism in humans is uncharacterized; checking baseline and periodic ALT/AST adds a low-cost safety signal.
HbA1c or fasting glucose
Mouse data show improved glucose tolerance; tracking baseline + periodic values is a reasonable research observation.
Stopping or review points should be considered if resting heart rate climbs persistently, sleep is significantly disrupted, or any liver-enzyme or metabolic-panel value moves substantially outside the personal baseline range. None of this is a clinical protocol — it is a research-monitoring sketch.
SLU-PP-332 Clinical Evidence Context
Human evidence: none. As of June 2026 there is no registered or completed human clinical trial for SLU-PP-332 on ClinicalTrials.gov.
Billon 2023 (ACS Chemical Biology)
Preclinical in vivo, 15-28 days, C57BL/6J mice (n = 8-10 per group). 25 mg/kg IP for 15 days increased treadmill endurance; 50 mg/kg twice daily for 28 days raised oxidative muscle fibers and OXPHOS proteins.
Billon 2024 (Journal of Pharmacology and Experimental Therapeutics)
Preclinical in vivo, 12-28 days, DIO C57BL/6J and ob/ob mice (n = 7-8 per group). 50 mg/kg twice daily reduced fat mass, lowered cholesterol and triglycerides, reduced adipocyte size, and improved glucose tolerance.
Xu 2024 (Circulation)
Preclinical in vivo, 6 weeks, C57BL/6J mice, pressure-overload TAC heart-failure model. Improved ejection fraction, reduced fibrosis, and increased survival; effects mediated mainly via ERRγ in cardiomyocytes.
Wang 2023 (American Journal of Pathology)
Preclinical in vivo, 8 weeks, aged mice, aging-kidney model. 25 mg/kg/day reduced albuminuria, preserved podocin, reversed mitochondrial dysfunction and inflammation.
Human-trial gap
No registered or completed human clinical trial as of June 2026 per ClinicalTrials.gov. All efficacy claims circulating for SLU-PP-332 in humans rely on mouse-to-human extrapolation.
For context, the fat-mass reductions reported in Billon 2024 — roughly 25-30% in diet-induced obese mice over 28 days without exercise — are large for a preclinical metabolic agent and explain why the "exercise mimetic" label stuck. Until human PK and safety data exist, all efficacy claims should be treated as mouse-only.
SLU-PP-332 Storage & Handling
SLU-PP-332 is a small molecule rather than a peptide, so it is generally more stable than fragile lyophilized peptides at ambient conditions. Storage still depends on whether you are holding dry powder, a BAC-water solution, oral tablets, or a laboratory DMSO stock.
Storage Reference
State
Lyophilized powder (vial)
Storage
-4°F (-20°C) long-term, or 35.6-46.4°F (2-8°C)
Duration
Months at 2-8°C; longer at -20°C per supplier label.
State
Reconstituted solution (vial)
Storage
35.6-46.4°F (2-8°C), protect from light
Duration
Typically 2-4 weeks.
State
Oral tablets (sealed bottle)
Storage
Cool, dry room temperature, away from light and humidity
Duration
Per supplier expiration on the bottle.
State
DMSO stock solution (lab)
Storage
-112°F (-80°C) ideal; -4°F (-20°C) acceptable
Duration
Up to 6 months at -80°C or ~1 month at -20°C.
| State | Storage | Duration |
|---|---|---|
| Lyophilized powder (vial) | -4°F (-20°C) long-term, or 35.6-46.4°F (2-8°C) | Months at 2-8°C; longer at -20°C per supplier label. |
| Reconstituted solution (vial) | 35.6-46.4°F (2-8°C), protect from light | Typically 2-4 weeks. |
| Oral tablets (sealed bottle) | Cool, dry room temperature, away from light and humidity | Per supplier expiration on the bottle. |
| DMSO stock solution (lab) | -112°F (-80°C) ideal; -4°F (-20°C) acceptable | Up to 6 months at -80°C or ~1 month at -20°C. |
Protect reconstituted solutions from light, avoid freeze-thaw cycles, and keep oral tablets in a cool, dry, dark location.
What if my reconstituted vial turns yellow?
Some users notice a yellow tint in reconstituted SLU-PP-332 solution. A faint pale-yellow color can occur with small-molecule compounds in aqueous solution, but a deepening yellow shade often indicates oxidation or degradation from light or temperature excursions. If the color shifts noticeably from the initial appearance, treat the vial as potentially degraded and consult the supplier for guidance rather than continuing use. Formal stability data for community reconstitution conditions has not been published.
SLU-PP-332 Protocol Mistakes & Troubleshooting
- 01
Missed an oral dose
Community oral protocols typically skip the missed dose rather than doubling up. There is no published human half-life that would justify a precise catch-up rule.
- 02
Cloudy or particulate vial after reconstitution
Stop using the vial. Confirm you reconstituted with bacteriostatic water (not plain saline), inspect under good light, and consult the supplier if particulates persist after gentle swirling.
- 03
Wrong BAC water volume added
Recalculate the actual concentration using the reconstitution math (total mcg ÷ total mL = mcg/mL). Adjust draw volume accordingly, or discard and start over with a new vial if the math is hard to reconcile.
- 04
Dose feels too strong
Stop and reassess. Compare the calculated draw against the reconstitution table for that exact vial size and BAC water volume. Many overdose situations come from misreading U-100 syringe markings.
- 05
Injection-site reaction (injectable route)
Rotate sites, confirm sterile technique with two swabs (vial stopper and skin), and check that the syringe was new and unbroken. Persistent reactions warrant pausing and consulting a qualified clinician.
- 06
Vial turned yellow
Treat as potentially degraded. See the storage section for context. Replace rather than push through unknown stability.
- 07
Confused which format to use
Oral tablets need no reconstitution and use bottle math. Injection vials need BAC water and use syringe-unit math. Do not mix instructions across the two formats.
When to seek qualified medical care
Chest pain, persistent palpitations, fainting, severe injection-site infection, or any symptom that feels urgent: stop the protocol and seek qualified medical care. PDP cannot give emergency guidance.
SLU-PP-332 Regulatory Status
As of June 2026, SLU-PP-332 is not approved by the FDA, EMA, or any other major regulator for any human indication. It is sold by research suppliers under research-use-only terms and is not intended for human consumption.
FDA
Not approved. No human IND or NDA has been publicly filed for SLU-PP-332 as of June 2026.
ClinicalTrials.gov
No registered or completed human clinical trial for SLU-PP-332 as of June 2026.
WADA
Not named explicitly in the WADA prohibited list, but ERR agonists fall under WADA class S4.5 metabolic modulators as a class. Competitive athletes subject to WADA testing should treat SLU-PP-332 as prohibited at all times.
Compounding pharmacies
SLU-PP-332 is not currently a compounded product at 503A/503B pharmacies. Community sourcing is via research-use suppliers only.
SLU-PP-332 vs MOTS-c vs AOD-9604
These three compounds are often discussed together because they all show up in metabolic and fat-loss research conversations, but they are not interchangeable. SLU-PP-332 is the nuclear-receptor-level lever, MOTS-c is the mitochondrial peptide with AMPK-linked signaling, and AOD-9604 is a GH-fragment-derived lipolysis tool.
Side-by-Side Reference
Attribute
Class
SLU-PP-332
Synthetic small-molecule pan-ERR agonist
MOTS-c
Mitochondrial-derived peptide (16 aa)
AOD-9604
Modified GH fragment (aa 176-191)
Attribute
Primary target
SLU-PP-332
ERRα / β / γ nuclear receptors
MOTS-c
AMPK activation and mitochondrial signaling
AOD-9604
Lipolysis pathways without GH-receptor signaling
Attribute
Half-life
SLU-PP-332
Not formally published; 6-hour exposure seen in mouse plasma/muscle
MOTS-c
~3 hours (mouse plasma)
AOD-9604
~2-4 hours (rodent data)
Attribute
Dosing frequency
SLU-PP-332
BID preclinical; QD community oral or SC
MOTS-c
Daily SC, often 5 days on / 2 off
AOD-9604
Daily SC
Attribute
Max studied dose
SLU-PP-332
50 mg/kg BID (mouse, 28 days)
MOTS-c
5-15 mg/kg (mouse)
AOD-9604
1-5 mg/day in human Phase 2
Attribute
Peak efficacy signal
SLU-PP-332
~25-30% fat-mass reduction in DIO mice over 28 days
MOTS-c
Improved insulin sensitivity in aged mice
AOD-9604
Modest fat-loss signal in human Phase 2; primary endpoint missed
Attribute
Human route
SLU-PP-332
Oral tablet or SC in community use; no validation
MOTS-c
SC in community use; no human efficacy trials
AOD-9604
SC in clinical trials
Attribute
FDA status
SLU-PP-332
Not approved; no human trials
MOTS-c
Not approved; no native human trials
AOD-9604
Not approved for fat loss; Phase 2 failed primary endpoint
Attribute
Unique advantage
SLU-PP-332
Only pan-ERR agonist with demonstrated in-vivo exercise-mimetic activity
MOTS-c
Endogenous mitochondrial peptide with AMPK-focused signaling
AOD-9604
Most human clinical history of the three
| Attribute | SLU-PP-332 | MOTS-c | AOD-9604 |
|---|---|---|---|
| Class | Synthetic small-molecule pan-ERR agonist | Mitochondrial-derived peptide (16 aa) | Modified GH fragment (aa 176-191) |
| Primary target | ERRα / β / γ nuclear receptors | AMPK activation and mitochondrial signaling | Lipolysis pathways without GH-receptor signaling |
| Half-life | Not formally published; 6-hour exposure seen in mouse plasma/muscle | ~3 hours (mouse plasma) | ~2-4 hours (rodent data) |
| Dosing frequency | BID preclinical; QD community oral or SC | Daily SC, often 5 days on / 2 off | Daily SC |
| Max studied dose | 50 mg/kg BID (mouse, 28 days) | 5-15 mg/kg (mouse) | 1-5 mg/day in human Phase 2 |
| Peak efficacy signal | ~25-30% fat-mass reduction in DIO mice over 28 days | Improved insulin sensitivity in aged mice | Modest fat-loss signal in human Phase 2; primary endpoint missed |
| Human route | Oral tablet or SC in community use; no validation | SC in community use; no human efficacy trials | SC in clinical trials |
| FDA status | Not approved; no human trials | Not approved; no native human trials | Not approved for fat loss; Phase 2 failed primary endpoint |
| Unique advantage | Only pan-ERR agonist with demonstrated in-vivo exercise-mimetic activity | Endogenous mitochondrial peptide with AMPK-focused signaling | Most human clinical history of the three |
Half-life and dose figures across the three compounds are mostly from animal data and should not be read as validated human pharmacology.
If "exercise mimetic" is the research framing, SLU-PP-332 is the class-defining compound. If "mitochondrial signaling in aging" is the framing, MOTS-c is the literature favorite. If "clinical trial history" matters, AOD-9604 is the only one with Phase 2 human data. Worth keeping in the same conversation is Tesamorelin, which works through the GHRH → GH → IGF-1 axis rather than ERR signaling.
SLU-PP-332 Blood Tests & Monitoring
SLU-PP-332 is usually discussed in metabolic, endurance, and exercise-mimetic research. Monitoring focuses on liver/kidney context, glucose, lipids, and muscle-stress markers when training load is relevant.
Blood test markers to discuss with a clinician
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver, kidney, electrolytes, and glucose before interpreting metabolic or endurance changes.
Timing
Baseline
Marker
A1c
Why it matters
Shows longer-term glucose control relevant to metabolic research.
Timing
Baseline
Marker
Lipid panel
Why it matters
Tracks cardiometabolic trends that may shift with body composition or training changes.
Timing
Follow-up
Marker
Creatine kinase (CK)
Why it matters
May help interpret muscle stress when high training load, muscle pain, or statin use is part of the context.
Timing
Optional
Marker
CBC with differential
Why it matters
Adds broad health context before interpreting fatigue or performance changes.
Timing
Baseline
| Marker | Why it matters | Timing |
|---|---|---|
| Comprehensive metabolic panel (CMP) | Reviews liver, kidney, electrolytes, and glucose before interpreting metabolic or endurance changes. | Baseline |
| A1c | Shows longer-term glucose control relevant to metabolic research. | Baseline |
| Lipid panel | Tracks cardiometabolic trends that may shift with body composition or training changes. | Follow-up |
| Creatine kinase (CK) | May help interpret muscle stress when high training load, muscle pain, or statin use is part of the context. | Optional |
| CBC with differential | Adds broad health context before interpreting fatigue or performance changes. | Baseline |
Monitoring guidance is pathway-based and cautious because SLU-PP-332 has limited human monitoring data.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with liver disease, kidney disease, diabetes risk, statin use, or high-intensity training.
Follow-up
Repeat metabolic markers after 8-12 weeks or sooner if fatigue, muscle pain, or exercise tolerance changes sharply.
Longer term
For longer protocols, review metabolic and muscle-stress context every 3-6 months with a clinician.
How to interpret the labs
- Routine labs do not prove improved endurance or mitochondrial function.
- Training, nutrition, sleep, stimulant use, and medications can strongly affect performance and CK.
- Liver and kidney context matter for research compounds without mature human safety data.
Do not wait for routine labs
Severe muscle pain, dark urine, fainting, chest pain, or severe weakness needs medical review.
FAQ
Q1: What is SLU-PP-332 and what is it commonly researched for?
SLU-PP-332 is a synthetic small-molecule pan-ERR agonist developed in the Thomas Burris lab. It activates the same nuclear receptors that endurance exercise activates, which is why it is often described as an exercise mimetic. Published mouse studies report increased treadmill endurance, fat-mass reduction in obese mice, improved cardiac function in heart-failure models, and reduced inflammation in aging-kidney models. Despite the 'peptide' label used in many product listings, SLU-PP-332 is not a peptide — it is a small organic molecule.
Q2: What is the starting dose of SLU-PP-332?
There is no human-validated starting dose. Published murine studies used 25-50 mg/kg intraperitoneal injection once or twice daily. Two community patterns circulate for humans: a low-dose oral pattern (250 mcg to ~1.5 mg once daily) using small-strength vendor capsules, and a higher pattern anchored to the supplier's 50 mg tablet (1 tablet daily). A separate high-dose extrapolation lands near 650 mg/day based on mouse-to-human allometric scaling, but no human has been studied at any dose. None of these are dosing recommendations.
Q3: How are SLU-PP-332 tablets typically dosed?
The current featured supplier carries SLU-PP-332 as a 50 mg oral tablet in a 60-tablet bottle. Community oral protocols range from a 25 mg split-tablet pattern to a 50 mg or 100 mg daily pattern. Oral bioavailability in humans has not been formally published, so any tablet dose is a community pattern, not a clinically validated dose. See the PepPal supplier rankings for broader sourcing context.
Q4: What is the difference between SLU-PP-332 tablets and injectable vials?
Tablets are easier to handle, need no reconstitution, and dose by bottle and tablet count. Injectable vials are the format used in every published animal study, but those used intraperitoneal injection in mice — not subcutaneous injection in humans. Community injectable users reconstitute a 5 mg or 10 mg vial with bacteriostatic water and inject subcutaneously. Oral bioavailability and pharmacokinetics for SC human administration are not published, so there is no clinical answer to which format is more effective.
Q5: What is SLU-PP-332's half-life?
A formal human pharmacokinetic half-life has not been published. In the Billon 2023 paper, mice given 30 mg/kg IP still showed measurable plasma and muscle concentrations at 6 hours post-injection, which helps explain why twice-daily dosing was used in efficacy studies.
Q6: How do you reconstitute SLU-PP-332 injection vials?
For a 5 mg vial, adding 2 mL of bacteriostatic water gives a 2,500 mcg/mL concentration where a 500 mcg dose equals 20 units on a U-100 insulin syringe. Other vial sizes and concentrations are tabulated in the reconstitution section above. For exact draw volumes, use the Pep Pal reconstitution calculator.
Q7: Is SLU-PP-332 FDA-approved?
No. SLU-PP-332 is not approved by the FDA for any indication. It is sold by research suppliers as a research-use compound. There is no registered or completed human clinical trial program on ClinicalTrials.gov as of June 2026.
Q8: What are the most common side effects of SLU-PP-332?
There is no human side-effect dataset. Published mouse studies did not report overt toxicity, liver-enzyme issues, or sickness-related weight loss at 25-50 mg/kg IP for up to 8 weeks. Community reports describe mild appetite changes, sleep disturbance, and increased resting heart rate in some users, but these are uncontrolled observations.
Q9: Why did my reconstituted SLU-PP-332 turn yellow?
A faint pale-yellow tint can occur with small-molecule compounds in aqueous solution, but a deepening yellow shade often indicates oxidation or degradation from light or temperature excursions. If the color shifts noticeably from the initial appearance, treat the vial as potentially degraded and contact the supplier rather than continuing use. Formal stability data for community reconstitution conditions has not been published.
Q10: How does SLU-PP-332 compare to MOTS-c and AOD-9604?
SLU-PP-332 works at the nuclear-receptor level through ERRα / β / γ. MOTS-c is a mitochondrial-derived peptide with AMPK-linked signaling, and AOD-9604 is a GH-fragment-derived lipolysis compound. SLU-PP-332 has the strongest preclinical exercise-mimetic signature of the three, but zero human clinical data.
Q11: Can SLU-PP-332 be stacked with other compounds like MK-677?
No human study has evaluated SLU-PP-332 in combination with any other compound. Theoretical pairings appear in community discussion, but none are clinically validated, and combining experimental compounds compounds the unknowns. PDP does not provide stacking recommendations involving SLU-PP-332. For broader stacking context, see the PepPal peptide stacking guide.
Q12: What is the maximum dose of SLU-PP-332 studied?
In published mouse studies, 50 mg/kg IP twice daily for 28 days is the highest-dose, longest-duration regimen reported in peer-reviewed literature. Human-equivalent-dose extrapolation from that protocol lands around 650 mg/day for an 80 kg adult, but no human has been studied at any dose in a published trial. This is not a dosing recommendation.
Q13: Is the information on this page medical advice?
No. Everything on this page is educational research context. SLU-PP-332 is a preclinical research compound with no FDA-approved indication and no human trial program. Nothing on this page is intended as a personal dosing recommendation or as treatment guidance. Work with a qualified clinician for individual decisions.
Sources & Research
- 1. Billon C, Sitaula S, Banerjee S, Welch R, Elgendy B, Hegazy L, et al. Synthetic ERRα/β/γ Agonist Induces an ERRα-Dependent Acute Aerobic Exercise Response and Enhances Exercise Capacity. ACS Chemical Biology (2023)
- 2. Billon C, Schoepke E, Avdagic A, Chatterjee A, Butler A, Elgendy B, et al. A Synthetic ERR Agonist Alleviates Metabolic Syndrome. Journal of Pharmacology and Experimental Therapeutics (2024)
- 3. Xu W, Billon C, Li H, Wilderman A, Qi L, Graves A, et al. Novel Pan-ERR Agonists Ameliorate Heart Failure Through Enhancing Cardiac Fatty Acid Metabolism and Mitochondrial Function. Circulation (2024)
- 4. Wang XX, Myakala K, Libby AB, Krawczyk E, Panov J, Jones BA, et al. Estrogen-Related Receptor Agonism Reverses Mitochondrial Dysfunction and Inflammation in the Aging Kidney. American Journal of Pathology (2023)
- 5. MedChemExpress SLU-PP-332 | ERR Agonist product data sheet. MedChemExpress (2024)
- 6. Cayman Chemical SLU-PP-332 product data sheet (CAS 303760-60-3). Cayman Chemical (2024)
- 7. Shahien M, Elgendy B, Hegazy L, Patouret R, Walker JK, Burris TP. Development of synthetic agonists of estrogen-related receptors (ERRs) based on an aniline-based pan-agonist scaffold. Journal of Medicinal Chemistry (precursor scaffold context) (2023)
- 8. Frontiers in Physiology editorial team Targeting ERRs to counteract age-related muscle atrophy associated with physical inactivity: a pilot study. Frontiers in Physiology (2025)
- 9. Nasri H. New hopes on 'SLU-PP-332' as an effective agent for weight loss with indirect kidney protection efficacy; a nephrology point of view. Journal of Renal Endocrinology (2024)
- 10. PubChem PubChem entry for SLU-PP-332 (CAS 303760-60-3). PubChem / NCBI (2024)
- 11. ClinicalTrials.gov Registry search for 'SLU-PP-332' confirming no registered or completed human trials. ClinicalTrials.gov (2026)
- 12. World Anti-Doping Agency WADA Prohibited List — class S4.5 metabolic modulators (ERR agonists as a class). WADA (2026)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page