MOTS-c Quick Start
MOTS-c is short for mitochondrial open reading frame of the 12S rRNA-c. It is a 16-amino-acid peptide that your mitochondria make on their own. Mitochondria are the parts of cells that turn food and oxygen into energy.
Researchers study MOTS-c because it acts like a chemical signal. It tells cells how to handle energy when the body is stressed, exercising, or aging. The most studied effect is that it turns on a protein called AMPK, which is a key energy switch inside cells.
This page is a research-planning reference. It covers the protocol structure most often discussed for MOTS-c, simple reconstitution math, and what the published evidence does and does not show. It is not medical advice.
Route
Subcutaneous injection (under the skin) is the format used in animal studies and reported research planning.
Schedule
Common research planning: 5 mg, 2 to 3 times per week, for 4 to 8 weeks.
Measure
Reconstitute a 10 mg vial with 1.0 mL bacteriostatic water. A 5 mg dose is 0.5 mL, which is 50 units on a U-100 insulin syringe.
Supplies
Per dose you need one vial (shared across two doses), one syringe, two alcohol swabs, and a small amount of bacteriostatic water.
Research status
MOTS-c is not FDA-approved. As of April 22, 2026 it is no longer in FDA Category 2, but it has not been added to the 503A Bulks List. WADA bans it at all times.
Disclaimer
This page is an educational research reference and is not medical advice. MOTS-c is not FDA-approved for human use. Talk with a qualified healthcare provider before making any health decisions.
This page handles MOTS-c dose steps, vial math, timing, and storage. Want the deeper science view? Read the MOTS-c research guide. It covers cell energy, key studies, safety notes, and comparisons.
MOTS-c Dosing Protocol & Schedule
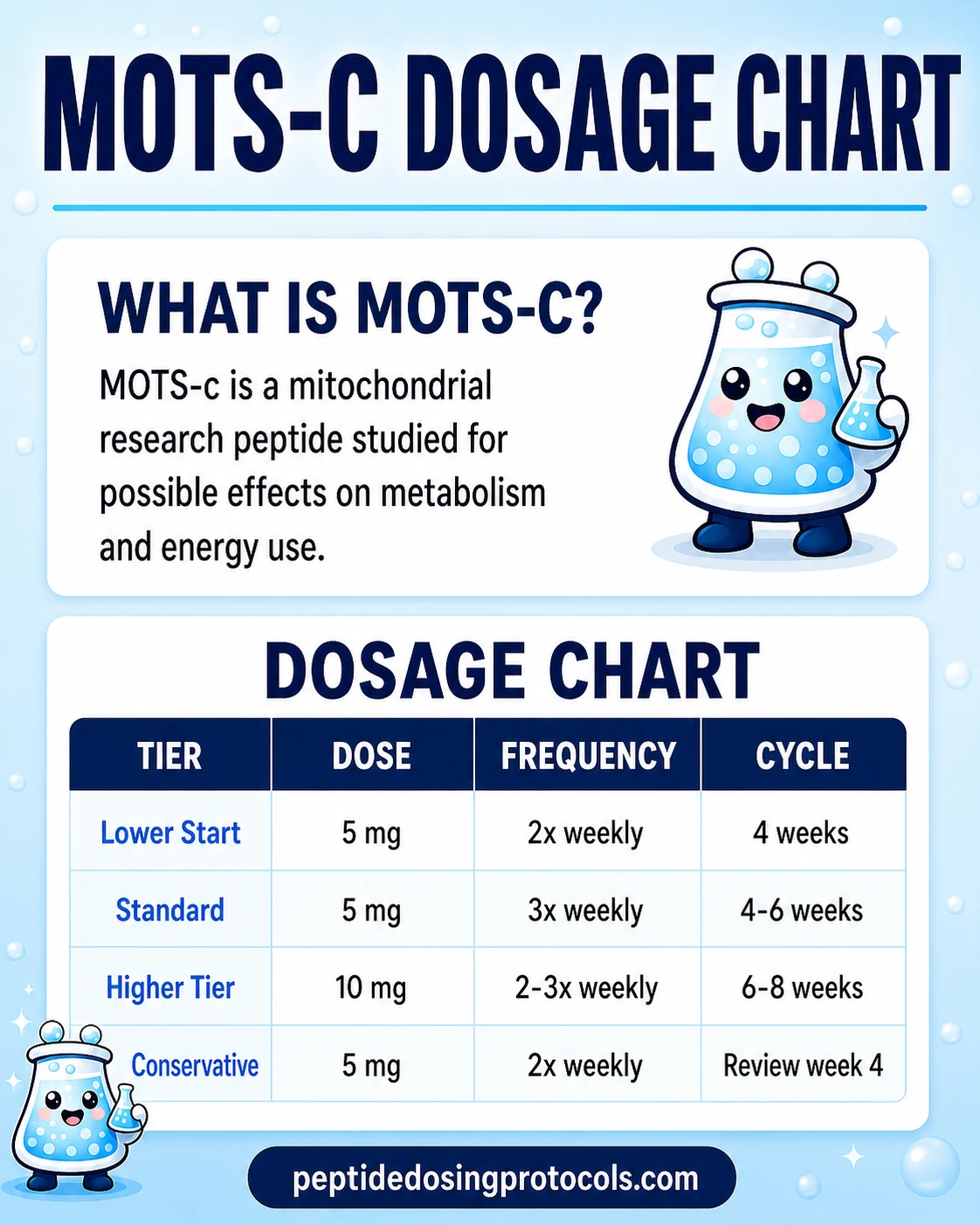
The MOTS-c dosing pattern most often discussed in research planning is 5 mg subcutaneously, 2 to 3 times per week, for 4 to 8 weeks. There is no FDA-approved label for MOTS-c, so this is not a clinical dose. It is the dose range repeatedly cited in community protocols and clinic literature, summarized here for reference only.
Smaller, more frequent doses are often described as a way to keep AMPK signaling steadier, since the peptide has a short estimated half-life. Larger weekly totals do not appear to add benefit in the published animal work and may push side effects higher.
MOTS-c Dosage Chart
MOTS-c research-planning dose tiers
Tier
Lower-end starting tier
Dose
5 mg
Frequency
2x per week
Cycle length
4 weeks
Notes
Used by researchers checking tolerance and histamine response.
Tier
Standard tier
Dose
5 mg
Frequency
3x per week
Cycle length
4-6 weeks
Notes
Most common research-planning anchor for steady AMPK signaling.
Tier
Higher tier
Dose
10 mg
Frequency
2-3x per week
Cycle length
6-8 weeks
Notes
Reported in the upper end of community protocols. Side effects and quality risk rise with dose.
| Tier | Dose | Frequency | Cycle length | Notes |
|---|---|---|---|---|
| Lower-end starting tier | 5 mg | 2x per week | 4 weeks | Used by researchers checking tolerance and histamine response. |
| Standard tier | 5 mg | 3x per week | 4-6 weeks | Most common research-planning anchor for steady AMPK signaling. |
| Higher tier | 10 mg | 2-3x per week | 6-8 weeks | Reported in the upper end of community protocols. Side effects and quality risk rise with dose. |
These tiers summarize community and clinic-reported research planning. None of them have been validated in a published human randomized trial. This is not a dosing recommendation. For protocol-focused research, also see Peptide Dosing Protocols.
Cycle Guidelines
Approach
Conservative
Duration
4 weeks
Off period
4 weeks
Best for
First-time tolerance review.
Approach
Standard
Duration
6 weeks
Off period
4-6 weeks
Best for
Most published animal protocols and community references.
Approach
Extended
Duration
8 weeks
Off period
6-8 weeks
Best for
Used in research planning that tracks endpoints over a longer block.
| Approach | Duration | Off period | Best for |
|---|---|---|---|
| Conservative | 4 weeks | 4 weeks | First-time tolerance review. |
| Standard | 6 weeks | 4-6 weeks | Most published animal protocols and community references. |
| Extended | 8 weeks | 6-8 weeks | Used in research planning that tracks endpoints over a longer block. |
Cycling is reported as a way to limit AMPK downregulation and to give a clean off-window for reviewing markers. There is no published human trial that has compared cycle lengths directly.
Where the dose ranges come from
These tiers are summarized from animal studies (Reynolds 2021, Lee 2015, Kumagai 2021), the WADA monograph, and the clinic-provider language reported in Innerbody's MOTS-c review. No FDA-approved MOTS-c label exists.
MOTS-c Supplies Needed
Plan based on a 10 mg MOTS-c vial reconstituted with 1.0 mL bacteriostatic water. At 5 mg per dose, one vial covers two doses. The math below assumes 5 mg, 2 times per week. Add one vial per week if planning 3 doses per week instead.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

MOTS-c 40mg Supply

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
MOTS-c Vials (10 mg each)
One 10 mg vial covers two 5 mg doses. Plan one vial per week at 2x weekly.
| Cycle length | Planning note |
|---|---|
4 weeks 4 vials | 8 doses needed; one vial per week. |
6 weeks 6 vials | 12 doses needed; one vial per week. |
8 weeks 8 vials | 16 doses needed; one vial per week. |
4 weeks
4 vials
8 doses needed; one vial per week.
6 weeks
6 vials
12 doses needed; one vial per week.
8 weeks
8 vials
16 doses needed; one vial per week.
Insulin Syringes (U-100)
Use 1 mL / 100-unit U-100 insulin syringes since a 5 mg dose draws 0.5 mL (50 units).
| Cycle length | Planning note |
|---|---|
4 weeks 8 syringes | 1 syringe per injection. |
6 weeks 12 syringes | 1 syringe per injection. |
8 weeks 16 syringes | 1 syringe per injection. |
4 weeks
8 syringes
1 syringe per injection.
6 weeks
12 syringes
1 syringe per injection.
8 weeks
16 syringes
1 syringe per injection.
Bacteriostatic Water
Use 1.0 mL per 10 mg vial for a 10 mg/mL concentration.
| Cycle length | Planning note |
|---|---|
4-8 weeks 1 x 10 mL bottle | 4 weeks: 4 vials use 4 mL total; one bottle gives margin.; 6 weeks: 6 vials use 6 mL total; one bottle gives margin.; 8 weeks: 8 vials use 8 mL total; one bottle is enough. |
4-8 weeks
1 x 10 mL bottle
4 weeks: 4 vials use 4 mL total; one bottle gives margin.; 6 weeks: 6 vials use 6 mL total; one bottle gives margin.; 8 weeks: 8 vials use 8 mL total; one bottle is enough.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments. At 3 doses per week, add one vial, two more swabs, and one more syringe per week to the totals above.
Companion Supplies & Routine Support
MOTS-c Dosage Chart
This MOTS-c dosage chart summarizes the research-planning tiers from 5 mg to 10 mg, two to three times weekly shown in the dosing section above.
MOTS-c Reconstitution Guide
Reconstitution means mixing the dry MOTS-c powder with bacteriostatic water so it becomes a liquid you can draw into a syringe. The math below uses a 10 mg vial because that is the most common size for research-grade MOTS-c.
MOTS-c reconstitution math (10 mg vial)
Step
Vial size
Value
10 mg
Why it matters
The starting amount of peptide in the vial.
Step
BAC water added
Value
1.0 mL
Why it matters
Sets the final concentration. More water means a weaker mix per mL.
Step
Final concentration
Value
10 mg/mL
Why it matters
Each 1 mL of liquid carries 10 mg of MOTS-c.
Step
5 mg dose volume
Value
0.5 mL
Why it matters
Half a milliliter of liquid for one 5 mg dose.
Step
5 mg dose in syringe units
Value
50 units (U-100)
Why it matters
Standard U-100 insulin syringes show 100 units = 1 mL, so 50 units = 0.5 mL.
| Step | Value | Why it matters |
|---|---|---|
| Vial size | 10 mg | The starting amount of peptide in the vial. |
| BAC water added | 1.0 mL | Sets the final concentration. More water means a weaker mix per mL. |
| Final concentration | 10 mg/mL | Each 1 mL of liquid carries 10 mg of MOTS-c. |
| 5 mg dose volume | 0.5 mL | Half a milliliter of liquid for one 5 mg dose. |
| 5 mg dose in syringe units | 50 units (U-100) | Standard U-100 insulin syringes show 100 units = 1 mL, so 50 units = 0.5 mL. |
If you use 2.0 mL of BAC water instead, the concentration drops to 5 mg/mL and a 5 mg dose becomes 1.0 mL (100 units). Both are valid; 1.0 mL gives cleaner draw math on a U-100 syringe.
- 01
Inspect the vial
Confirm the vial label, the listed peptide amount, and the appearance of the powder. The lyophilized powder should look like a small white plug or fine cake.
- 02
Wipe the stoppers
Wipe both the bacteriostatic water vial and the MOTS-c vial stoppers with a fresh alcohol swab.
- 03
Draw the bacteriostatic water
Pull 1.0 mL of bacteriostatic water into a syringe.
- 04
Add water slowly
Insert the needle into the MOTS-c vial and let the water trickle down the inside wall of the vial. Do not blast it directly onto the powder.
- 05
Swirl gently
Swirl the vial in slow circles until the powder dissolves. Do not shake. Shaking can damage the peptide.
- 06
Check the solution
The liquid should look clear and free of particles. If it is cloudy or has visible specks, do not use it.
- 07
Refrigerate and label
Refrigerate the reconstituted vial at 36-46F (2-8C). Note the date you reconstituted it on the label.
Use a calculator
If your vial size or BAC water volume is different from the example above, use a peptide reconstitution calculator. Different vial sizes change the dose volume and the syringe units, so do not copy numbers from a chart that does not match your vial.
How MOTS-c Works
MOTS-c is encoded by mitochondrial DNA, not the DNA in the cell nucleus. That makes it part of a small group called mitochondria-derived peptides. Your body makes more of it during exercise and physical stress, and levels drop with age.
The most studied effect is AMPK activation. AMPK is an enzyme that acts like an energy switch. When AMPK turns on, cells take in more glucose, burn more fat for fuel, and build more mitochondria over time.
Lee and colleagues described this pattern in a 2015 paper in Cell Metabolism using mouse and cell models. The authors compared the metabolic profile to the diabetes drug metformin, but stopped short of saying the two are interchangeable.
Reynolds and colleagues then showed in a 2021 Nature Communications paper that MOTS-c improved running capacity in young, middle-aged, and older mice, which is why some clinic and community sources call it an exercise-mimetic. That label overstates the human evidence: no published human randomized trial has reproduced the running-capacity effect.
Who MOTS-c Is For and Who Should Avoid It
MOTS-c is studied in metabolic health, exercise performance, and aging research. None of those uses have been approved by the FDA. The list below is research-planning context, not a treatment recommendation.
Often researched in
- Glucose handling and insulin-sensitivity research, anchored to the Lee 2015 Cell Metabolism paper.
- Exercise capacity and aging research, anchored to the Reynolds 2021 Nature Communications paper.
- Bone metabolism research, summarized in the Yi 2023 Frontiers in Physiology review.
- Inflammation research, anchored to the Zhe 2024 Neurological Research paper on inflammatory pain models.
Should avoid or hold off
- Anyone with an active cancer diagnosis, since MOTS-c effects on tumor biology are mixed in the literature and clinician sources cited by Innerbody recommend caution.
- Pregnant or breastfeeding individuals, because there is no human safety data.
- People taking other AMPK-activating drugs such as metformin, thiazolidinediones, or aspirin without prescriber input, because of theoretical overlap.
- Athletes subject to drug testing under WADA rules, since MOTS-c is prohibited at all times under section S4.4.1.
- Anyone who would not have access to a clinician if a side effect appeared.
MOTS-c Side Effects & Safety
There is no large human safety database for MOTS-c. The closest published human safety data is for CB4211, a synthetic MOTS-c analog that completed a Phase 1 trial and was reported as well tolerated. That is similar but not the same molecule, so the read-across is limited.
The U.S. Anti-Doping Agency monograph and clinician sources cited by Innerbody describe a small, mostly mild side-effect pattern in people who buy MOTS-c online.
Reported MOTS-c side effects
Side effect
Injection site redness or swelling
Frequency reported
Common
What to do
Rotate sites, inject slowly.
Side effect
Flushing or skin warmth (histamine response)
Frequency reported
Occasional
What to do
Inject more slowly; consider lower dose for the first few sessions.
Side effect
Headache
Frequency reported
Occasional
What to do
Stay hydrated; reduce dose if persistent.
Side effect
Mild fatigue after dose
Frequency reported
Occasional
What to do
Lower dose or move dose to morning.
Side effect
Heart palpitations
Frequency reported
Reported by USADA
What to do
Stop and seek qualified medical input.
Side effect
Insomnia or fever
Frequency reported
Reported by USADA
What to do
Stop and seek qualified medical input.
| Side effect | Frequency reported | What to do |
|---|---|---|
| Injection site redness or swelling | Common | Rotate sites, inject slowly. |
| Flushing or skin warmth (histamine response) | Occasional | Inject more slowly; consider lower dose for the first few sessions. |
| Headache | Occasional | Stay hydrated; reduce dose if persistent. |
| Mild fatigue after dose | Occasional | Lower dose or move dose to morning. |
| Heart palpitations | Reported by USADA | Stop and seek qualified medical input. |
| Insomnia or fever | Reported by USADA | Stop and seek qualified medical input. |
Reports are drawn from the USADA MOTS-c monograph and clinician sources cited in Innerbody's MOTS-c review. They are not from a randomized human trial.
Theoretical risks
- Cancer signaling. Some preclinical work shows MOTS-c slowing certain tumor lines (Yin 2024 ovarian cancer model). Other sources cited by Innerbody flag possible risk in prostate and breast cancer settings. Direction of effect is not settled, so an active cancer diagnosis is a hold reason.
- AMPK overlap. People on metformin, aspirin, or thiazolidinediones may layer AMPK activation, with unknown net effect.
- Quality variability. Research-grade peptides can include impurities. Immunogenicity (an unwanted immune reaction) is a stated risk in FDA materials on protein-based therapeutics.
MOTS-c Timeline & What to Monitor
MOTS-c does not produce a noticeable acute effect like a stimulant. The shifts described in clinic and community sources are slow and small. Innerbody's clinician sources describe steadier energy in the first 1-2 weeks and possible exercise-tolerance changes by weeks 4-6.
Common reporting windows
Window
Week 1-2
What is reported
Steadier daytime energy is reported in clinic literature.
What to track
Subjective energy notes; sleep timing.
Window
Week 3-4
What is reported
Workout tolerance and recovery are described as smoother.
What to track
Workout logs; recovery feel.
Window
Week 4-6
What is reported
Body-composition shifts described in animal protocols may begin to show up in humans, though without published RCT confirmation.
What to track
Waist circumference; bodyweight trend; fasting glucose if available.
Window
End of cycle
What is reported
Reasonable point to stop and review.
What to track
Compare baseline notes to end-of-cycle notes; do not extend without a review.
| Window | What is reported | What to track |
|---|---|---|
| Week 1-2 | Steadier daytime energy is reported in clinic literature. | Subjective energy notes; sleep timing. |
| Week 3-4 | Workout tolerance and recovery are described as smoother. | Workout logs; recovery feel. |
| Week 4-6 | Body-composition shifts described in animal protocols may begin to show up in humans, though without published RCT confirmation. | Waist circumference; bodyweight trend; fasting glucose if available. |
| End of cycle | Reasonable point to stop and review. | Compare baseline notes to end-of-cycle notes; do not extend without a review. |
Track what you can measure rather than what you can feel. Energy and recovery are subjective and easy to misread without a control.
MOTS-c is not a diagnostic tool. Markers like fasting glucose, A1C, and body composition can move for many reasons. Use them to look for trend, not to make medical decisions.
MOTS-c Clinical Evidence Context
Direct human evidence for MOTS-c is limited to a few cross-sectional and small-sample studies. The strongest mechanistic evidence comes from animal and cell research. The closest randomized human safety data is for the synthetic analog CB4211, not for native MOTS-c.
Human evidence (limited)
Domin and colleagues (2023, International Journal of Molecular Sciences) reported that higher serum MOTS-c levels correlated with greater lower-body muscle strength in healthy adults. This is a correlation in one small sample, not a randomized intervention trial.
Phase 1 analog data
CB4211, a synthetic MOTS-c analog, completed a Phase 1a/1b trial reported as safe and well tolerated. The molecule is related but not identical, so this safety signal does not transfer fully to native MOTS-c.
Preclinical evidence (strongest)
Lee and colleagues (2015, Cell Metabolism) showed MOTS-c reduced obesity and insulin resistance in mice on a high-fat diet. Reynolds and colleagues (2021, Nature Communications) showed running capacity improvement across mouse age groups. Kumagai and colleagues (2021, American Journal of Physiology - Endocrinology and Metabolism) reported reduced myostatin and atrophy signaling in mice. Yi and colleagues (2023, Frontiers in Physiology) reviewed bone-metabolism findings.
Mechanism review
Wan and colleagues (2023, Journal of Translational Medicine) and Kong and colleagues (2023, Diabetes & Metabolism Journal) reviewed AMPK activation, mitochondria-to-nucleus signaling, and the link between MOTS-c and aging-related metabolic disease.
Evidence gap
No published human randomized controlled trial has tested native MOTS-c for any clinical endpoint. Treat the dose tiers on this page as research-planning context, not as proof of human benefit.
MOTS-c Storage & Handling
Storage temperatures and stability
State
Lyophilized (Powder Form)
Storage
-4F (-20C) long-term
Notes
Refrigerator (36-46F / 2-8C) is acceptable short-term per supplier label and stability data.
State
Reconstituted (Liquid Form)
Storage
36-46F (2-8C)
Notes
Use within 2-3 weeks per the stability concern flagged by clinic and community sources for MOTS-c specifically.
State
Appearance after mixing
Storage
Clear
Notes
Discard if cloudy or with visible particles.
| State | Storage | Notes |
|---|---|---|
| Lyophilized (Powder Form) | -4F (-20C) long-term | Refrigerator (36-46F / 2-8C) is acceptable short-term per supplier label and stability data. |
| Reconstituted (Liquid Form) | 36-46F (2-8C) | Use within 2-3 weeks per the stability concern flagged by clinic and community sources for MOTS-c specifically. |
| Appearance after mixing | Clear | Discard if cloudy or with visible particles. |
MOTS-c is reported as more sensitive to heat and time than many other research peptides. Keep it cold and use it within the supplier-stated window.
MOTS-c Protocol Mistakes & Troubleshooting
- 01
Missed dose
If you miss a dose by a day, take the next dose on the regular schedule. Do not double-dose. Note the miss in your log.
- 02
Cloudy or speckled vial
Do not inject. A cloudy or particulate vial means the peptide may be degraded or the solution may be contaminated. Discard it.
- 03
Wrong BAC water volume
If you used 2.0 mL instead of 1.0 mL, your concentration dropped to 5 mg/mL. A 5 mg dose then becomes 1.0 mL (100 units), not 0.5 mL (50 units). Recalculate before drawing.
- 04
Strong flushing or itching
MOTS-c can trigger histamine release. Inject slower, drop to the lower-end dose tier for the next session, and if symptoms persist, stop and seek qualified medical input.
- 05
Injection-site reaction
A small red mark for a few hours is common. Persistent swelling, hardness, or warmth lasting more than 48 hours is a stop signal.
- 06
Storage mistake
If a reconstituted vial sat at room temperature for more than a few hours, treat it as compromised. Do not inject older or warm-stored MOTS-c.
- 07
Confusion about the schedule
MOTS-c is dosed 2-3 times per week, not daily. Daily dosing is associated with a different protocol (1 mg) seen in one community source and is not the dominant pattern in published animal work.
If something feels wrong
Stop dosing and contact a qualified healthcare provider. This page does not cover medical emergencies.
MOTS-c Regulatory Status
MOTS-c is not FDA-approved for any human use as of June 2026. Research-grade vials sold in the U.S. are labeled for laboratory and research use only.
FDA 503A timeline
- Late 2023: FDA placed MOTS-c on Category 2 of its 503A bulks list, the category for substances flagged for significant safety concerns.
- February 27, 2026: HHS Secretary Robert F. Kennedy Jr. publicly stated an intent to move 14 of the 19 Category 2 peptides back to Category 1. A statement is not a rule change.
- April 15, 2026: FDA announced removal of 12 peptides from Category 2, including MOTS-c, because the original nominators withdrew their nominations.
- April 22, 2026 (effective date): Removal from Category 2 took effect. Removal from Category 2 does not make a substance Category 1, and it does not add the substance to the 503A Bulks List.
- July 23, 2026 (scheduled): Pharmacy Compounding Advisory Committee meeting to discuss MOTS-c (free base and acetate forms) for 503A Bulks List inclusion.
Practical effect: as of June 2026, MOTS-c is not legally compoundable as a Category 1 substance, has been removed from Category 2, and is awaiting PCAC review. The status can change after July 23, 2026. Verify the current FDA list before assuming legality.
WADA / sports testing
MOTS-c is named explicitly on the 2026 WADA Prohibited List under section S4.4.1 (AMPK activators) and is prohibited at all times. Any athlete subject to anti-doping testing should not use MOTS-c.
MOTS-c vs Tesamorelin vs SS-31
MOTS-c is one of several peptides that gets discussed in metabolic and longevity research. The closest comparators are tesamorelin (a GHRH analog with FDA approval for HIV-related fat) and SS-31 (a separate mitochondrial peptide that targets cardiolipin rather than AMPK). For the telomere and pineal-gland side of longevity research, compare against Epithalon. For senolytic research rather than AMPK or mitochondrial signaling, compare against FOXO4-DRI. If you are comparing MOTS-c with incretin-based weight and metabolic research instead, start with the Retatrutide protocol.
MOTS-c vs nearby peptides
Peptide
MOTS-c
Main mechanism
Mitochondria-derived AMPK activator.
Typical research context
Metabolic flexibility, exercise capacity, aging research.
Regulatory status
Not FDA-approved; WADA banned at all times.
Peptide
Tesamorelin
Main mechanism
GHRH analog that raises growth hormone release.
Typical research context
FDA-approved for HIV-associated visceral fat; community use for body composition.
Regulatory status
FDA-approved for one indication. See Tesamorelin protocol.
Peptide
SS-31
Main mechanism
Targets cardiolipin in the inner mitochondrial membrane.
Typical research context
Mitochondrial repair and ischemia research.
Regulatory status
Not FDA-approved. See SS-31 protocol.
Peptide
Metformin (drug, not peptide)
Main mechanism
AMPK activator, among other effects.
Typical research context
FDA-approved for type 2 diabetes; widely studied for healthy aging.
Regulatory status
FDA-approved prescription drug.
| Peptide | Main mechanism | Typical research context | Regulatory status |
|---|---|---|---|
| MOTS-c | Mitochondria-derived AMPK activator. | Metabolic flexibility, exercise capacity, aging research. | Not FDA-approved; WADA banned at all times. |
| Tesamorelin | GHRH analog that raises growth hormone release. | FDA-approved for HIV-associated visceral fat; community use for body composition. | FDA-approved for one indication. See Tesamorelin protocol. |
| SS-31 | Targets cardiolipin in the inner mitochondrial membrane. | Mitochondrial repair and ischemia research. | Not FDA-approved. See SS-31 protocol. |
| Metformin (drug, not peptide) | AMPK activator, among other effects. | FDA-approved for type 2 diabetes; widely studied for healthy aging. | FDA-approved prescription drug. |
MOTS-c and metformin share an AMPK link but are not interchangeable. Tesamorelin works through growth hormone, not AMPK.
MOTS-c Blood Tests & Monitoring
MOTS-c is usually discussed in mitochondrial and metabolic research. Monitoring focuses on glucose, lipids, liver/kidney context, and muscle-stress context when training intensity is high.
Blood test markers to discuss with a clinician
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver, kidney, electrolytes, and glucose before interpreting energy or metabolic changes.
Timing
Baseline
Marker
A1c
Why it matters
Shows longer-term glucose control relevant to metabolic research.
Timing
Baseline
Marker
Fasting glucose
Why it matters
Gives a current glucose snapshot during metabolic or training changes.
Timing
Follow-up
Marker
Lipid panel
Why it matters
Tracks cardiometabolic trends during body-composition or metabolic protocols.
Timing
Follow-up
Marker
Creatine kinase (CK)
Why it matters
May help interpret muscle stress when intense training, muscle pain, or statin use is part of the context.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| Comprehensive metabolic panel (CMP) | Reviews liver, kidney, electrolytes, and glucose before interpreting energy or metabolic changes. | Baseline |
| A1c | Shows longer-term glucose control relevant to metabolic research. | Baseline |
| Fasting glucose | Gives a current glucose snapshot during metabolic or training changes. | Follow-up |
| Lipid panel | Tracks cardiometabolic trends during body-composition or metabolic protocols. | Follow-up |
| Creatine kinase (CK) | May help interpret muscle stress when intense training, muscle pain, or statin use is part of the context. | Optional |
Monitoring guidance is mitochondrial and metabolic pathway-based because MOTS-c has limited established clinical monitoring standards.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with diabetes risk, kidney disease, liver disease, statin use, or intense training.
Follow-up
Repeat metabolic markers after 8-12 weeks or sooner if training load, fatigue, or symptoms change.
Longer term
For longer protocols, review trends every 3-6 months with a clinician.
How to interpret the labs
- Routine labs do not directly prove mitochondrial improvement.
- Training load, sleep, nutrition, and medications can strongly affect energy and metabolic labs.
- CK is most useful when muscle symptoms or unusually high training stress are present.
Do not wait for routine labs
Severe muscle pain, dark urine, chest pain, fainting, confusion, or severe weakness needs medical review.
FAQ
Q1: What is MOTS-c?
MOTS-c is a 16-amino-acid peptide encoded by mitochondrial DNA. It activates AMPK, an enzyme that controls how cells use energy. The body makes more of it during exercise, and levels drop with age. It is not FDA-approved for human use.
Q2: What is MOTS-c commonly researched for?
MOTS-c is studied in metabolic health, exercise capacity, body composition, aging, bone metabolism, and inflammation. Most published evidence is from animal and cell models, with limited cross-sectional human data.
Q3: How is MOTS-c commonly dosed in research planning?
Common research-planning anchor is 5 mg subcutaneous, 2 to 3 times per week, in 4 to 8 week cycles. Lower-end planning is 5 mg twice weekly, higher-end is 10 mg two to three times weekly. None of these have been validated in a published human randomized trial. This is not a dosing recommendation.
Q4: What is the standard MOTS-c dosage chart?
Three tiers are commonly cited: a starting tier of 5 mg twice weekly for 4 weeks, a standard tier of 5 mg three times weekly for 4-6 weeks, and a higher tier of 10 mg two to three times weekly for 6-8 weeks. See the dosage chart table on this page for context. For a deeper dosing reference, also see Peptide Dosing Protocols.
Q5: How is MOTS-c reconstituted?
A 10 mg vial reconstituted with 1.0 mL of bacteriostatic water gives a 10 mg/mL concentration. A 5 mg dose is 0.5 mL, which is 50 units on a U-100 insulin syringe. Swirl the vial gently rather than shaking, and refrigerate after mixing.
Q6: How long is a typical MOTS-c cycle?
Cycles described in research planning are 4 to 8 weeks on, with an off period of similar length. Cycling is reported as a way to limit AMPK downregulation. There is no published human trial that has compared cycle lengths directly.
Q7: What are the main side effects of MOTS-c?
Reported side effects include injection-site redness or swelling, flushing or skin warmth (a histamine response), mild fatigue, and headache. The U.S. Anti-Doping Agency monograph also lists heart palpitations, insomnia, and fever in people who buy it online. There is no large human safety database for native MOTS-c.
Q8: Why does MOTS-c sometimes cause flushing?
MOTS-c can trigger mast cell activation, which releases histamine and causes warmth, redness, or itching at or near the injection site. Slower injection and a lower starting dose can reduce it. Persistent reactions are a stop signal.
Q9: Who should avoid MOTS-c?
People with an active cancer diagnosis, anyone pregnant or breastfeeding, athletes subject to WADA testing, and people taking other AMPK-activating drugs (metformin, thiazolidinediones, aspirin) without prescriber input should avoid it. None of these groups have human safety data for MOTS-c.
Q10: How does MOTS-c compare to tesamorelin and SS-31?
MOTS-c works through AMPK and mitochondrial signaling. Tesamorelin works through growth hormone release and is FDA-approved for HIV-associated visceral fat. SS-31 targets the inner mitochondrial membrane through cardiolipin. They are studied for related goals but are not interchangeable.
Q11: Is MOTS-c FDA-approved?
No. MOTS-c is not FDA-approved for any human use as of June 2026. It was removed from FDA Category 2 effective April 22, 2026, and is scheduled for Pharmacy Compounding Advisory Committee discussion on July 23, 2026. Removal from Category 2 does not mean it is approved or that it is on the 503A Bulks List.
Q12: Is MOTS-c banned in sports?
Yes. MOTS-c is named explicitly on the 2026 World Anti-Doping Agency (WADA) Prohibited List under section S4.4.1 (AMPK activators) and is prohibited at all times.
Q13: Is this page medical advice?
No. This page is an educational research reference. It is not medical advice, and it is not a treatment plan. Talk with a qualified healthcare provider before making any health decisions involving MOTS-c.
Sources & Research
- 1. Lee C, Zeng J, Drew BG, et al. The mitochondrial-derived peptide MOTS-c promotes metabolic homeostasis and reduces obesity and insulin resistance. Cell Metabolism (2015)
- 2. Reynolds JC, Lai RW, Woodhead JST, et al. MOTS-c is an exercise-induced mitochondrial-encoded regulator of age-dependent physical decline and muscle homeostasis. Nature Communications (2021)
- 3. Kumagai H, Coelho AR, Wan J, et al. MOTS-c reduces myostatin and muscle atrophy signaling. American Journal of Physiology - Endocrinology and Metabolism (2021)
- 4. Wan W, Zhang L, Lin Y, et al. Mitochondria-derived peptide MOTS-c: effects and mechanisms related to stress, metabolism and aging. Journal of Translational Medicine (2023)
- 5. Kong BS, Lee C, Cho YM. Mitochondrial-encoded peptide MOTS-c, diabetes, and aging-related diseases. Diabetes & Metabolism Journal (2023)
- 6. Domin R, Pytka M, Niziolek-Szynczak A, et al. MOTS-c serum concentration positively correlates with lower-body muscle strength and is not related to maximal oxygen uptake — a preliminary study. International Journal of Molecular Sciences (2023)
- 7. Yi X, Hu G, Yang Y, et al. Role of MOTS-c in the regulation of bone metabolism. Frontiers in Physiology (2023)
- 8. Zhe W, Liu Y, Han P, et al. Central and peripheral mechanism of MOTS-c attenuates pain hypersensitivity in a mice model of inflammatory pain. Neurological Research (2024)
- 9. Yin Y, Pan Y, He J, et al. Mitochondrial-derived peptide MOTS-c suppresses ovarian cancer progression by attenuating USP7-mediated LARS1 deubiquitination. Advanced Science (2024)
- 10. U.S. Anti-Doping Agency. What is the MOTS-c peptide? USADA (2024)
- 11. World Anti-Doping Agency. The 2026 Prohibited List - Section S4.4 Metabolic Modulators (MOTS-c named under AMPK activators). WADA (2026)
- 12. U.S. Food and Drug Administration. Bulk Drug Substances Nominated for Use in Compounding Under Section 503A — MOTS-c removal from Category 2 (effective April 22, 2026); PCAC consultation scheduled July 23, 2026. FDA (2026)
- 13. Alzheimer's Drug Discovery Foundation. MOTS-c — Cognitive Vitality Report (notes CB4211 Phase 1 safety read-across). ADDF (2021)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page