KLOW Peptide Blend Quick Start
KLOW is a research-context name for a four-peptide blend that pairs GHK-Cu (a copper-binding peptide tied to skin and connective-tissue research) with KPV (an anti-inflammatory tripeptide), BPC-157 (a peptide studied in soft-tissue repair models), and TB-500 (a synthetic fragment of thymosin beta-4 used in cell-migration research). The standard vial size discussed in the research community is 80 mg total, with 50 mg GHK-Cu and 10 mg each of KPV, BPC-157, and TB-500.
KLOW is most often compared to the GLOW stack, which has the same three regenerative peptides (GHK-Cu, BPC-157, TB-500) but does not include KPV. The KPV component is what people most commonly point to when they choose KLOW over GLOW.
Reconstitute
Add 3.0 mL bacteriostatic water to the 80 mg vial -> about 26.7 mg/mL total blend.
Easy measuring
1 unit on a U-100 syringe (0.01 mL) is about 267 mcg total: ~167 mcg GHK-Cu + ~33 mcg of each of the other three.
Schedule
Common research planning uses once-daily subcutaneous injection.
Cycle
Typical cycle structure is 4-6 weeks on, 2-4 weeks off; copper accumulation from GHK-Cu is the main driver of the off period.
Research status
Not FDA-approved. No published trial has evaluated the four-peptide KLOW combination together.
Disclaimer
This page is an educational research reference and is not medical advice. KLOW is not an FDA-approved treatment. Information is provided for research-context understanding only.
Use this page for KLOW Stack dose setup, timing, and planning. For the bigger blend picture, read the KLOW Stack overview on compound roles, research, safety notes, and related stacks.
KLOW Peptide Blend Dosing Protocol & Schedule
KLOW dosing planning has two starting points: knowing the blend ratio inside the vial, and knowing the draw volume that delivers the target component exposure. Because GHK-Cu makes up 62.5% of the blend, every draw delivers a larger GHK-Cu amount alongside smaller matched amounts of KPV, BPC-157, and TB-500.
Common Research-Context Titration
Community protocols typically titrate the blend slowly so users can observe response before increasing the daily volume. The schedule below shows the draw volume, total blend delivered, and component breakdown at 3.0 mL reconstitution. It is not a medical recommendation.
Representative KLOW titration at 3.0 mL reconstitution
Volumes assume the standard 80 mg vial and 3.0 mL reconstitution.
Phase
Weeks 1-2
Draw volume
7.5 units (0.075 mL)
Total blend delivered
~2.0 mg total blend
GHK-Cu
~1.25 mg
KPV
~250 mcg
BPC-157
~250 mcg
TB-500
~250 mcg
Phase
Weeks 3-4
Draw volume
15 units (0.15 mL)
Total blend delivered
~4.0 mg total blend
GHK-Cu
~2.5 mg
KPV
~500 mcg
BPC-157
~500 mcg
TB-500
~500 mcg
Phase
Weeks 5-8
Draw volume
22.5 units (0.225 mL)
Total blend delivered
~6.0 mg total blend
GHK-Cu
~3.75 mg
KPV
~750 mcg
BPC-157
~750 mcg
TB-500
~750 mcg
Phase
Weeks 9-12 (taper)
Draw volume
15 units (0.15 mL)
Total blend delivered
~4.0 mg total blend
GHK-Cu
~2.5 mg
KPV
~500 mcg
BPC-157
~500 mcg
TB-500
~500 mcg
| Phase | Draw volume | Total blend delivered | GHK-Cu | KPV | BPC-157 | TB-500 |
|---|---|---|---|---|---|---|
| Weeks 1-2 | 7.5 units (0.075 mL) | ~2.0 mg total blend | ~1.25 mg | ~250 mcg | ~250 mcg | ~250 mcg |
| Weeks 3-4 | 15 units (0.15 mL) | ~4.0 mg total blend | ~2.5 mg | ~500 mcg | ~500 mcg | ~500 mcg |
| Weeks 5-8 | 22.5 units (0.225 mL) | ~6.0 mg total blend | ~3.75 mg | ~750 mcg | ~750 mcg | ~750 mcg |
| Weeks 9-12 (taper) | 15 units (0.15 mL) | ~4.0 mg total blend | ~2.5 mg | ~500 mcg | ~500 mcg | ~500 mcg |
Blend ratio
50 / 10 / 10 / 10 mg
GHK-Cu dominant
Select a draw volume from the titration table above to see the approximate amount of each peptide delivered.
Reconstitute
3.0 mL BAC water
Concentration
26.7 mg/mL total blend
1 unit (0.01 mL)
~267 mcg total blend
Typical cycle
4-6 weeks
Dose selector
Component Delivery by Titration Step
- GHK-Cu:~1.25 mg
- KPV:~250 mcg
- BPC-157:~250 mcg
- TB-500:~250 mcg
Selector options mirror the representative titration table above. These component values are mathematical breakdowns of the blend, not dose recommendations. Note that GHK-Cu doses scale faster than the other three peptides because GHK-Cu makes up most of the vial.
Cycle Guidelines
KLOW Cycle Guidelines
Approach
Standard
Duration
4-6 weeks
Off Period
2-4 weeks
Notes
Most common cycle structure cited in the research-use community.
Approach
Extended
Duration
8-12 weeks
Off Period
4 weeks
Notes
Reported with slow titration; longer cycles raise copper-accumulation concern from GHK-Cu.
Approach
Maximum extension
Duration
Up to 16 weeks
Off Period
4+ weeks
Notes
Reported anecdotally; no safety data supports continuous use beyond 12 weeks.
| Approach | Duration | Off Period | Notes |
|---|---|---|---|
| Standard | 4-6 weeks | 2-4 weeks | Most common cycle structure cited in the research-use community. |
| Extended | 8-12 weeks | 4 weeks | Reported with slow titration; longer cycles raise copper-accumulation concern from GHK-Cu. |
| Maximum extension | Up to 16 weeks | 4+ weeks | Reported anecdotally; no safety data supports continuous use beyond 12 weeks. |
GHK-Cu's copper component is the main reason cycles are time-limited. Off periods are intended to allow copper clearance.
No direct trial evidence
No published clinical trial has evaluated the four-peptide KLOW combination together, and the doses cited above are extrapolated from individual-component research and community protocols, not validated as a synergistic dose for the blend.
KLOW Peptide Blend Supplies Needed
Plan based on a once-daily protocol at 3.0 mL reconstitution. The standard 80 mg vial supports about 30 daily injections at the 22.5-unit (0.225 mL) ceiling, or 40 daily injections at the 15-unit maintenance volume.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

KLOW Blend Supplies

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials
80 mg KLOW blend vials (50 mg GHK-Cu + 10 mg KPV + 10 mg BPC-157 + 10 mg TB-500).
| Cycle length | Planning note |
|---|---|
4 weeks 1 vial | 28 daily draws fit inside one vial at 22.5 units/day. |
6-8 weeks 2 vials | 6 weeks: 42 daily draws; one vial is not enough at the higher draw volume.; 8 weeks: 56 daily draws; allow margin for priming and dropped syringes. |
12 weeks 3 vials | 84 daily draws; round up for losses. |
4 weeks
1 vial
28 daily draws fit inside one vial at 22.5 units/day.
6-8 weeks
2 vials
6 weeks: 42 daily draws; one vial is not enough at the higher draw volume.; 8 weeks: 56 daily draws; allow margin for priming and dropped syringes.
12 weeks
3 vials
84 daily draws; round up for losses.
Insulin Syringes (U-100)
Use 30- or 50-unit syringes for draws under 10 units to improve readability.
| Cycle length | Planning note |
|---|---|
4 weeks 28 syringes | 1 syringe per day. |
6 weeks 42 syringes | 1 syringe per day. |
8 weeks 56 syringes | 1 syringe per day. |
12 weeks 84 syringes | 1 syringe per day. |
4 weeks
28 syringes
1 syringe per day.
6 weeks
42 syringes
1 syringe per day.
8 weeks
56 syringes
1 syringe per day.
12 weeks
84 syringes
1 syringe per day.
Bacteriostatic Water
Use 3.0 mL per vial for reconstitution.
| Cycle length | Planning note |
|---|---|
4-8 weeks 1 x 10 mL bottle | 4 weeks: 1 vial uses 3 mL; the bottle leaves margin.; 6 weeks: 2 vials use 6 mL total; one bottle is enough.; 8 weeks: 2 vials use 6 mL total; one bottle is enough. |
12 weeks 2 x 10 mL bottles | 3 vials use 9 mL total; a second bottle gives margin. |
4-8 weeks
1 x 10 mL bottle
4 weeks: 1 vial uses 3 mL; the bottle leaves margin.; 6 weeks: 2 vials use 6 mL total; one bottle is enough.; 8 weeks: 2 vials use 6 mL total; one bottle is enough.
12 weeks
2 x 10 mL bottles
3 vials use 9 mL total; a second bottle gives margin.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments.
Companion Supplies & Routine Support
KLOW Peptide Blend Reconstitution Guide
KLOW ships as a single lyophilized (freeze-dried) powder containing all four peptides. Reconstituting once produces a single solution from which every daily draw is taken. Most research-context protocols use 3.0 mL of bacteriostatic water for the 80 mg vial, which produces about 26.7 mg/mL total blend concentration.
KLOW concentration at common reconstitution volumes
BAC water
2.0 mL
Total concentration
40.0 mg/mL
GHK-Cu per unit (0.01 mL)
~250 mcg
KPV / BPC-157 / TB-500 per unit
~50 mcg each
BAC water
3.0 mL (most common)
Total concentration
26.7 mg/mL
GHK-Cu per unit (0.01 mL)
~167 mcg
KPV / BPC-157 / TB-500 per unit
~33 mcg each
BAC water
4.0 mL
Total concentration
20.0 mg/mL
GHK-Cu per unit (0.01 mL)
~125 mcg
KPV / BPC-157 / TB-500 per unit
~25 mcg each
| BAC water | Total concentration | GHK-Cu per unit (0.01 mL) | KPV / BPC-157 / TB-500 per unit |
|---|---|---|---|
| 2.0 mL | 40.0 mg/mL | ~250 mcg | ~50 mcg each |
| 3.0 mL (most common) | 26.7 mg/mL | ~167 mcg | ~33 mcg each |
| 4.0 mL | 20.0 mg/mL | ~125 mcg | ~25 mcg each |
Higher BAC water volumes give more measurable draws but require larger injection volumes.
Reconstitution Steps
- 01
Inspect the vial
Check the label, batch, and powder appearance. Loose, even powder is normal. A discolored or damp vial should not be used.
- 02
Sanitize
Swab the rubber stopper of the KLOW vial and the bacteriostatic water vial with alcohol prep pads. Let them dry.
- 03
Draw bacteriostatic water
Draw 3.0 mL bacteriostatic water with a sterile syringe. Vent the BAC water vial if needed to avoid pressure changes.
- 04
Inject down the vial wall
Insert the needle and inject the BAC water slowly down the inside wall of the KLOW vial. Avoid spraying directly onto the powder, which can cause foaming and denaturation.
- 05
Swirl, do not shake
Gently swirl or roll the vial until the powder is fully dissolved. The solution should be clear, with possible light blue tint from GHK-Cu (normal). Do not shake — shaking damages peptides.
- 06
Label and store
Label with the reconstitution date and store the vial at 35.6-46.4 F (2-8 C), protected from light.
- 07
Use within shelf life
Most stability references suggest using reconstituted multi-peptide blends within 14-28 days when refrigerated. Avoid freeze-thaw cycles.
Reconstitution math reminder
Verify the math for the specific vial size and BAC water volume in your batch. A peptide reconstitution calculator is the safest way to confirm draw volumes before injecting.
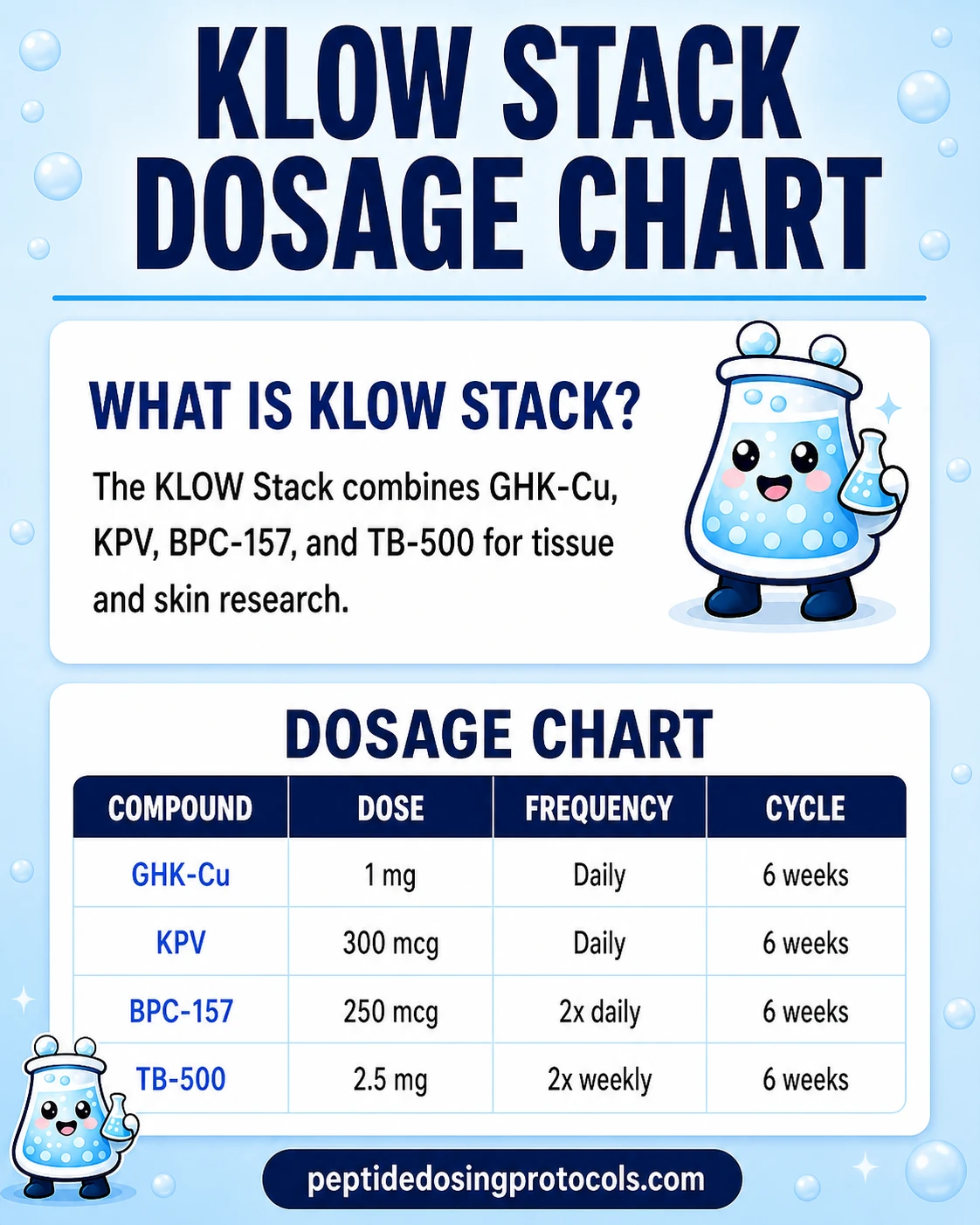
KLOW Stack Dosage Chart
This KLOW Stack dosage chart summarizes the common pre-blended 80 mg vial schedule, including the 50:10:10:10 GHK-Cu, KPV, BPC-157, and TB-500 ratio, the 3 mL reconstitution setup, and the once-daily reference dose range.
Why the KLOW Blend Adds KPV to the GLOW Stack
The GLOW stack pairs three regenerative peptides (GHK-Cu, BPC-157, TB-500) for a structural-repair and skin-rejuvenation focus. KLOW adds a fourth peptide, KPV, for a different reason: KPV's research focus is anti-inflammatory signaling, which the other three peptides do not directly target.
KPV is the C-terminal tripeptide fragment of alpha-melanocyte-stimulating hormone (alpha-MSH). In published preclinical work, KPV has been studied for inhibiting NF-κB activation in intestinal epithelial cells, with one widely cited study showing PepT1-mediated transport into colonic cells as part of its anti-inflammatory mechanism in mouse colitis models (Dalmasso et al., Gastroenterology, 2008).
BPC-157 and TB-500 also reduce inflammation in animal studies, but as a secondary effect of their tissue-repair pathways, not as a primary mechanism. GHK-Cu's anti-inflammatory effects flow through its broader gene-expression activity. KPV is the only one of the four that targets NF-κB-driven cytokine production directly.
Practical decision framing in the research-use community: if the research interest is structural repair, soft-tissue work, or skin remodeling alone, GLOW covers those bases. If the research context also involves chronic inflammation, gut-related models, or autoimmune-style settings, KPV is what KLOW adds.
Combination is not validated
No published study has tested whether GHK-Cu, KPV, BPC-157, and TB-500 act synergistically when administered together. The rationale above is mechanism-based community reasoning, not direct combination evidence.
KLOW Peptide Blend Side Effects & Safety
There are no published safety studies on the four-peptide KLOW combination. The information below is drawn from individual-compound research and community reports, separated into compound-level effects and stack-specific concerns.
Most Frequently Reported Effects
Subcutaneous peptide injections most commonly produce mild local effects: redness, mild swelling, or sensitivity at the injection site. A faint blue-green tint at the injection site is sometimes reported and is associated with the copper in GHK-Cu (cosmetic only). First-week mild fatigue and transient digestive shifts are also commonly described in user reports.
Less Commonly Reported Effects
Headache, light-headedness, vivid dreams (often attributed to BPC-157), and brief appetite changes are reported less frequently. None of these have been formally measured in a controlled study of the blend.
Stack-Specific Concerns
Copper accumulation (GHK-Cu)
GHK-Cu makes up 62.5% of the blend. Prolonged continuous use without an off period raises a theoretical risk of copper accumulation. Cycling 4-6 weeks on / 2-4 weeks off is the most common community-derived structure used to manage this.
Angiogenesis (BPC-157 and TB-500)
Both BPC-157 and TB-500 promote new blood vessel formation in animal models. This is the same mechanism that supports tissue repair, but it is a meaningful contraindication for anyone with active or recent malignancy.
Unknown interactions
No pharmacokinetic study has examined how the four peptides behave when injected together. Effects, timing, and any interactions are inferred, not measured.
Quality control
Research-use peptides are not held to pharmaceutical-grade manufacturing standards. Vial-to-vial purity, sterility, and accuracy of stated mass vary by supplier. Third-party Certificates of Analysis (COAs) reduce but do not eliminate this risk.
Common Contraindications
Active or recent cancer (BPC-157 and TB-500 angiogenesis concern), Wilson's disease or other copper metabolism disorders (GHK-Cu component), pregnancy or breastfeeding (no safety data for any component), and competitive sport at WADA-tested levels (BPC-157 and TB-500 are listed under WADA category S0 — Unapproved Substances) are commonly cited reasons not to research KLOW. Anyone on anticoagulants should be especially cautious with the angiogenesis-active components.
Stop and reassess
Stop the protocol and seek qualified medical care if pronounced symptoms appear: significant swelling, ongoing dizziness, rapid heart rate, shortness of breath, or marked fatigue.
KLOW Peptide Blend Clinical Evidence Context
No direct evidence: No published human or animal trial has evaluated the four-peptide KLOW combination. Every claim about the blend is extrapolated from individual-compound research, anecdotal community reports, or supplier marketing material. This is the most important boundary on this page.
Compound-Level Evidence
GHK-Cu
A 2018 review in the International Journal of Molecular Sciences synthesized gene-expression data showing GHK-Cu modulates over 4,000 human genes (Pickart and Margolina). Animal and ex-vivo human skin studies have reported increased collagen and elastin synthesis. Most clinical evidence is topical-formulation cosmetic research, not injectable. For topical research context, PepPal breaks down GHK-Cu skin product options.
KPV
Mechanism evidence comes from cell and animal studies. Dalmasso et al. (Gastroenterology, 2008) showed KPV reduces NF-κB activation and is taken up via PepT1 in mouse colitis models. No FDA-approved KPV drug exists.
BPC-157
A 2024 systematic review in HSS Journal (Vasireddi et al.) identified 36 included studies — 35 preclinical, 1 small clinical — across nearly three decades. Preclinical models report tendon, ligament, muscle, and gut healing benefits, but human evidence remains limited to a handful of small open-label pilot studies.
TB-500 / Thymosin beta-4
Goldstein and colleagues established thymosin beta-4 as the principal G-actin-sequestering peptide in mammalian cells. Preclinical work documents accelerated wound healing, cardiac repair after infarction, and corneal healing. Most human trials use the full 43-amino-acid thymosin beta-4 (RGN-259, RGN-137), not the TB-500 fragment.
Compound-level evidence does not validate a stack. Even if each peptide has independent research support, the combination has not been studied for synergy, antagonism, pharmacokinetic interaction, or safety. Anyone reading the literature should treat KLOW as a research-context blend, not as a clinically validated protocol.
KLOW Peptide Blend Storage & Handling
KLOW Storage at a Glance
State
Lyophilized (powder)
Storage
-4 F (-20 C) long-term; refrigerator acceptable short-term
Notes
Keep dry, dark, in original packaging.
State
Reconstituted (liquid)
Storage
35.6-46.4 F (2-8 C) refrigerated
Notes
Use within 14-28 days; do not freeze.
State
Appearance
Storage
Clear; light blue tint possible
Notes
Discoloration beyond a faint blue-green hint suggests contamination.
| State | Storage | Notes |
|---|---|---|
| Lyophilized (powder) | -4 F (-20 C) long-term; refrigerator acceptable short-term | Keep dry, dark, in original packaging. |
| Reconstituted (liquid) | 35.6-46.4 F (2-8 C) refrigerated | Use within 14-28 days; do not freeze. |
| Appearance | Clear; light blue tint possible | Discoloration beyond a faint blue-green hint suggests contamination. |
Allow lyophilized vials to reach room temperature before reconstitution to reduce condensation moisture.
Avoid repeated freeze-thaw cycles in the reconstituted form — every freeze-thaw cycle damages peptide structure and reduces potency. Keep the vial protected from direct light during cold storage.
KLOW vs GLOW vs Wolverine Stack
KLOW is most often compared to two nearby blends. The choice usually comes down to whether KPV's anti-inflammatory mechanism is part of the research interest.
KLOW vs GLOW vs Wolverine Stack
Feature
Components
Wolverine Stack
BPC-157 + TB-500
GLOW Stack
GHK-Cu + BPC-157 + TB-500
KLOW Blend
GHK-Cu + KPV + BPC-157 + TB-500
Feature
Total vial mass (typical)
Wolverine Stack
10-20 mg
GLOW Stack
70 mg
KLOW Blend
80 mg
Feature
Primary research focus
Wolverine Stack
Soft-tissue repair
GLOW Stack
Skin + tissue + recovery
KLOW Blend
Skin + tissue + anti-inflammatory
Feature
Adds KPV (anti-inflammatory)
Wolverine Stack
No
GLOW Stack
No
KLOW Blend
Yes
Feature
Adds GHK-Cu (collagen / gene expression)
Wolverine Stack
No
GLOW Stack
Yes
KLOW Blend
Yes
Feature
Number of injections
Wolverine Stack
1
GLOW Stack
1
KLOW Blend
1
| Feature | Wolverine Stack | GLOW Stack | KLOW Blend |
|---|---|---|---|
| Components | BPC-157 + TB-500 | GHK-Cu + BPC-157 + TB-500 | GHK-Cu + KPV + BPC-157 + TB-500 |
| Total vial mass (typical) | 10-20 mg | 70 mg | 80 mg |
| Primary research focus | Soft-tissue repair | Skin + tissue + recovery | Skin + tissue + anti-inflammatory |
| Adds KPV (anti-inflammatory) | No | No | Yes |
| Adds GHK-Cu (collagen / gene expression) | No | Yes | Yes |
| Number of injections | 1 | 1 | 1 |
These are the most common community framings; vial mass varies by supplier.
If the research interest centers on tendon, muscle, or post-injury repair, the Wolverine stack is the simplest entry point. If skin/connective-tissue research is the focus, GLOW adds GHK-Cu. KLOW is the choice when the research scope also touches on inflammatory signaling — KPV is the differentiator.
KLOW Stack Blood Tests & Monitoring
The KLOW Stack combines GHK-Cu, KPV, BPC-157, and TB-500, so monitoring should cover immune/inflammatory context, tissue-repair context, and copper exposure. Labs can support broad review but may not capture local tissue or gut response.
Blood test markers to discuss with a clinician
Marker
CBC with differential
Why it matters
Screens blood-cell patterns, infection context, anemia, and immune changes.
Timing
Baseline
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver, kidney, electrolyte, and glucose context in one broad panel.
Timing
Baseline
Marker
CRP
Why it matters
Adds a broad inflammation marker when gut, skin, immune, or injury symptoms are part of the question.
Timing
Follow-up
Marker
ESR
Why it matters
Provides a slower-moving inflammation marker for chronic inflammatory symptoms.
Timing
Optional
Marker
Copper and ceruloplasmin
Why it matters
Adds copper-status context when repeated high-exposure GHK-Cu use is being discussed.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| CBC with differential | Screens blood-cell patterns, infection context, anemia, and immune changes. | Baseline |
| Comprehensive metabolic panel (CMP) | Reviews liver, kidney, electrolyte, and glucose context in one broad panel. | Baseline |
| CRP | Adds a broad inflammation marker when gut, skin, immune, or injury symptoms are part of the question. | Follow-up |
| ESR | Provides a slower-moving inflammation marker for chronic inflammatory symptoms. | Optional |
| Copper and ceruloplasmin | Adds copper-status context when repeated high-exposure GHK-Cu use is being discussed. | Optional |
Monitoring guidance combines immune, inflammation, tissue-repair, and copper-context pathway logic for the listed stack components.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with autoimmune disease, gut symptoms, active injury, infection concern, liver disease, kidney disease, or copper concerns.
Follow-up
Repeat broad and inflammation markers after 6-12 weeks if symptoms change or the protocol continues.
Longer term
For longer repeated exposure, review broad health, inflammation, and copper-context markers every 3-6 months with a clinician.
How to interpret the labs
- Autoimmune disease, infection risk, immune medications, and copper exposure from supplements should be reviewed clinically.
- Routine labs may look normal even when local gut, skin, or connective-tissue symptoms remain.
- Avoid positioning this stack as a treatment or cure for inflammatory disease.
Do not wait for routine labs
Fever, bloody stool, severe abdominal pain, spreading rash, jaundice, allergic symptoms, or severe wound changes need medical review.
FAQ
Q1: What is the KLOW peptide blend?
KLOW is a research-context name for a four-peptide blend that combines GHK-Cu, KPV, BPC-157, and TB-500 in a single vial. The standard format is an 80 mg vial split as 50 mg GHK-Cu, 10 mg KPV, 10 mg BPC-157, and 10 mg TB-500. KLOW is not an FDA-approved treatment and no published clinical trial has evaluated the four-peptide combination together.
Q2: What does the KLOW peptide blend research focus on?
Community discussion of KLOW most often centers on tissue-repair research, skin/connective-tissue remodeling, recovery research, and anti-inflammatory research. These are research-context interests, not validated clinical outcomes. Direct human evidence for the KLOW combination does not exist.
Q3: How is the KLOW peptide blend dosed in research planning?
Most community protocols reconstitute the 80 mg vial with 3.0 mL bacteriostatic water (about 26.7 mg/mL total blend) and use once-daily subcutaneous injections starting at small volumes. Common research-context daily total-blend amounts range from about 250 mcg total per component up to about 750 mcg per component during a peak phase. None of these are dose recommendations.
Q4: What is the difference between KLOW and GLOW peptides?
GLOW is a three-peptide blend with GHK-Cu, BPC-157, and TB-500. KLOW adds a fourth peptide, KPV. The KPV component is what distinguishes KLOW — its research focus is on anti-inflammatory signaling (NF-κB inhibition, PepT1-mediated transport in gut models). When chronic inflammation is part of the research interest, KLOW is the more common choice; otherwise GLOW covers the same regenerative components.
Q5: How long is a typical KLOW cycle?
Community-derived cycle structures most often run 4-6 weeks on followed by 2-4 weeks off. Some protocols extend to 8-12 weeks with longer off periods. The off period is mainly there to address copper-accumulation concern from the GHK-Cu component, which makes up 62.5% of the blend.
Q6: How is the KLOW peptide blend reconstituted?
The most common research-context approach is to add 3.0 mL of bacteriostatic water to the 80 mg KLOW vial. This produces about 26.7 mg/mL total blend. The mix is swirled gently — never shaken — and stored refrigerated at 35.6-46.4 F (2-8 C). A peptide reconstitution calculator is the safest way to confirm draw volumes for a specific vial size.
Q7: Is the KLOW peptide blend FDA-approved?
No. As of June 2026, none of the four peptides in KLOW are FDA-approved for the indications discussed in the research community. BPC-157 and TB-500 are also listed by WADA under category S0 (Unapproved Substances) and are prohibited in tested sport.
Q8: What supplies are needed for a KLOW protocol?
A common research-context setup includes the 80 mg KLOW vial(s), one 10 mL bottle of bacteriostatic water per 1-2 vials, U-100 insulin syringes (one per daily injection — 30- or 50-unit syringes are easier to read for small draws), and alcohol prep pads (two per injection). For an 8-week protocol, that is typically 2 vials of KLOW, 1 bottle of bacteriostatic water, 56 syringes, and 112 swabs.
Q9: Who should avoid the KLOW peptide blend?
Common contraindications cited in the research-use community include: anyone with active or recent cancer (BPC-157 and TB-500 promote angiogenesis), people with Wilson's disease or other copper-metabolism disorders (GHK-Cu component), anyone pregnant or breastfeeding (no safety data), and athletes subject to WADA testing (BPC-157 and TB-500 are prohibited).
Q10: Is the KLOW peptide blend medical advice?
No. This page is an educational research reference, not medical advice. KLOW is not an FDA-approved treatment. Anyone considering peptide research should work within their applicable regulations and seek qualified medical guidance.
Sources & Research
- 1. Pickart L, Margolina A. Regenerative and Protective Actions of the GHK-Cu Peptide in the Light of the New Gene Data. International Journal of Molecular Sciences (2018)
- 2. Pickart L. GHK Peptide as a Natural Modulator of Multiple Cellular Pathways in Skin Regeneration. BioMed Research International (2015)
- 3. Dou Y, et al. The potential of GHK as an anti-aging peptide. Aging Pathobiology and Therapeutics (2022)
- 4. Dalmasso G, Charrier-Hisamuddin L, Nguyen HT, et al. PepT1-Mediated Tripeptide KPV Uptake Reduces Intestinal Inflammation. Gastroenterology (2008)
- 5. Brzoska T, Luger TA, Maaser C, Abels C, Bohm M. Alpha-MSH related peptides: a new class of anti-inflammatory and immunomodulating drugs. British Journal of Pharmacology / NIHMS PMC (2008)
- 6. Xiao B, Xu Z, Viennois E, et al. Orally Targeted Delivery of Tripeptide KPV via Hyaluronic Acid-Functionalized Nanoparticles Efficiently Alleviates Ulcerative Colitis. Molecular Therapy / PMC (2017)
- 7. Vasireddi N, Hahamyan H, Salata MJ, et al. Emerging Use of BPC-157 in Orthopaedic Sports Medicine: A Systematic Review. HSS Journal (2025)
- 8. Various authors. Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing. Cureus / PMC (2024)
- 9. Malinda KM, Sidhu GS, Mani H, et al. Thymosin beta4 accelerates wound healing. Journal of Investigative Dermatology (1999)
- 10. Goldstein AL, Hannappel E, Sosne G, Kleinman HK. Thymosin beta4: a multi-functional regenerative peptide. Basic properties and clinical applications. Expert Opinion on Biological Therapy (2012)
- 11. Sosne G, Qiu P, Goldstein AL, Wheater M. Thymosin beta 4: A novel corneal wound healing and anti-inflammatory agent. Clinical Ophthalmology / PMC (2007)
- 12. U.S. Food and Drug Administration. 503A Bulks List Final Rule and 503B Bulk Drug Substances - peptide categorization references. FDA (2026)
- 13. World Anti-Doping Agency. WADA Prohibited List - Section S0 Unapproved Substances (BPC-157, TB-500 categorization). WADA (2026)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page