KPV Peptide Quick Start
KPV is a three-amino-acid peptide (lysine-proline-valine) cut from the C-terminus of alpha-MSH. The research community most often discusses it for anti-inflammatory and gut-barrier work, particularly in inflammatory bowel disease (IBD) models.
What makes KPV unusual is that it can be used orally. Most peptides break down in the gut, but KPV is small and stable enough to be absorbed through a transporter called PepT1. This is why oral KPV protocols are common, especially for gut-focused research, while subcutaneous (SubQ) protocols are more common for systemic models.
Unlike melanotan-type peptides, KPV does not trigger pigmentation. It uses a different mechanism than the rest of alpha-MSH and skips melanocortin-receptor signaling.
Routes
Oral, subcutaneous, topical, and (less commonly) intranasal.
Range
200-500 mcg daily is the most-discussed research-planning range.
Measure
10 mg + 2 mL BAC water gives 5,000 mcg/mL; 500 mcg = 0.10 mL = 10 units.
Supplies
Vial, BAC water, U-100 insulin syringes, and alcohol swabs for SubQ; oral can be drawn into the mouth from the same vial in some protocols.
Status
Not FDA-approved. Removed from Category 2 on April 22, 2026; PCAC consults July 23, 2026.
Disclaimer
This page is an educational research reference and is not medical advice. KPV is not FDA-approved for any indication. No published human efficacy trial defines an optimal dose. Consult a licensed clinician before considering any peptide protocol.
This protocol page is for KPV dosing, vial mixing, and planning. For the broader research view, visit the KPV guide on how it may work, studies, safety notes, and legal status.
KPV Dosing Protocol & Schedule
KPV has been discussed across three main routes: oral, subcutaneous (SubQ), and topical. The choice usually follows the research target. Oral is favored for gut-focused work because PepT1 transporters are concentrated in inflamed intestinal tissue. SubQ is favored for systemic anti-inflammatory models. Topical is sometimes compounded for localized skin-inflammation models.
No completed human dose-finding trial defines an official KPV dose. The ranges below come from preclinical extrapolation and community-derived planning notes, not from FDA labels or registered trials.
KPV Protocol Formats
Choose the format you are researching to see route-specific notes.
Subcutaneous use is the most common route in systemic anti-inflammatory research.
Injectable (SubQ) Phased Schedule
Phase
Initiation
Weeks
Weeks 1-2
Daily Dose
200 mcg/day SubQ
Notes
Low-start tolerance and response check.
Phase
Titration
Weeks
Weeks 3-4
Daily Dose
300-400 mcg/day SubQ
Notes
Increase by about 100 mcg/week as tolerated.
Phase
Maintenance
Weeks
Weeks 5-12
Daily Dose
400-500 mcg/day SubQ
Notes
Common anti-inflammatory maintenance window.
| Phase | Weeks | Daily Dose | Notes |
|---|---|---|---|
| Initiation | Weeks 1-2 | 200 mcg/day SubQ | Low-start tolerance and response check. |
| Titration | Weeks 3-4 | 300-400 mcg/day SubQ | Increase by about 100 mcg/week as tolerated. |
| Maintenance | Weeks 5-12 | 400-500 mcg/day SubQ | Common anti-inflammatory maintenance window. |
Some research-planning protocols extend to 1,000 mcg/day in higher-burden contexts; this is on the upper end and is not better-supported than the 200-500 mcg range.
Injection logistics: Most users rotate SubQ sites (abdomen, flank, thigh) and use a separate syringe for each compound when stacking with BPC-157, TB-500, or GHK-Cu. Reconstituted KPV is refrigerated between draws.
Oral dosing is the preferred route for gut-focused research because of PepT1 absorption.
Oral KPV Schedule
Approach
Standard oral
Duration
Weeks 1-8+
Daily Dose
200-500 mcg once or twice daily
Notes
Preferred route for gut-focused workflows.
Approach
Intensive oral
Duration
Weeks 1-8+
Daily Dose
500 mcg twice daily
Notes
Used in higher-burden inflammatory contexts.
| Approach | Duration | Daily Dose | Notes |
|---|---|---|---|
| Standard oral | Weeks 1-8+ | 200-500 mcg once or twice daily | Preferred route for gut-focused workflows. |
| Intensive oral | Weeks 1-8+ | 500 mcg twice daily | Used in higher-burden inflammatory contexts. |
Take on an empty stomach to reduce competition from dietary peptides at PepT1.
Why oral works for KPV: Most peptides cannot survive the digestive tract. KPV's proline and valine residues resist gut enzymes, and the small size allows transport through PepT1. Inflamed intestinal tissue produces more PepT1, so oral KPV may concentrate in exactly the area being studied.
Topical KPV is compounded by some pharmacies for localized skin-inflammation research.
Topical KPV Schedule
Use Model
Localized skin inflammation
Duration
4-8+ weeks
Frequency
1-2x daily
Notes
Compounded topical preparation; concentration varies by formulation.
| Use Model | Duration | Frequency | Notes |
|---|---|---|---|
| Localized skin inflammation | 4-8+ weeks | 1-2x daily | Compounded topical preparation; concentration varies by formulation. |
Topical KPV concentration and base are formulation-specific; follow the compounding pharmacy's labeling.
KPV Cycle Guidelines
Approach
Standard
On Period
4-8 weeks
Off Period
2-4 weeks
Best For
General anti-inflammatory research planning
Approach
Extended
On Period
8-16 weeks
Off Period
4-8 weeks
Best For
Longer protocols with periodic off windows
Approach
Pulsed gut-focused
On Period
4 weeks
Off Period
2 weeks
Best For
Oral KPV, IBD-style flare-window models
| Approach | On Period | Off Period | Best For |
|---|---|---|---|
| Standard | 4-8 weeks | 2-4 weeks | General anti-inflammatory research planning |
| Extended | 8-16 weeks | 4-8 weeks | Longer protocols with periodic off windows |
| Pulsed gut-focused | 4 weeks | 2 weeks | Oral KPV, IBD-style flare-window models |
Cycle structure is community-derived. No human trial has defined optimal on/off ratios for KPV.
Evidence Level Notice
No completed human dose-finding trials define optimal KPV dosing. The schedules above are preclinical extrapolation and community-derived. Missed-dose handling: resume the next scheduled dose without doubling up.
KPV Supplies Needed
Affiliate disclosure: PDP may earn a commission when you use eligible supplier links, at no extra cost to you. The math below assumes 500 mcg daily SubQ from a 10 mg vial reconstituted with 2 mL BAC water (5,000 mcg/mL).
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

KPV Supply

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
KPV Vials (10 mg)
Most common research-grade size. Reconstituted with 2 mL BAC water, one vial supplies 20 doses at 500 mcg/day.
| Cycle length | Planning note |
|---|---|
4 weeks 2 vials | 28 doses needed; 2 vials cover with margin. |
6-8 weeks 3 vials | 6 weeks: 42 doses needed; round up for losses.; 8 weeks: 56 doses needed; 3 vials = 60 doses. |
12 weeks 5 vials | 84 doses needed; round up for losses and longer storage. |
4 weeks
2 vials
28 doses needed; 2 vials cover with margin.
6-8 weeks
3 vials
6 weeks: 42 doses needed; round up for losses.; 8 weeks: 56 doses needed; 3 vials = 60 doses.
12 weeks
5 vials
84 doses needed; round up for losses and longer storage.
Insulin Syringes (U-100)
0.3 mL / 30-unit syringes are typical for KPV's small draw volumes.
| Cycle length | Planning note |
|---|---|
4 weeks 30 syringes | 1 syringe per injection. |
6 weeks 45 syringes | 1 syringe per injection. |
8 weeks 60 syringes | 1 syringe per injection. |
12 weeks 90 syringes | 1 syringe per injection. |
4 weeks
30 syringes
1 syringe per injection.
6 weeks
45 syringes
1 syringe per injection.
8 weeks
60 syringes
1 syringe per injection.
12 weeks
90 syringes
1 syringe per injection.
Bacteriostatic Water
Each 10 mg KPV vial uses 2 mL BAC water at the standard concentration.
| Cycle length | Planning note |
|---|---|
4-8 weeks 1 x 10 mL bottle | 4 weeks: 2 vials use 4 mL total; one bottle gives margin.; 6 weeks: 3 vials use 6 mL total.; 8 weeks: 3 vials use 6 mL total. |
12 weeks 2 x 10 mL bottles | 5 vials use 10 mL; second bottle gives margin. |
4-8 weeks
1 x 10 mL bottle
4 weeks: 2 vials use 4 mL total; one bottle gives margin.; 6 weeks: 3 vials use 6 mL total.; 8 weeks: 3 vials use 6 mL total.
12 weeks
2 x 10 mL bottles
5 vials use 10 mL; second bottle gives margin.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments. Oral protocols do not need syringes or swabs but still need BAC water for reconstitution.
Companion Supplies & Routine Support
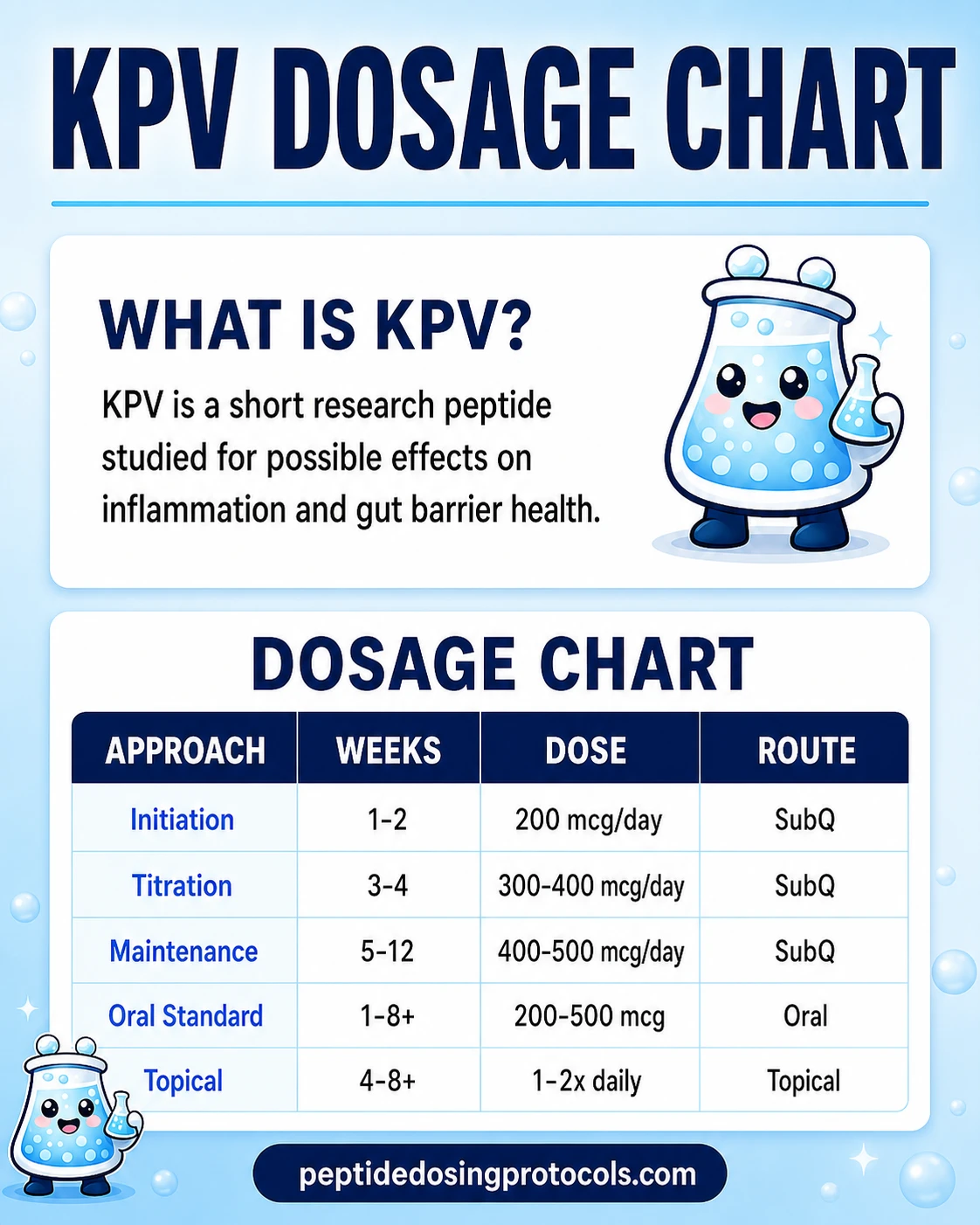
KPV Dosage Chart
This KPV dosage chart summarizes the oral, SubQ, and topical research-context dosing ranges shown in the dosing section above.
KPV Reconstitution Guide
Reconstitution is the same step regardless of route. Even oral protocols often start from a reconstituted vial — the liquid is taken sublingually or with water on an empty stomach. The table below covers the most common 5 mg and 10 mg vial sizes at multiple BAC-water volumes.
KPV Reconstitution Math (Vial × BAC Water)
Vial Size
5 mg
BAC Water
1 mL
Concentration
5,000 mcg/mL
200 mcg
0.04 mL (4 units)
300 mcg
0.06 mL (6 units)
500 mcg
0.10 mL (10 units)
Vial Size
5 mg
BAC Water
2 mL
Concentration
2,500 mcg/mL
200 mcg
0.08 mL (8 units)
300 mcg
0.12 mL (12 units)
500 mcg
0.20 mL (20 units)
Vial Size
10 mg
BAC Water
2 mL
Concentration
5,000 mcg/mL
200 mcg
0.04 mL (4 units)
300 mcg
0.06 mL (6 units)
500 mcg
0.10 mL (10 units)
Vial Size
10 mg
BAC Water
3 mL
Concentration
3,333 mcg/mL
200 mcg
0.06 mL (6 units)
300 mcg
0.09 mL (9 units)
500 mcg
0.15 mL (15 units)
Vial Size
10 mg
BAC Water
5 mL
Concentration
2,000 mcg/mL
200 mcg
0.10 mL (10 units)
300 mcg
0.15 mL (15 units)
500 mcg
0.25 mL (25 units)
| Vial Size | BAC Water | Concentration | 200 mcg | 300 mcg | 500 mcg |
|---|---|---|---|---|---|
| 5 mg | 1 mL | 5,000 mcg/mL | 0.04 mL (4 units) | 0.06 mL (6 units) | 0.10 mL (10 units) |
| 5 mg | 2 mL | 2,500 mcg/mL | 0.08 mL (8 units) | 0.12 mL (12 units) | 0.20 mL (20 units) |
| 10 mg | 2 mL | 5,000 mcg/mL | 0.04 mL (4 units) | 0.06 mL (6 units) | 0.10 mL (10 units) |
| 10 mg | 3 mL | 3,333 mcg/mL | 0.06 mL (6 units) | 0.09 mL (9 units) | 0.15 mL (15 units) |
| 10 mg | 5 mL | 2,000 mcg/mL | 0.10 mL (10 units) | 0.15 mL (15 units) | 0.25 mL (25 units) |
Lower concentration = larger draw volume = better precision for microgram-level dosing. Use a U-100 insulin syringe and read units, not mL.
Standard 7-Step Reconstitution
- 01
Wipe the stopper
Wipe the vial stopper with alcohol and let it dry.
- 02
Draw BAC water
Draw the planned BAC water volume into a sterile syringe.
- 03
Inject against the wall
Direct the BAC water against the inside of the vial wall, not onto the powder.
- 04
Let it flow gently
Allow gentle flow; do not force pressure.
- 05
Roll, do not shake
Roll the vial gently for 30-60 seconds. Shaking can damage the peptide.
- 06
Inspect
Solution should be clear and colorless. Cloudy, particulate, or off-color solutions should be discarded.
- 07
Label and refrigerate
Label with concentration and date. Refrigerate at 35.6-46.4F (2-8C). Use within 30 days.
Calculator
Need exact units for a different vial size or BAC volume? Use the PepPal reconstitution calculator.
How KPV Works
KPV works differently from most anti-inflammatory compounds. Instead of broadly suppressing the immune system the way steroids do, it targets a specific inflammation switch inside cells. The mechanism is unusually well mapped for a peptide that has not been tested in humans.
PepT1 Uptake
PepT1 is a transporter on the surface of intestinal cells that moves di- and tripeptides from the gut into the cell. KPV is small enough to fit. Inflamed gut tissue produces more PepT1, so oral KPV may preferentially concentrate where inflammation is worst (Dalmasso et al. 2008, Gastroenterology).
NF-kB Inhibition
NF-kB is the master switch that turns on inflammatory gene expression. Preclinical work reports that KPV reduces how long this switch stays "on" and how many inflammatory signals are produced — without the broad immunosuppression of corticosteroids.
What KPV Does Not Do
Some older articles claim KPV acts on melanocortin receptors. This is incorrect. The 2008 Dalmasso paper showed no melanocortin-receptor signaling, and follow-up work in receptor-knockout mice confirmed KPV still works without those receptors. KPV does not cause tanning or pigmentation changes and should not be confused with melanotan compounds.
PepT1-mediated uptake
Concentrates KPV in inflamed intestinal tissue.
NF-kB inhibition
Reduces inflammatory gene expression intracellularly.
MAP kinase suppression
Lowers TNF-driven inflammatory signaling in cell models.
Antimicrobial activity
Direct activity against S. aureus and C. albicans in lab assays.
Not melanocortin-mediated
Bypasses the receptor pathway used by alpha-MSH and melanotan compounds.
Who KPV Is For and Who Should Avoid It
KPV is researched mainly for anti-inflammatory and gut-barrier models. Because no human trial has been completed, eligibility framing is conservative.
Generally outside research-planning scope: pregnancy and breastfeeding (no safety data), known hypersensitivity to peptide compounds, and active complex infectious disease without clinician oversight (because of overlapping inflammatory and antimicrobial signaling).
Caution areas: active autoimmune disease on prescribed immunomodulators (the interaction has not been studied), and IBD or other inflammatory bowel conditions managed with prescription therapy. KPV should not replace prescribed medication and should be discussed with the treating clinician.
Quality-control caution: KPV is sold as research-use peptide outside FDA-approved channels. Source quality, COA verification, and storage handling vary widely between suppliers.
KPV Side Effects & Safety
KPV is generally reported as well-tolerated in animal studies and in community use, but no formal human safety trial has been completed. Long-term safety data does not exist.
Commonly reported effects (community-level, not trial data): mild and transient injection-site irritation, occasional mild headache, and occasional GI upset at higher oral doses.
Pigmentation: KPV is generally modeled as non-pigmenting. It does not bind the melanocortin receptors that drive melanotan-style tanning.
Immune profile: KPV dials down specific inflammatory pathways (notably NF-kB) rather than broadly suppressing the immune system. In animal work this has not produced the infection-susceptibility profile seen with corticosteroids — but this distinction has not been confirmed in human trials.
Quality-control risk: As with any research-use peptide, contamination, underdosing, or incorrect labeling are real risks. Use COA-verified suppliers and inspect every reconstituted vial for clarity before use.
General cautions: Avoid in pregnancy/breastfeeding. Discuss with a clinician if you have active autoimmune disease, complex infectious disease, or are taking prescribed immunomodulators.
KPV Timeline & What to Monitor
There is no human trial defining a KPV timeline. Animal studies measure inflammatory markers within days to weeks. Community-reported timelines should be treated as anecdotal.
Reported KPV Timeline (Community-Level)
Window
Week 1-2
Commonly Reported
Early symptom-level shifts in gut comfort or skin inflammation
Notes
Highly individual; not a guarantee.
Window
Week 2-4
Commonly Reported
Broader trend changes; inflammatory flares often described as less frequent
Notes
No biomarker confirmation in community reports.
Window
Week 6-12
Commonly Reported
Full anti-inflammatory model assessment
Notes
End of common research-planning windows.
| Window | Commonly Reported | Notes |
|---|---|---|
| Week 1-2 | Early symptom-level shifts in gut comfort or skin inflammation | Highly individual; not a guarantee. |
| Week 2-4 | Broader trend changes; inflammatory flares often described as less frequent | No biomarker confirmation in community reports. |
| Week 6-12 | Full anti-inflammatory model assessment | End of common research-planning windows. |
These are reported observations, not human trial endpoints.
What to monitor (for research review): symptom-level changes, injection-site condition, oral GI tolerance, and any new symptoms that prompt review with a clinician. Lab panels are not standard for KPV review because there is no trial-defined monitoring protocol.
Stopping points: persistent injection-site reactions that worsen rather than improve, unexpected GI symptoms on oral protocols, or any symptom that warrants clinician evaluation.
KPV Clinical Evidence Context
No completed human trial
All published KPV efficacy data comes from animal models and laboratory cell experiments. No completed human clinical trial has confirmed KPV's effects, optimal dosing, or long-term safety profile in people.
Dalmasso et al. 2008 (Gastroenterology)
Oral KPV reduced colitis severity in DSS and TNBS mouse models. Identified PepT1-mediated uptake as the central mechanism.
Xiao et al. 2017 (Molecular Therapy)
Nanoparticle-delivered KPV improved targeting to inflamed colonic tissue and reduced inflammatory markers in DSS colitis.
Kannengiesser et al. 2008
Dose-dependent suppression of TNF-driven inflammatory signaling in bronchial epithelial cell models.
Catania et al. 2000
Reported direct antimicrobial activity against S. aureus and C. albicans in lab assays.
Brzoska, Luger, Maaser et al. 2008
Review of alpha-MSH-derived peptides as a class, including KPV's place in melanocortin-system research.
Getting et al. 2006
Reviewed melanocortin-derived anti-inflammatory pharmacology and confirmed KPV's distinction from receptor-mediated signaling.
The gut-inflammation findings — particularly the PepT1 transport discovery — are the strongest part of the KPV literature. They are still preclinical. No human study has yet confirmed how effective KPV is in people, what an optimal dose looks like, or what the long-term safety profile is.
KPV Storage & Handling
KPV Storage Reference
State
Lyophilized (powder)
Storage
-4F (-20C) freezer
Duration
Long-term (years)
State
Lyophilized (powder)
Storage
35.6-46.4F (2-8C) refrigerator
Duration
Months
State
Lyophilized (powder)
Storage
59-77F (15-25C) room
Duration
Weeks (shipping tolerance)
State
Reconstituted
Storage
35.6-46.4F (2-8C) refrigerator
Duration
Up to 30 days
State
Reconstituted
Storage
Do not freeze
Duration
N/A
| State | Storage | Duration |
|---|---|---|
| Lyophilized (powder) | -4F (-20C) freezer | Long-term (years) |
| Lyophilized (powder) | 35.6-46.4F (2-8C) refrigerator | Months |
| Lyophilized (powder) | 59-77F (15-25C) room | Weeks (shipping tolerance) |
| Reconstituted | 35.6-46.4F (2-8C) refrigerator | Up to 30 days |
| Reconstituted | Do not freeze | N/A |
Protect from light and moisture. Avoid freeze-thaw cycling. Use bacteriostatic water (not sterile water) for multi-dose workflows.
KPV Protocol Mistakes & Troubleshooting
- 01
Missed dose
Resume the next scheduled dose without doubling up. KPV's effect window is short, so a single missed daily dose has limited downstream impact.
- 02
Cloudy or particulate vial
Discard. Reconstituted KPV should be clear and colorless. Cloudiness can indicate contamination or peptide degradation.
- 03
Wrong BAC water volume
Recalculate concentration before drawing. Adding more water lowers concentration and increases the draw volume; do not draw the original units number against a re-diluted vial.
- 04
Oral dose taken with food
PepT1 absorption competes with dietary peptides. Re-take on an empty stomach next time; do not double the dose to compensate.
- 05
Injection-site reaction
Mild redness or irritation usually resolves quickly. Persistent or worsening reactions should pause the protocol and prompt clinician review.
- 06
Storage mistake (left at room temperature)
Reconstituted KPV is stable at 2-8C for up to 30 days. Brief room-temperature exposure during a draw is fine; prolonged unrefrigerated storage shortens shelf life and risks degradation.
- 07
Confused mcg vs mg
KPV is dosed in micrograms (mcg). When stacking with TB-500 or GHK-Cu (dosed in mg), label every vial to avoid 1,000x errors.
KPV Regulatory Status
As of June 2026, KPV is not FDA-approved for any indication. No pharmaceutical company holds an approved KPV drug.
On April 15, 2026, the FDA published a notice that twelve peptide bulk drug substances would be removed from Category 2 (the "significant safety concerns" list) effective April 22, 2026, because the original nominators withdrew their nominations. KPV was on that list.
Removal from Category 2 does not place KPV on Category 1 and does not constitute FDA approval. The Pharmacy Compounding Advisory Committee (PCAC) is scheduled to consult on the potential inclusion of KPV acetate and KPV (free base) on the 503A bulks list at its meeting on July 23, 2026. Until that review concludes and the FDA acts on it, compounding pharmacies remain in a transitional position.
WADA status: KPV is not a named WADA-prohibited substance. The relevant alpha-MSH-derived compounds covered under WADA rules are different molecules.
Sources for this section: FDA bulk substances list update (April 22, 2026 revision) and the SSRP Institute April 15, 2026 announcement. See the Sources & Research section for direct links.
KPV vs BPC-157 vs alpha-MSH
KPV is most often compared to BPC-157 (a repair-focused peptide) and to alpha-MSH (the full-length hormone KPV is derived from). The short version: KPV is for inflammation, BPC-157 is for repair, and alpha-MSH is the parent hormone with broader effects.
KPV vs BPC-157 vs alpha-MSH
Feature
Origin
KPV
C-terminal tripeptide of alpha-MSH
BPC-157
Synthetic 15-aa gastric-protein fragment
alpha-MSH (full-length)
Endogenous 13-aa melanocortin hormone
Feature
Primary mechanism
KPV
PepT1 uptake; NF-kB inhibition
BPC-157
Angiogenesis; tissue-protective signaling
alpha-MSH (full-length)
Melanocortin-receptor activation
Feature
Primary use model
KPV
Inflammation control; gut-barrier support
BPC-157
Structural tissue repair
alpha-MSH (full-length)
Pigmentation; melanocortin signaling
Feature
Oral viability
KPV
Yes (PepT1)
BPC-157
Yes
alpha-MSH (full-length)
Limited
Feature
Pigmentation effects
KPV
No
BPC-157
No
alpha-MSH (full-length)
Yes
Feature
Clinical evidence
KPV
Preclinical only
BPC-157
Limited human + broad preclinical
alpha-MSH (full-length)
Extensive hormonal research
| Feature | KPV | BPC-157 | alpha-MSH (full-length) |
|---|---|---|---|
| Origin | C-terminal tripeptide of alpha-MSH | Synthetic 15-aa gastric-protein fragment | Endogenous 13-aa melanocortin hormone |
| Primary mechanism | PepT1 uptake; NF-kB inhibition | Angiogenesis; tissue-protective signaling | Melanocortin-receptor activation |
| Primary use model | Inflammation control; gut-barrier support | Structural tissue repair | Pigmentation; melanocortin signaling |
| Oral viability | Yes (PepT1) | Yes | Limited |
| Pigmentation effects | No | No | Yes |
| Clinical evidence | Preclinical only | Limited human + broad preclinical | Extensive hormonal research |
KPV and BPC-157 are commonly paired in gut-focused stacks because KPV emphasizes inflammation control while BPC-157 emphasizes structural repair.
KPV should not be confused with melanotan compounds. Pigmentation is not part of KPV's profile.
KPV Blood Tests & Monitoring
KPV is usually discussed in inflammation, gut, immune, and skin research. Monitoring focuses on broad inflammatory context, but labs may not capture local skin or gut response.
Blood test markers to discuss with a clinician
Marker
CBC with differential
Why it matters
Screens white-cell patterns, anemia, and immune context before interpreting inflammatory symptoms.
Timing
Baseline
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver, kidney, electrolyte, and glucose context in one broad panel.
Timing
Baseline
Marker
CRP
Why it matters
Adds a broad inflammation marker when systemic inflammation is part of the question.
Timing
Follow-up
Marker
ESR
Why it matters
Provides a slower-moving inflammation marker that may be useful for chronic symptoms.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| CBC with differential | Screens white-cell patterns, anemia, and immune context before interpreting inflammatory symptoms. | Baseline |
| Comprehensive metabolic panel (CMP) | Reviews liver, kidney, electrolyte, and glucose context in one broad panel. | Baseline |
| CRP | Adds a broad inflammation marker when systemic inflammation is part of the question. | Follow-up |
| ESR | Provides a slower-moving inflammation marker that may be useful for chronic symptoms. | Optional |
Monitoring guidance is immune and inflammation pathway-based because KPV has limited established human monitoring standards.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with autoimmune disease, gut symptoms, infection concern, liver disease, kidney disease, or immune medication use.
Follow-up
Repeat broad markers after 6-12 weeks if symptoms change or inflammation tracking is part of the research context.
Longer term
For longer immune or gut-focused protocols, review trends every 3-6 months with a clinician.
How to interpret the labs
- Gut, skin, and immune symptoms can change even when routine labs look normal.
- Autoimmune disease, infection risk, and immune-suppressing medications need clinician-guided interpretation.
- Avoid presenting KPV as a treatment or cure for inflammatory disease.
Do not wait for routine labs
Fever, bloody stool, severe abdominal pain, fast-spreading rash, or breathing symptoms need medical review.
FAQ
Q1: What is KPV peptide?
KPV is a three-amino-acid peptide (lysine-proline-valine) cut from the C-terminus of alpha-MSH, the body's natural anti-inflammatory hormone. It is researched mainly for anti-inflammatory and gut-barrier effects and skips the melanocortin-receptor pathway used by melanotan compounds.
Q2: What are KPV peptide benefits in research?
Preclinical and laboratory research has reported anti-inflammatory effects (especially in colitis and IBD models), antimicrobial activity against S. aureus and C. albicans, and skin-inflammation effects in animal and cell studies. No completed human trial has confirmed these effects in people.
Q3: What is the KPV peptide dosage in research planning?
The most-discussed range is 200-500 mcg daily, used either orally or subcutaneously. Some protocols extend up to 1,000 mcg daily, but this is not better supported than the standard range. No completed human dose-finding trial defines an official dose.
Q4: How is KPV reconstituted?
A common setup is 10 mg of lyophilized KPV with 2 mL of bacteriostatic water, giving a concentration of 5,000 mcg/mL. At that concentration, a 500 mcg dose equals 0.10 mL or 10 units on a U-100 insulin syringe. The full vial × BAC matrix is in the reconstitution section.
Q5: Can KPV be taken orally?
Yes. Oral KPV is a common research route, especially for gut-focused work, because KPV is absorbed through the PepT1 transporter in the small intestine. Oral protocols are typically taken on an empty stomach to reduce competition from dietary peptides.
Q6: What are KPV's main side effects?
Community reports are usually mild: transient injection-site irritation, occasional mild headache, and occasional GI discomfort at higher oral doses. Long-term safety is not established because no completed human trial has been published.
Q7: Does KPV cause tanning or pigmentation changes?
No. KPV does not bind the melanocortin receptors that drive melanotan-style pigmentation. It is generally modeled as non-pigmenting and should not be confused with melanotan compounds.
Q8: Is KPV FDA approved in 2026?
No. KPV is not FDA-approved. On April 22, 2026 the FDA removed KPV from Category 2 because the nomination was withdrawn. The Pharmacy Compounding Advisory Committee (PCAC) is scheduled to consult on KPV acetate and KPV free base on July 23, 2026 for potential inclusion on the 503A bulks list. Removal from Category 2 is not the same as FDA approval.
Q9: How does KPV compare to BPC-157 for gut research?
KPV and BPC-157 target different problems. KPV is studied for reducing inflammation through NF-kB inhibition. BPC-157 is studied for tissue repair through angiogenesis and protective signaling. They are commonly paired in gut-focused research stacks because the targets are complementary rather than overlapping.
Q10: What vial sizes is KPV available in?
The most common research-grade lyophilized vial sizes are 5 mg and 10 mg. Some suppliers offer larger vials, but 5 mg and 10 mg dominate research-use SKUs.
Q11: How should reconstituted KPV be stored?
Store reconstituted KPV refrigerated at 35.6-46.4F (2-8C), protect it from light, and use within about 30 days. Do not freeze the reconstituted solution. Lyophilized powder is stable at -4F (-20C) for long-term storage.
Q12: Is KPV dosing protocol guidance medical advice?
No. This page is an educational research reference. KPV is not FDA-approved, no completed human trial defines an optimal dose, and nothing on this page should replace consultation with a licensed clinician. Treat the dose ranges shown as research-context references, not as recommendations.
Sources & Research
- 1. Dalmasso G, Charrier-Hisamuddin L, et al. PepT1-mediated tripeptide KPV uptake reduces intestinal inflammation. Gastroenterology (2008)
- 2. Xiao B, Laroui H, et al. Orally targeted delivery of tripeptide KPV via hyaluronic acid-functionalized nanoparticles efficiently alleviates ulcerative colitis. Molecular Therapy (2017)
- 3. Brzoska T, Luger TA, Maaser C, et al. Alpha-MSH related peptides: a new class of anti-inflammatory and immunomodulating drugs. Annals of the Rheumatic Diseases (2008)
- 4. Catania A, et al. The neuropeptide alpha-MSH and inflammation: peripheral and central anti-inflammatory effects. Journal of Leukocyte Biology (2000)
- 5. Getting SJ. Targeting melanocortin receptors as potential novel therapeutics. Pharmacology & Therapeutics (2006)
- 6. Lee DJ, Kwon JY, et al. The therapeutic potential of melanocortin peptides in inflammatory bowel disease. Nature Reviews Gastroenterology and Hepatology (2018)
- 7. Wang W, et al. Melanocortin regulation of inflammation. Frontiers in Endocrinology (2019)
- 8. Star RA, Rajora N, et al. Evidence for autocrine modulation of macrophage nitric oxide synthase by alpha-melanocyte-stimulating hormone. PNAS (1995)
- 9. Rajora N, Boccoli G, et al. Alpha-MSH modulates experimental inflammatory bowel disease. Peptides (1997)
- 10. Lipton JM, et al. Anti-inflammatory effects of the neuropeptide alpha-MSH in acute, chronic, and systemic inflammation. Annals of the New York Academy of Sciences (1989)
- 11. U.S. Food and Drug Administration. Bulk drug substances nominated for use in compounding under 503A: Category 2 update (KPV removed from Category 2 effective April 22, 2026). FDA (2026)
- 12. SSRP Institute. FDA Announces Change in Status of 12 Peptides (April 15, 2026 announcement). Seeds Scientific Research & Performance (2026)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page