Semax Quick Start
Semax is a synthetic seven-amino-acid peptide (a heptapeptide) with the sequence Met-Glu-His-Phe-Pro-Gly-Pro. It was designed in Russia from a fragment of adrenocorticotropic hormone (ACTH) and a stabilizing Pro-Gly-Pro tail. The Pro-Gly-Pro tail was added to slow enzymatic breakdown so the molecule has a longer functional window than the bare ACTH fragment.
In Russian clinical practice, Semax (Russian: СЕМАКС) is on the country's Vital and Essential Drugs List and is used for stroke recovery, transient ischemic attack, cognitive disorders, and optic nerve disease. In the United States it is not FDA-approved, and as of April 23, 2026 it was removed from FDA's 503A Category 2 list of bulk substances flagged for compounding safety risks because the underlying nominations were withdrawn. It will be discussed at the FDA Pharmacy Compounding Advisory Committee meeting on July 24, 2026 for possible inclusion on the 503A Bulks List for cerebral ischemia and trigeminal neuralgia.
Route
Intranasal solution is the most-studied format. Subcutaneous injection from a reconstituted vial is also discussed in research planning.
Schedule
Daily administration is typical in research protocols, often divided into morning and afternoon doses to avoid late-day stimulation.
Measure (intranasal)
Bottles are usually labeled in mcg per spray or mcg per drop. Read the label, do not guess by counting drops.
Measure (injectable)
This guide assumes 20 mg lyophilized vials for injectable Semax math, requiring reconstitution with bacteriostatic water before subcutaneous research use.
Cycle
Russian-language clinical references commonly describe courses of several weeks followed by a break rather than continuous indefinite use.
Research status
Not FDA-approved. Removed from 503A Category 2 on April 23, 2026; PCAC review scheduled July 24, 2026.
Disclaimer
This page is an educational research reference and is not medical advice. Semax is not FDA-approved in the United States. Removal from FDA Category 2 does not authorize compounding or human use. Consult a qualified clinician for any health decision.
Semax Dosing Protocol & Schedule
Semax research planning splits cleanly by route. Intranasal solution is what dominates the published literature. Subcutaneous injection from a reconstituted research vial is less common in studies but is what most US-side research-use vials are sold for. The dose ranges below come from the published clinical literature in the corresponding routes — they are reported here as trial-context ranges, not as a dosing recommendation.
Semax Dosing Guide
Choose the format you are researching to see route-specific notes.
Less common in published research; relevant for those reconstituting a research-use lyophilized vial.
Subcutaneous Semax is much less common in the published literature than the intranasal route. The injectable math on this page assumes a 20 mg lyophilized research vial intended for reconstitution and subcutaneous research administration.
Russian clinical references and review summaries describe injectable Semax in research contexts at amounts up to about 1 mg per kilogram of body weight in some animal pharmacology models, but human subcutaneous research data is sparse. Any planning here should rely on vial concentration math (see the Reconstitution Guide section) rather than transferring intranasal numbers across routes. This is not a dosing recommendation.
Reported injectable Semax research ranges (trial-context only)
Context
Animal pharmacology (rodent)
Reported amount
Up to ~1 mg/kg
Notes
Not human-applicable; for context only
Source type
Animal pharmacology summaries
Context
Human research-community planning (subQ)
Reported amount
Sub-milligram per administration
Notes
Sparse direct human data
Source type
Community research planning, not formal trials
| Context | Reported amount | Notes | Source type |
|---|---|---|---|
| Animal pharmacology (rodent) | Up to ~1 mg/kg | Not human-applicable; for context only | Animal pharmacology summaries |
| Human research-community planning (subQ) | Sub-milligram per administration | Sparse direct human data | Community research planning, not formal trials |
Injectable subQ Semax has limited human evidence. Most strong data is intranasal.
Evidence boundary
If a research design depends on human-relevant Semax evidence, the intranasal literature is the strongest body of work. Subcutaneous research-context use exists, but does not have the same depth of published human data.
The format used in the majority of published Semax research, including stroke and cognitive studies.
Intranasal Semax is delivered as a nasal solution from a metered spray bottle or as drops. Bottles are commonly sold at concentrations such as 0.1% (1 mg/mL) or 1% (10 mg/mL), and the label should specify the amount delivered per spray or per drop.
Russian clinical references describe daily courses for cognitive and post-stroke contexts. A 1997 Russian clinical study in acute hemispheric ischemic stroke administered Semax intranasally during the acute period; the cognitive-research literature commonly reports total daily intranasal amounts in the milligram range divided across multiple administrations. This is not a dosing recommendation.
Reported intranasal Semax research ranges (trial-context only)
Context
Cognitive / nootropic research planning
Total daily amount (reported)
About 0.6 to 1.5 mg/day
Pattern (reported)
Split into 2 administrations (morning + early afternoon)
Source type
Russian clinical literature (Voronina 2023; Kaplan 1996)
Context
Acute ischemic stroke (clinical, Russia)
Total daily amount (reported)
Higher daily amounts under hospital supervision
Pattern (reported)
Multiple daily administrations during acute period
Source type
Gusev 1997 acute-stroke clinical study
Context
Healthy-volunteer cognitive-attention study
Total daily amount (reported)
Single intranasal administration of about 1.2 mg
Pattern (reported)
One-time research administration
Source type
ADDF Cognitive Vitality summary
| Context | Total daily amount (reported) | Pattern (reported) | Source type |
|---|---|---|---|
| Cognitive / nootropic research planning | About 0.6 to 1.5 mg/day | Split into 2 administrations (morning + early afternoon) | Russian clinical literature (Voronina 2023; Kaplan 1996) |
| Acute ischemic stroke (clinical, Russia) | Higher daily amounts under hospital supervision | Multiple daily administrations during acute period | Gusev 1997 acute-stroke clinical study |
| Healthy-volunteer cognitive-attention study | Single intranasal administration of about 1.2 mg | One-time research administration | ADDF Cognitive Vitality summary |
These are reported trial-context ranges and pharmacy summaries, not a dosing recommendation. Russian-language sources dominate, and protocol details vary by indication.
Cycle Guidelines (research-context)
Approach
Standard short course
Duration
10-14 days
Review point
End of course
Best for
Acute clinical research contexts in the literature
Approach
Extended cognitive course
Duration
4-6 weeks
Review point
Week 4
Best for
Cognitive performance research planning
Approach
Cycled use
Duration
4-6 weeks on, 2-4 weeks off
Review point
End of each cycle
Best for
Reducing tolerance signals reported in research-community discussions
| Approach | Duration | Review point | Best for |
|---|---|---|---|
| Standard short course | 10-14 days | End of course | Acute clinical research contexts in the literature |
| Extended cognitive course | 4-6 weeks | Week 4 | Cognitive performance research planning |
| Cycled use | 4-6 weeks on, 2-4 weeks off | End of each cycle | Reducing tolerance signals reported in research-community discussions |
Cycle structures are inferred from Russian clinical practice and community research planning. Continuous indefinite use is not common in published references.
Route boundary
Do not move research-context dosing from one route to another. A 1.2 mg intranasal amount and a 1.2 mg subcutaneous amount produce very different exposure profiles, and the published literature is not interchangeable across routes.
Semax Supplies Needed
Affiliate disclosure: PDP may earn a commission when you use eligible supplier links, at no extra cost to you. Supplies math below is for the subcutaneous research format using a 20 mg lyophilized vial reconstituted with 4 mL bacteriostatic water (final concentration: 5 mg/mL). Daily research planning of about 0.5 mg = 0.10 mL = 10 units on a U-100 syringe. Adjust if your protocol or reconstitution volume differs.
Recommended Supply
Use discount code SAVE10 at Peptira checkout. See why we love Peptira.
Semax

At-Home Blood Test
Research Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials (20 mg, subQ research format)
One 20 mg vial reconstituted with 4 mL bacteriostatic water yields about 40 daily research administrations of 0.5 mg.
| Cycle length | Planning note |
|---|---|
2-4 weeks 1 vial | 2 weeks: About 14 administrations needed; 1 vial provides 40 planned draws.; 4 weeks: About 28 administrations needed; 1 vial provides 40 planned draws. |
6-8 weeks 2 vials | 6 weeks: About 42 administrations needed; 2 vials provide 80 planned draws.; 8 weeks: About 56 administrations needed; 2 vials provide 80 planned draws. |
2-4 weeks
1 vial
2 weeks: About 14 administrations needed; 1 vial provides 40 planned draws.; 4 weeks: About 28 administrations needed; 1 vial provides 40 planned draws.
6-8 weeks
2 vials
6 weeks: About 42 administrations needed; 2 vials provide 80 planned draws.; 8 weeks: About 56 administrations needed; 2 vials provide 80 planned draws.
Insulin Syringes (U-100, 0.3 mL / 30 unit)
Smaller-barrel U-100 syringes are easier for sub-half-mL draws. One syringe per administration.
| Cycle length | Planning note |
|---|---|
2 weeks 14 syringes | 1 syringe per administration; recommend 1 x 100-count box. |
4 weeks 28 syringes | 1 syringe per administration; recommend 1 x 100-count box. |
6 weeks 42 syringes | Recommend 1 x 100-count box. |
8 weeks 56 syringes | Recommend 1 x 100-count box. |
2 weeks
14 syringes
1 syringe per administration; recommend 1 x 100-count box.
4 weeks
28 syringes
1 syringe per administration; recommend 1 x 100-count box.
6 weeks
42 syringes
Recommend 1 x 100-count box.
8 weeks
56 syringes
Recommend 1 x 100-count box.
Bacteriostatic Water
Use 4 mL per 20 mg vial. One 10 mL bottle reconstitutes two vials with margin for losses.
| Cycle length | Planning note |
|---|---|
2-8 weeks 1 x 10 mL bottle | 2 weeks: 1 vial uses 4 mL total.; 4 weeks: 1 vial uses 4 mL total.; 6 weeks: 2 vials use 8 mL total.; 8 weeks: 2 vials use 8 mL total; consider a second bottle if you want extra margin. |
2-8 weeks
1 x 10 mL bottle
2 weeks: 1 vial uses 4 mL total.; 4 weeks: 1 vial uses 4 mL total.; 6 weeks: 2 vials use 8 mL total.; 8 weeks: 2 vials use 8 mL total; consider a second bottle if you want extra margin.
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments. Intranasal users do not need vial / syringe / BAC water math; verify the bottle label for mcg per spray and total mg.
Companion Supplies & Routine Support
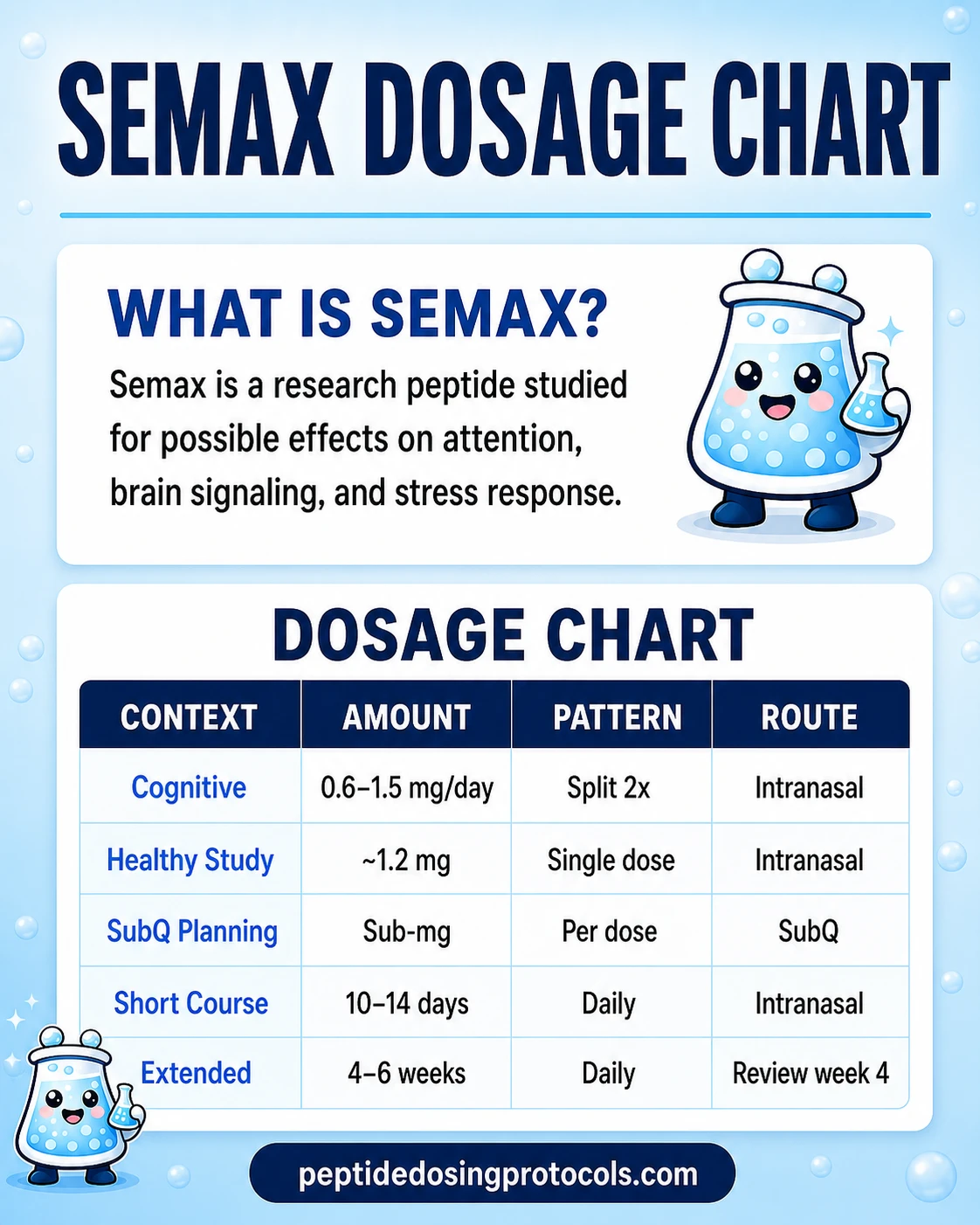
Semax Dosage Chart
This Semax dosage chart summarizes the intranasal and SubQ research-context dose ranges shown in the dosing section above.
Semax Reconstitution Guide
Reconstitution applies to the injectable / subcutaneous research format of Semax. Intranasal Semax solutions arrive pre-formulated and do not need to be reconstituted — verify the bottle's mcg-per-spray label instead.
Common Semax vial reconstitution math
Vial size
20 mg
BAC water added
2.0 mL
Final concentration
10.0 mg/mL
Example draw (0.5 mg)
0.05 mL = 5 units on U-100
Vial size
20 mg
BAC water added
4.0 mL
Final concentration
5.0 mg/mL
Example draw (0.5 mg)
0.10 mL = 10 units on U-100
Vial size
20 mg
BAC water added
5.0 mL
Final concentration
4.0 mg/mL
Example draw (0.5 mg)
0.125 mL = 12.5 units on U-100
| Vial size | BAC water added | Final concentration | Example draw (0.5 mg) |
|---|---|---|---|
| 20 mg | 2.0 mL | 10.0 mg/mL | 0.05 mL = 5 units on U-100 |
| 20 mg | 4.0 mL | 5.0 mg/mL | 0.10 mL = 10 units on U-100 |
| 20 mg | 5.0 mL | 4.0 mg/mL | 0.125 mL = 12.5 units on U-100 |
Pick a reconstitution volume that lands your typical research draw at a clean number on a U-100 insulin syringe. Higher BAC water volume = lower concentration = larger easier-to-read draw.
- 01
Inspect the vial
Check the label for compound name, total mg, and lot number. The lyophilized powder should be a clean white or off-white cake or pellet.
- 02
Wipe the stoppers
Use one alcohol swab on the bacteriostatic water vial stopper and another on the Semax vial stopper.
- 03
Draw the BAC water
Use a sterile syringe to draw your chosen volume (commonly 4 mL for a 20 mg vial).
- 04
Inject down the side wall
Insert the needle at an angle and let the bacteriostatic water run slowly down the inside of the Semax vial. Do not jet it directly onto the powder cake.
- 05
Swirl, do not shake
Gently swirl the vial in your hand until the powder fully dissolves. Vigorous shaking can foam the solution and stress the peptide.
- 06
Inspect the solution
Reconstituted Semax should be clear and colorless. Cloudiness, particles, or any floating material is a stop signal.
- 07
Label and store
Write the reconstitution date on the vial, then store refrigerated. Track the expected beyond-use window.
Calculator
If your vial size, BAC water volume, or planned amount differs from the table above, run the math through a peptide reconstitution calculator before drawing — small concentration errors become large dose errors quickly.
How Semax Works
Plain English first: Semax appears to nudge brain plasticity programs and stress-response biology, especially when the brain is under load. Researchers most often describe it through three overlapping mechanism layers — neurotrophin signaling, neurotransmitter modulation, and stress/ischemia gene expression. None of these layers fully explains the molecule on its own.
BDNF and TrkB signaling
Single intranasal Semax administration increased BDNF protein and TrkB receptor signaling in rat hippocampus (Dolotov 2006). This is the most-cited mechanism behind Semax's nootropic and neuroprotective framing.
Monoamine modulation
Semax has been reported to modulate dopaminergic and serotonergic systems in rodents, including amphetamine-evoked locomotor effects (Eremin 2005). This is described as neuromodulation, not classic stimulant action.
Melanocortin receptor interaction
Semax may act as a partial agonist or antagonist at MC4 and MC5 melanocortin receptors in vitro (Bertolini 2012). The full receptor profile is not settled.
Enkephalinase inhibition
Semax inhibits enkephalin-degrading enzymes from human serum at IC50 ~10 µM (Kost 2001), though the clinical significance of this property is uncertain.
Ischemia transcriptomics
Genome-wide transcriptional analysis in rat focal ischemia found Semax altered hundreds of genes, with notable clusters in immune response and vascular pathways (Medvedeva 2014).
A useful interpretation of the data: Semax appears most measurable when the brain is under a perturbation (stress, ischemia, fatigue, learning load) rather than as a constant baseline amplifier. This pattern fits the clinical literature too — the strongest reported effects are in stroke recovery and stress-research contexts, not in well-rested healthy volunteers.
Who Semax Is For and Who Should Avoid It
Semax is not a universal nootropic. The published research clusters around specific neurological and cognitive contexts, and several populations should not be treated as candidates outside formal medical care.
Where research interest is most consistent
Semax research interest concentrates in cerebral ischemia and stroke recovery, post-traumatic cognitive impairment, attention/memory under cognitive load, and stress-related conditions. The July 24, 2026 FDA PCAC review will specifically discuss Semax for cerebral ischemia and trigeminal neuralgia.
Populations that should avoid Semax outside clinician oversight
People with diabetes
ADDF and Russian-language safety summaries note Semax may raise blood glucose levels in people with diabetes.
Pregnant or breastfeeding individuals
There is not enough human research to evaluate fetal or infant safety. ADDF lists pregnancy and lactation as contraindications.
People with elevated baseline anxiety
A 1996 study described an anxiogenic component in some research subjects, suggesting Semax can amplify anxiety in already-anxious individuals. Calmer-feel goals are usually a better fit for Selank than Semax.
People taking psychiatric or stimulant medications
Semax interacts with monoaminergic systems in animal models. Combining with SSRIs, SNRIs, MAOIs, stimulants, or sleep-affecting drugs deserves clinician oversight.
Anyone using research-grade product without quality data
FDA's compounding-risk language specifically calls out aggregation and peptide-related impurities for Semax. Product quality and immunogenicity risk can exceed molecule risk.
Semax Side Effects & Safety
Semax safety reporting in accessible English-language literature is thin. The clearest summary comes from the Alzheimer's Drug Discovery Foundation (2020), which described 'very little human evidence for potential side effects' despite many preclinical trials. The 2022 Pharmaceutics review on Russian peptide biopharmaceuticals corroborates the low-toxicity framing.
Reported side effects
Nasal cavity discoloration (intranasal route)
ADDF reports approximately 10% of intranasal users experience nasal cavity discoloration.
Increased blood glucose
Reported specifically in people with diabetes.
Anxiety / overstimulation
Some users describe a 'too activated' feeling, especially when stacked with caffeine, stimulants, or used late in the day.
Nasal irritation, sneezing, dryness (intranasal route)
Local effects from nasal solution are common with frequent use.
Sleep disruption
Late-day use can interfere with sleep onset, especially at the upper end of research-context ranges.
Theoretical and product-level risks
FDA's 503A Category 2 listing (active September 29, 2023 to April 23, 2026) flagged Semax for immunogenicity risk for certain routes of administration due to potential for aggregation and peptide-related impurities. That risk is about how the molecule is manufactured, handled, and stored — not the molecule itself. Removal from Category 2 in April 2026 was a procedural withdrawal of nominations, not a safety clearance.
Quality matters more than dose
For a peptide used at sub-milligram amounts, batch contamination or aggregation can matter more than a 10-20% dose change. Documentation (HPLC purity, identity confirmation, endotoxin testing, batch-specific COA) should be the first sourcing checkpoint, not the last.
Semax Timeline & What to Monitor
Semax effect timelines reported in the literature and in research-community discussions vary by route and context. Intranasal effects are described as fast onset; neuroprotective and immunomodulatory signals take longer.
Reported Semax timeline signals (research-context)
Window
Same day (intranasal)
What is reported
Faster task initiation, sharper attention, reduced cognitive drag in some users
What not to overread
A single good work session does not validate the molecule; placebo and novelty are real
Window
First week
What is reported
Pattern of focus, mental stamina, and tolerability becomes more readable
What not to overread
Overstimulation, sleep disruption, or irritability appearing here is a stop-and-reassess signal
Window
2-4 weeks
What is reported
Cognitive consistency and any neuroprotective / immunomodulatory signals are described in this window in the literature
What not to overread
Daily-life subjective improvement does not equal evidence of neuroprotection
Window
End of cycle
What is reported
Whether baseline performance holds without continued use
What not to overread
Feeling unable to work without it is a tool-dependency signal, not a Semax success
| Window | What is reported | What not to overread |
|---|---|---|
| Same day (intranasal) | Faster task initiation, sharper attention, reduced cognitive drag in some users | A single good work session does not validate the molecule; placebo and novelty are real |
| First week | Pattern of focus, mental stamina, and tolerability becomes more readable | Overstimulation, sleep disruption, or irritability appearing here is a stop-and-reassess signal |
| 2-4 weeks | Cognitive consistency and any neuroprotective / immunomodulatory signals are described in this window in the literature | Daily-life subjective improvement does not equal evidence of neuroprotection |
| End of cycle | Whether baseline performance holds without continued use | Feeling unable to work without it is a tool-dependency signal, not a Semax success |
Timeline rows are reported research-community and literature observations, not guaranteed outcomes.
What is reasonable to monitor
A simple log of focus quality (1-10), stress (1-10), sleep quality (1-10), nasal tolerability (intranasal users), and side effects taken before starting and through the cycle is more honest than memory. For research planning that touches glucose-sensitive populations, baseline and on-cycle fasting glucose is a reasonable additional marker.
Semax Clinical Evidence Context
Direct human evidence summary: No published Western Phase 2 or Phase 3 randomized controlled trial exists for Semax. The strongest human evidence is Russian-language clinical experience — most notably acute ischemic stroke (Gusev 1997) and small healthy-volunteer cognitive studies. No FDA-approved indication exists in the United States.
Human evidence (acute ischemic stroke)
Gusev et al. 1997 reported improved neurological function in patients with acute hemispheric ischemic stroke after Semax administration in the acute period. The study is foundational to Russian clinical use of Semax.
Human evidence (healthy cognition)
Lebedeva 2018 reported effects on the brain's default mode network. Kaplan 1996 reported nootropic-like activity in healthy male participants under demanding cognitive conditions.
Preclinical (BDNF/TrkB)
Dolotov 2006 demonstrated single-administration BDNF and TrkB increases in rat hippocampus — the most-cited mechanistic anchor for the nootropic narrative.
Preclinical (ischemia transcriptomics)
Medvedeva 2014 (PMC3987924) and the 2020 PMC7350263 paper documented gene-expression changes in rat focal ischemia and ischemia-reperfusion models — important mechanism but not direct human stroke outcome data.
Preclinical (depression/anxiety models)
Inozemtseva 2024 reported antidepressant- and antistress-like effects in chronic unpredictable stress rat models, including BDNF normalization. Yatsenko 2013 reported similar attenuation of chronic stress effects.
Evidence boundary
There is no published head-to-head Western RCT comparing Semax against modafinil, racetams, caffeine + L-theanine, or placebo for cognitive performance in healthy adults. Confidence in everyday cognitive claims should be calibrated accordingly.
Semax Storage & Handling
Semax storage reference
State
Lyophilized (powder, sealed vial)
Storage
-4°F (-20°C) long-term; refrigerator (35.6-46.4°F / 2-8°C) short-term
Notes
Keep sealed and away from light. Verify supplier label.
State
Reconstituted (subcutaneous solution)
Storage
35.6-46.4°F (2-8°C)
Notes
Use within several weeks per supplier label and bacteriostatic water beyond-use guidance.
State
Intranasal solution
Storage
Most labels: refrigerator (35.6-46.4°F / 2-8°C) recommended; some manufacturers tolerate cool, dry storage below 50°F (10°C)
Notes
UK NIBSC reference recommends ~39°F (4°C). Verify the specific bottle label.
State
All forms
Storage
Out of direct sunlight; avoid temperature cycling
Notes
Repeated freeze-thaw or heat exposure increases aggregation risk.
| State | Storage | Notes |
|---|---|---|
| Lyophilized (powder, sealed vial) | -4°F (-20°C) long-term; refrigerator (35.6-46.4°F / 2-8°C) short-term | Keep sealed and away from light. Verify supplier label. |
| Reconstituted (subcutaneous solution) | 35.6-46.4°F (2-8°C) | Use within several weeks per supplier label and bacteriostatic water beyond-use guidance. |
| Intranasal solution | Most labels: refrigerator (35.6-46.4°F / 2-8°C) recommended; some manufacturers tolerate cool, dry storage below 50°F (10°C) | UK NIBSC reference recommends ~39°F (4°C). Verify the specific bottle label. |
| All forms | Out of direct sunlight; avoid temperature cycling | Repeated freeze-thaw or heat exposure increases aggregation risk. |
Aggregation risk is the central reason the FDA flagged Semax in 503A Category 2. Storage discipline is part of safety, not just stability.
Semax Protocol Mistakes & Troubleshooting
Cloudy or particulate solution
Stop use. Cloudiness or floating material in reconstituted Semax indicates degradation, contamination, or aggregation. Discard the vial.
Late-day administration ruining sleep
Community protocols typically shift administration earlier in the day. Sleep disruption that does not resolve within several days suggests the protocol may be a poor fit.
Feeling 'too activated' or anxious
Persistent irritability or overstimulation warrants clinician review before continuing. A calm-focus profile (Selank) may align differently with the research goal than a cognitive-push profile (Semax).
No noticeable effect after several weeks
Check route, label, concentration, and storage first. Many 'Semax does nothing' reports trace back to mislabeled bottles, drift in reconstitution math, or product-quality issues — not to the molecule.
Nasal irritation or sneezing on intranasal use
Reported practice alternates nostrils, allows time between sprays, and checks the formulation's preservative system. Persistent irritation is a stop signal.
Wrong reconstitution volume
Recalculate concentration before discarding the vial. A 20 mg vial reconstituted in 5 mL is still usable — the concentration is 4 mg/mL, and draw volume must adjust.
Storage mistake (left at room temperature)
Lyophilized powder is more tolerant than reconstituted solution. Reconstituted solution left out for hours raises aggregation and contamination risk; err toward discarding.
When to seek qualified medical care
Severe injection-site reaction, rash, breathing difficulty, sudden swelling, or any allergic-type response after Semax administration is a medical concern, not a protocol question. Stop use and seek qualified medical care.
Semax Regulatory Status
Semax regulatory status is in active transition in the United States and is unchanged in Russia/Eastern Europe.
United States — current status (June 2026)
Not FDA-approved
Semax is not an FDA-approved drug for any indication in the United States.
503A Category 2 history
Semax (heptapeptide) was placed on FDA's 503A Category 2 list of bulk substances flagged for compounding safety risks on September 29, 2023. The cited concern was immunogenicity risk from potential aggregation and peptide-related impurities for certain routes of administration.
April 23, 2026 — removal from Category 2
FDA removed Semax (along with BPC-157, KPV, MOTs-C, Emideltide / DSIP, Epitalon, and TB-500) from 503A Category 2 effective April 23, 2026 because the underlying nominations were withdrawn. Removal from Category 2 does not authorize compounding under Section 503A.
July 23-24, 2026 — PCAC meeting
FDA's Pharmacy Compounding Advisory Committee will meet July 23-24, 2026 (Federal Register Docket No. FDA-2026-N-2979). On July 24, 2026, the Committee will discuss Semax-related bulk drug substances (Semax free base / Semax acetate) for potential inclusion on the 503A Bulks List for cerebral ischemia and trigeminal neuralgia.
Research-use bulk substances
Material sold as 'research grade' or 'research use only' is not authorized for human use and has FDA-flagged immunogenicity and impurity concerns.
Other jurisdictions
Russia
Semax is a registered prescription pharmaceutical and is on the Russian Federation's List of Vital and Essential Drugs (added 2011). Approved indications include stroke, transient ischemic attack, cognitive disorders, optic nerve disease, and peptic ulcer.
European Union
Semax has not been evaluated or approved by the EMA. Most EU member states treat it as an unauthorized medicine.
United Kingdom
Semax is not authorized as a medicine by the MHRA. Sales of Semax nasal spray to UK consumers as a research chemical do not constitute medical authorization.
Regulatory boundary
The April 2026 Category 2 removal is procedural. It does not approve Semax for compounding, prescribing, or human use in the United States. Anyone considering clinician-directed Semax should track the July 2026 PCAC outcome and any subsequent rulemaking before assuming the situation has changed.
Semax vs Selank vs Common Nootropics
The dominant comparison query in Semax research is Selank vs Semax. Both are short Russian-origin synthetic peptides with a stabilizing Pro-Gly-Pro tail, both are most often discussed as intranasal solutions, and both are commonly grouped under 'Russian nootropic peptides.' They solve different problems.
Semax vs Selank vs caffeine + L-theanine vs modafinil
Option
Semax
Primary research focus
Cognitive activation, neuroprotection, ischemia/stress models
Typical route
Intranasal (most studied); subQ less common
Subjective profile
More activating, drive-leaning
Main caution
Overstimulation; FDA immunogenicity flag for compounded forms
Option
Selank
Primary research focus
Anxiolytic / GABAergic gene expression, stress modulation
Typical route
Intranasal (most discussed)
Subjective profile
Calmer, anxiety-reducing
Main caution
FDA Category 2 history (separate listing)
Option
Caffeine + L-theanine
Primary research focus
Alertness + smoothing
Typical route
Oral
Subjective profile
Stimulant + relaxation
Main caution
Tolerance, sleep disruption
Option
Modafinil
Primary research focus
Wakefulness promotion
Typical route
Oral, prescription
Subjective profile
Strong wakefulness, less direct cognition
Main caution
Prescription-only; interactions
| Option | Primary research focus | Typical route | Subjective profile | Main caution |
|---|---|---|---|---|
| Semax | Cognitive activation, neuroprotection, ischemia/stress models | Intranasal (most studied); subQ less common | More activating, drive-leaning | Overstimulation; FDA immunogenicity flag for compounded forms |
| Selank | Anxiolytic / GABAergic gene expression, stress modulation | Intranasal (most discussed) | Calmer, anxiety-reducing | FDA Category 2 history (separate listing) |
| Caffeine + L-theanine | Alertness + smoothing | Oral | Stimulant + relaxation | Tolerance, sleep disruption |
| Modafinil | Wakefulness promotion | Oral, prescription | Strong wakefulness, less direct cognition | Prescription-only; interactions |
Semax and Selank are not interchangeable. The simplest mental model: Semax for cognitive push, Selank for calm focus.
Stack research planning sometimes pairs Semax and Selank — sometimes called the Russian Nootropic Stack — to get both cognitive activation and calmer stress handling. That pairing is research-community planning, not a clinically validated combination.
Semax Blood Tests & Monitoring
Semax is usually discussed in nootropic, cognitive, and neurologic research. Routine labs do not directly measure cognitive response, so monitoring focuses on broad health context and medication interactions.
Blood test markers to discuss with a clinician
Marker
CBC with differential
Why it matters
Screens broad blood-cell patterns that can affect fatigue, focus, and general health interpretation.
Timing
Baseline
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver, kidney, electrolyte, and glucose context before interpreting energy or cognition changes.
Timing
Baseline
Marker
Blood pressure and resting heart rate
Why it matters
Adds cardiovascular context when stimulants, anxiety, headaches, or palpitations are part of the picture.
Timing
Optional
Marker
TSH and free T4
Why it matters
Thyroid imbalance can affect focus, mood, energy, and sleep.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| CBC with differential | Screens broad blood-cell patterns that can affect fatigue, focus, and general health interpretation. | Baseline |
| Comprehensive metabolic panel (CMP) | Reviews liver, kidney, electrolyte, and glucose context before interpreting energy or cognition changes. | Baseline |
| Blood pressure and resting heart rate | Adds cardiovascular context when stimulants, anxiety, headaches, or palpitations are part of the picture. | Optional |
| TSH and free T4 | Thyroid imbalance can affect focus, mood, energy, and sleep. | Optional |
Monitoring guidance is neurologic and medication-context based because Semax lacks established routine clinical lab-monitoring standards.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline review before starting, especially with neurologic history, psychiatric history, stimulant use, blood pressure concerns, liver disease, or kidney disease.
Follow-up
Repeat broad labs after 8-12 weeks if symptoms change or the protocol continues.
Longer term
For recurring protocols, review cognition, mood, sleep, blood pressure, and medication changes periodically.
How to interpret the labs
- Routine labs do not prove a nootropic effect.
- Medication interactions, stimulants, sleep, anxiety, and neurologic history matter during interpretation.
- Track symptoms and function alongside labs instead of relying on labs alone.
Do not wait for routine labs
Severe headache, neurologic symptoms, chest pain, confusion, mania symptoms, or suicidal thoughts need medical review.
FAQ
Q1: What is Semax peptide?
Semax is a synthetic seven-amino-acid peptide (a heptapeptide) with the sequence Met-Glu-His-Phe-Pro-Gly-Pro. It is derived from a fragment of adrenocorticotropic hormone (ACTH) with an added Pro-Gly-Pro tail for stability, and is most commonly studied as an intranasal nootropic and neuroprotective peptide.
Q2: What does Semax do?
Semax is reported to nudge brain plasticity programs and stress-response biology rather than acting as a classical stimulant. It has been associated with increased BDNF and TrkB signaling in rodent brain studies, modulation of dopamine and serotonin systems, and gene-expression changes in ischemia models. Effects are most measurable when the brain is under load.
Q3: Is Semax FDA-approved?
No. Semax is not an FDA-approved drug in the United States. It was placed on FDA's 503A Category 2 list of bulk substances flagged for compounding safety risks in September 2023 and removed from that list on April 23, 2026 after the underlying nominations were withdrawn. Removal from Category 2 does not authorize compounding. The Pharmacy Compounding Advisory Committee will discuss Semax for possible inclusion on the 503A Bulks List on July 24, 2026, specifically for cerebral ischemia and trigeminal neuralgia.
Q4: What is a typical Semax dosage in research planning?
Total daily intranasal amounts in the cognitive research literature commonly fall around 0.6 to 1.5 mg per day, divided across two administrations. Acute-stroke clinical research used higher amounts under hospital supervision. Subcutaneous research-context amounts are sub-milligram per administration. These are reported trial-context ranges, not a dosing recommendation. PDP does not publish personalized Semax dosing protocols.
Q5: Selank vs Semax — what is the difference?
Both are short Russian-origin synthetic peptides with a Pro-Gly-Pro stabilizing tail, and both are most commonly discussed as intranasal solutions. Semax is associated with cognitive activation, focus, and neuroprotection (ACTH-derived). Selank is associated with anxiolytic and stress-modulating effects (tuftsin-derived, GABAergic gene-expression involvement). The simplest framing is: Semax for cognitive push, Selank for calm focus.
Q6: Is Semax nasal spray legal in the UK?
Semax is not authorized as a medicine by the UK Medicines and Healthcare products Regulatory Agency (MHRA). Sales of Semax nasal solution to UK consumers as a 'research chemical' do not constitute medical authorization or approval for human use.
Q7: Can Semax and Selank be used together?
Combining Semax and Selank is a research-community planning concept sometimes called the Russian Nootropic Stack. The logic is to pair cognitive activation (Semax) with calmer stress handling (Selank). The combination is not a clinically validated protocol, and FDA has flagged compounding-related risks for both peptides.
Q8: How fast does Semax work?
Intranasal Semax is described as fast-onset, with same-day effects on attention or task initiation reported by some users. Neuroprotective and immunomodulatory signals in the literature take longer (typically 2-4 weeks of consistent administration). Subjective reports vary widely, and a single session is not sufficient to evaluate the molecule.
Q9: What are Semax side effects?
Reported side effects include nasal cavity discoloration in approximately 10% of intranasal users (per the Alzheimer's Drug Discovery Foundation summary), increased blood glucose in people with diabetes, overstimulation or anxiety in sensitive users, nasal irritation with frequent intranasal use, and sleep disruption with late-day administration. FDA's compounding-risk language additionally flags potential immunogenicity from aggregation and peptide-related impurities for certain routes.
Q10: Is research-grade Semax safe for human use?
No. Material sold as 'research grade' or 'research use only' is not authorized for human use and is the specific category FDA flagged for immunogenicity risk from aggregation and peptide-related impurities. Quality, identity, and purity documentation can vary widely between sellers, and product-level risk can exceed molecule-level risk for a peptide used at sub-milligram amounts.
Q11: Is this Semax page medical advice?
No. This page is an educational research reference for Semax (heptapeptide) and is not medical advice, a prescription, or a recommendation to use the substance. Semax is not FDA-approved in the United States. Consult a qualified clinician for any health decision involving Semax or related peptides.
Sources & Research
- 1. U.S. Food and Drug Administration Certain Bulk Drug Substances for Use in Compounding that May Present Significant Safety Risks (503A Category 2 list). FDA.gov (2025)
- 2. U.S. Food and Drug Administration July 23-24, 2026: Meeting of the Pharmacy Compounding Advisory Committee — Semax (free base / acetate) for cerebral ischemia and trigeminal neuralgia. FDA.gov / Federal Register Docket FDA-2026-N-2979 (2026)
- 3. Federal Register / FDA Pharmacy Compounding Advisory Committee Notice of Meeting and Establishment of Public Docket — peptide nominations for 503A Bulk Drug Substances List. Federal Register (2026)
- 4. Voronina TA Cognitive Impairment and Nootropic Drugs: Mechanism of Action and Spectrum of Effects. Neurochemical Journal (2023)
- 5. Dolotov OV, Karpenko EA, Inozemtseva LS, et al. Semax, an analog of ACTH(4-10) with cognitive effects, regulates BDNF and trkB expression in the rat hippocampus. Brain Research (2006)
- 6. Eremin KO, Kudrin VS, Saransaari P, et al. Semax, an ACTH(4-10) analogue with nootropic properties, activates dopaminergic and serotoninergic brain systems in rodents. Neurochemical Research (2005)
- 7. Bertolini A Drug-induced activation of the nervous control of inflammation: a novel possibility for the treatment of hypoxic damage. European Journal of Pharmacology (2012)
- 8. Kost NV, Sokolov OI, Gabaeva MV, et al. Semax and selank inhibit the enkephalin-degrading enzymes from human serum. Bioorganicheskaia Khimiia (2001)
- 9. Medvedeva EV, Dmitrieva VG, Povarova OV, et al. The peptide semax affects the expression of genes related to the immune and vascular systems in rat brain focal ischemia: genome-wide transcriptional analysis. BMC Genomics (PMC3987924) (2014)
- 10. Filippenkov IB, Stavchansky VV, Glazova NY, et al. Novel Insights into the Protective Properties of ACTH(4-7)PGP (Semax) Peptide at the Transcriptome Level Following Cerebral Ischaemia-Reperfusion in Rats. Genes (PMC7350263) (2020)
- 11. Inozemtseva LS, Karpenko EA, Dolotov OV, et al. Antidepressant-like and antistress effects of the ACTH(4-10) synthetic analogs Semax and Melanotan II on male rats in a model of chronic unpredictable stress. European Journal of Pharmacology (2024)
- 12. Gusev EI, Skvortsova VI, Miasoedov NF, et al. Effectiveness of Semax in the acute period of hemispheric ischemic stroke (a clinical and electrophysiological study). Zhurnal Nevrologii i Psikhiatrii imeni S.S. Korsakova (1997)
- 13. Deigin VI, Poluektova EA, Beniashvili AG, et al. Development of Peptide Biopharmaceuticals in Russia. Pharmaceutics (PMC9030433) (2022)
- 14. Alzheimer's Drug Discovery Foundation Semax — Cognitive Vitality for Researchers (safety and evidence summary). ADDF (2020)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page