Humanin Quick Start
Humanin is a small mitochondrial-derived peptide. It is one of the first peptides shown to be encoded inside mitochondrial DNA rather than the cell nucleus. Researchers study it for its role in cell survival, mitochondrial function, and aging biology.
Most published research uses HNG, a synthetic version of humanin where one amino acid has been swapped at position 14. HNG is more stable and reportedly more potent than native humanin, so almost every animal dosing protocol on the public record uses HNG, not native humanin.
There is no published human randomized trial that has used humanin or HNG as a therapy. Everything below is a research-planning reference, not a treatment plan, and it is not medical advice.
Route
Subcutaneous (SC) is the most commonly described route in research planning. Animal studies often use intraperitoneal (IP).
Schedule
Animal HNG protocols use twice-weekly dosing. Research-context plans describe daily to 3x/week.
Cycle length
Cycles described in the research-use community are typically 4-12 weeks, with off periods.
Measure
U-100 insulin syringes after reconstitution with bacteriostatic water.
Research status
Not FDA-approved. No published human RCT of exogenous humanin or HNG as of June 2026.
Disclaimer
This page is an educational research reference and is not medical advice. Humanin is not approved by the FDA for any condition. Do not start any peptide protocol without qualified medical oversight.
Humanin Dosing Protocol & Schedule
There is no formal human clinical dose for humanin or HNG. The protocols below summarize what published animal research has used and what the research-use community has discussed for planning. None of this is a dosing recommendation.
Most-cited animal HNG protocol
The clearest reference point in the literature is HNG at 4 mg/kg, intraperitoneal, twice weekly, used in 18-month-old female C57BL/6N mice in the Yen et al. healthspan study and the Qin et al. cardiac fibrosis study. That protocol is reported across multiple peer-reviewed papers and is the dose researchers cite most often. This is not a dosing recommendation.
Reported Research-Context Dosing Ranges
Setting
Healthspan study (mice)
Compound
HNG
Dose
4 mg/kg
Route
IP
Frequency
2x/week, midlife start
Source
Yen et al., Aging, 2020
Setting
Cardiac fibrosis study (mice)
Compound
HNG
Dose
4 mg/kg
Route
IP
Frequency
2x/week, 14 months
Source
Qin et al., Am J Physiol Heart Circ Physiol, 2018
Setting
Metabolomic study (DIO mice)
Compound
HNG
Dose
2.5 mg/kg/injection
Route
IP
Frequency
2x/day, 3 days
Source
Mehta et al., 2019
Setting
Research-use planning (community)
Compound
Humanin or HNG
Dose
Subcutaneous milligram-range per session described in community discussion
Route
SC
Frequency
Varies, daily to 2-3x/week
Source
Community planning, not clinical evidence
| Setting | Compound | Dose | Route | Frequency | Source |
|---|---|---|---|---|---|
| Healthspan study (mice) | HNG | 4 mg/kg | IP | 2x/week, midlife start | Yen et al., Aging, 2020 |
| Cardiac fibrosis study (mice) | HNG | 4 mg/kg | IP | 2x/week, 14 months | Qin et al., Am J Physiol Heart Circ Physiol, 2018 |
| Metabolomic study (DIO mice) | HNG | 2.5 mg/kg/injection | IP | 2x/day, 3 days | Mehta et al., 2019 |
| Research-use planning (community) | Humanin or HNG | Subcutaneous milligram-range per session described in community discussion | SC | Varies, daily to 2-3x/week | Community planning, not clinical evidence |
These are research protocols and community-derived planning references. There is no FDA-approved label dose for humanin or HNG. This is not a dosing recommendation.
Cycle structure
Animal protocols have used continuous, multi-month dosing. In community research-use planning, common cycle structures are 4 weeks, 6-8 weeks, and 12 weeks, with an off period of similar length. Long-term human safety has not been characterized.
Cycle Guidelines
Approach
Short
Duration
4 weeks
Review Point
Week 4
Notes
Common entry length for community research-use planning
Approach
Standard
Duration
6-8 weeks
Review Point
Week 6
Notes
Most common cycle length in research-use planning
Approach
Extended
Duration
12 weeks
Review Point
Week 8 and Week 12
Notes
Used in animal studies; human equivalent is unstudied
| Approach | Duration | Review Point | Notes |
|---|---|---|---|
| Short | 4 weeks | Week 4 | Common entry length for community research-use planning |
| Standard | 6-8 weeks | Week 6 | Most common cycle length in research-use planning |
| Extended | 12 weeks | Week 8 and Week 12 | Used in animal studies; human equivalent is unstudied |
Cycles are research-planning references only and not medical recommendations.
Evidence boundary
There is no published human randomized clinical trial of exogenous humanin or HNG as of June 2026. Translating animal protocols to human use carries unknown risk, and any human dosing reference is extrapolation, not evidence.
Humanin Supplies Needed
Math below assumes a 20 mg humanin (or HNG) vial reconstituted with 2 mL bacteriostatic water (10 mg/mL) and a research-planning dose of about 1 mg per session, dosed 3 times per week.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

Humanin Vial

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials
Math assumes a 20 mg vial of humanin or HNG. A 1 mg session dose gives 20 sessions per vial.
| Cycle length | Planning note |
|---|---|
4-6 weeks 1 vial | 4 weeks: About 12 sessions at 3x/week; one vial gives about 8 sessions of margin; 6 weeks: About 18 sessions at 3x/week; one vial gives about 2 sessions of margin |
8-12 weeks 2 vials | 8 weeks: About 24 sessions at 3x/week; second vial gives margin; 12 weeks: About 36 sessions at 3x/week; two vials give about 4 sessions of margin |
4-6 weeks
1 vial
4 weeks: About 12 sessions at 3x/week; one vial gives about 8 sessions of margin; 6 weeks: About 18 sessions at 3x/week; one vial gives about 2 sessions of margin
8-12 weeks
2 vials
8 weeks: About 24 sessions at 3x/week; second vial gives margin; 12 weeks: About 36 sessions at 3x/week; two vials give about 4 sessions of margin
Insulin Syringes (U-100)
One syringe per session. 0.3 mL syringes work well for a 0.10 mL draw at 10 mg/mL.
| Cycle length | Planning note |
|---|---|
4 weeks 12 syringes | 1 syringe per session |
6 weeks 18 syringes | 1 syringe per session |
8 weeks 24 syringes | 1 syringe per session |
12 weeks 36 syringes | 1 syringe per session |
4 weeks
12 syringes
1 syringe per session
6 weeks
18 syringes
1 syringe per session
8 weeks
24 syringes
1 syringe per session
12 weeks
36 syringes
1 syringe per session
Bacteriostatic Water
2 mL per 20 mg vial gives 10 mg/mL. One 10 mL bottle covers most cycles.
| Cycle length | Planning note |
|---|---|
4-12 weeks 1 x 10 mL bottle | 4 weeks: 1 vial uses 2 mL total; 6 weeks: 1 vial uses 2 mL total; 8 weeks: 2 vials use 4 mL total; 12 weeks: 2 vials use 4 mL total |
4-12 weeks
1 x 10 mL bottle
4 weeks: 1 vial uses 2 mL total; 6 weeks: 1 vial uses 2 mL total; 8 weeks: 2 vials use 4 mL total; 12 weeks: 2 vials use 4 mL total
Round up for priming losses, dropped syringes, damaged swabs, and any protocol adjustments. Adjust the math if the supplier sells a different vial size or if the planned dose differs.
Companion Supplies & Routine Support
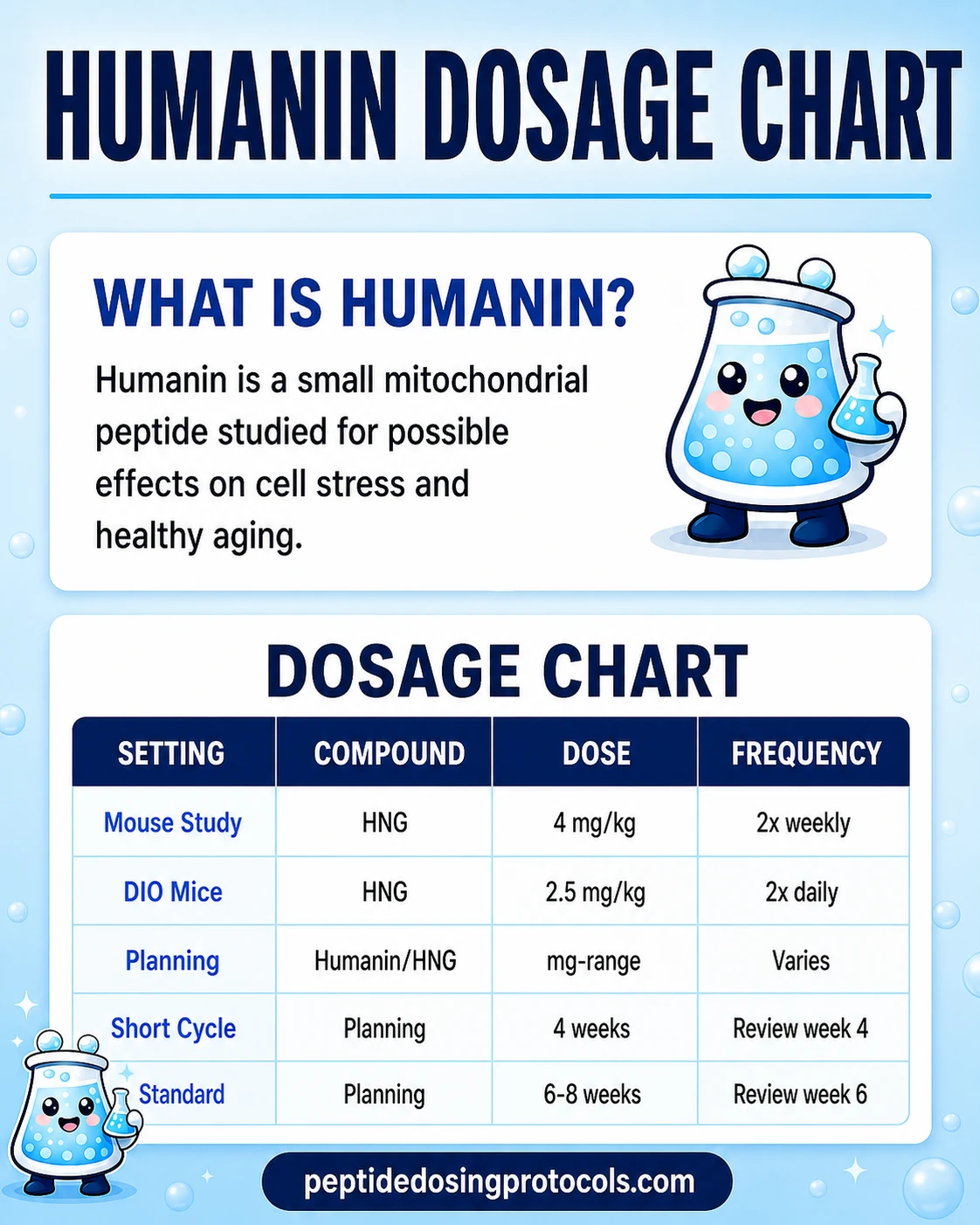
Humanin Dosage Chart
This Humanin dosage chart summarizes the HNG animal-study dosing and community research-planning cycle ranges shown in the dosing section above.
Humanin Reconstitution Guide
Humanin and HNG ship as a freeze-dried (lyophilized) powder inside a glass vial. Before use, the powder is mixed with bacteriostatic water (BAC water) so it can be drawn into a syringe. Always check the actual amount printed on the vial because suppliers sell different sizes.
Reconstitution Math (20 mg vial example)
Setting
Vial size
Value
20 mg
Setting
BAC water added
Value
2.0 mL
Setting
Final concentration
Value
10 mg/mL
Setting
1 mg session dose
Value
0.10 mL = 10 units on a U-100 syringe
Setting
0.5 mg session dose
Value
0.05 mL = 5 units on a U-100 syringe
| Setting | Value |
|---|---|
| Vial size | 20 mg |
| BAC water added | 2.0 mL |
| Final concentration | 10 mg/mL |
| 1 mg session dose | 0.10 mL = 10 units on a U-100 syringe |
| 0.5 mg session dose | 0.05 mL = 5 units on a U-100 syringe |
Adjust the math to match the actual vial size on the label.
- 01
Inspect the vial
Check the label for compound name (humanin vs HNG), amount in mg, lot number, and expiration. Make sure the vial is sealed and the powder cake looks intact.
- 02
Wipe the stoppers
Use a fresh alcohol swab on the BAC water vial stopper and the peptide vial stopper. Let them air-dry.
- 03
Draw BAC water
Draw 2.0 mL of bacteriostatic water into a clean syringe. Use a larger reconstitution syringe (3 mL) to make this easier.
- 04
Add slowly down the side
Insert the needle into the peptide vial at an angle and let the BAC water run down the inside of the glass instead of hitting the powder cake directly.
- 05
Swirl, do not shake
Swirl the vial gently until the powder dissolves. Vigorous shaking can damage peptides.
- 06
Inspect the solution
It should be clear or very faintly colored. Do not use cloudy, foamy, or particulate solutions.
- 07
Label and store
Mark the date on the vial. Refrigerate after reconstitution, ideally between 35.6 and 46.4F (2-8C).
Calculator
Use the Peptide Dosing Calculator to confirm draw volumes for your specific vial size and planned session dose.
How Humanin Works
Humanin is a small peptide encoded inside mitochondrial DNA. Most peptides in the body are encoded by the cell nucleus, so a peptide written in mitochondrial DNA is unusual. Humanin acts as a stress signal from the mitochondria back to the rest of the cell.
Two mechanisms come up most often in published research. First, humanin binds to the pro-apoptotic protein BAX and prevents BAX from triggering programmed cell death. Second, humanin acts as a ligand at cell-surface receptors including FPRL1 and a trimeric receptor made up of CNTFR, gp130, and WSX-1, which can activate STAT3 signaling and other survival pathways.
Humanin has also been shown to activate chaperone-mediated autophagy. That is the process the cell uses to identify damaged proteins and send them to lysosomes for clean-up. Together, these mechanisms are why humanin is described as a cytoprotective and stress-response peptide.
What is HNG?
HNG is a synthetic version of humanin where the serine at position 14 is swapped for glycine. That single change makes HNG more stable and substantially more potent than native humanin. Most of the published animal work uses HNG, not native humanin.
Who Humanin Is For and Who Should Avoid It
Humanin is a research-use peptide. It is not a treatment, not a supplement, and not a medical product. The list below describes situations where humanin or HNG would carry extra theoretical risk and where qualified clinical oversight matters most.
- Active or recent cancer history. Humanin blocks BAX-mediated apoptosis, and BAX is part of the system the body uses to remove damaged cells. The implications for cancer surveillance are not well understood.
- Pregnancy or lactation. There is no safety data in pregnant or lactating humans.
- Children and adolescents. There is no human safety data in any age group, and even less in growing individuals.
- Patients on insulin or insulin-secretagogues. Humanin and HNG have insulin-sensitizing effects in animal studies; combining them with other glucose-lowering agents could be unpredictable.
- Active autoimmune or inflammatory disease. Humanin has anti-inflammatory effects, and any change to inflammatory tone should be discussed with a qualified clinician.
- Anyone unable to access qualified medical oversight, lab monitoring, or sterile injection conditions.
Humanin Side Effects & Safety
There is no human clinical trial dataset for exogenous humanin or HNG. The safety statements below are based on animal studies, mechanism, and general subcutaneous-injection risk. Long-term safety is unknown.
Reported and expected effects
- Injection site reactions: redness, mild swelling, or transient discomfort at the SC injection site.
- Mild fatigue or lethargy: anecdotally reported in research-use community planning, not characterized in trials.
- Headache: uncommon, typically mild when reported anecdotally.
- Transient nausea: more often described at higher doses or with IV administration.
Theoretical risks
- Cancer surveillance concern. Humanin's anti-apoptotic effect through BAX inactivation is the clearest theoretical concern, especially for anyone with a personal or family history of cancer.
- Glucose handling. Insulin sensitization is a feature in animal models, which means glucose handling could shift in users on existing diabetes therapy.
- Immune effects. Pharmacological doses well above natural endogenous levels could shift inflammatory tone in ways that have not been characterized in humans.
Quality and route-specific risk
- Quality control. Research peptides are not FDA-regulated as drugs. Purity and accuracy of label depend on the supplier.
- Contamination risk. Improper reconstitution, dirty syringes, or non-sterile BAC water can introduce infection risk regardless of the peptide.
- Half-life. Native humanin has a short circulating half-life of about 30 minutes, which is part of why HNG was developed and is more commonly used in research.
Bottom line on safety
No human RCT exists for humanin or HNG as of June 2026. Animal studies have not flagged major adverse signals at the doses tested, but those studies were not designed to characterize human safety.
Humanin Timeline & What to Monitor
Humanin does not act like a stimulant. The endpoints studied in animal research are slow-changing: cardiac fibrosis was assessed over 14 months in mice, healthspan markers shifted over weeks, and metabolic markers like body composition changed over months of dosing.
What changes were measured in research
- Body composition shifts over weeks to months in HNG-treated middle-aged mice (lower visceral fat, higher lean body mass).
- Inflammatory markers like IL-6 and Iba-1 declined in aging mice over months of HNG dosing.
- Cognitive performance markers and rotarod motor function improved in aged mice on HNG over the dosing window.
- Cardiac fibrosis declined and cardiomyocyte-to-fibroblast ratio improved in 32-month-old mice receiving HNG for 14 months.
What is reasonable to monitor in research-use planning
- Baseline and follow-up labs with qualified clinical oversight: glucose, HbA1c, lipid panel, inflammatory markers, complete blood count.
- Symptom journal: sleep quality, energy, injection-site response, any unusual symptom.
- Stop-and-review point at week 4 and week 8 to compare change against baseline.
What cannot be promised
Animal endpoint changes do not guarantee any human outcome. There is no validated biomarker for humanin response in humans.
Humanin Clinical Evidence Context
There is no published human randomized clinical trial of exogenous humanin or HNG as a therapy as of June 2026. Most evidence is preclinical or comes from observational human plasma studies linking endogenous humanin levels to health outcomes.
Human evidence (observational)
Conte et al. 2019 measured plasma humanin in 693 subjects aged 21 to 113 years. FGF21, GDF15, and humanin all increased with age, with the highest levels found in centenarians, suggesting a stress-response role rather than simple deficiency in aging.
Human evidence (offspring of long-lived)
Yen et al. 2020 reported that children of centenarians showed higher circulating humanin than age-matched controls, supporting a longevity-association signal in observational data.
Animal evidence (healthspan)
Yen et al. 2020 administered HNG 4 mg/kg IP twice weekly to 18-month-old female mice. Treatment improved metabolic healthspan markers, lowered visceral fat, and increased lean body mass.
Animal evidence (cardiac)
Qin et al. 2018 administered HNG 4 mg/kg IP twice weekly to mice from 18 to 32 months. Treatment reduced age-related myocardial fibrosis, lowered cardiomyocyte apoptosis, and partially reversed the cardiomyocyte-to-fibroblast ratio toward young-mouse values.
Animal evidence (cardioprotection)
Sharp et al. 2020 translated cardioprotection from rodents to a porcine ischemia-reperfusion model, where a single IV HNG dose at reperfusion reduced infarct size after 60 minutes of ischemia, but not after 75 minutes, indicating a window-dependent effect.
Mechanism evidence
Humanin binds BAX to block apoptosis, activates STAT3 via FPRL1 and CNTFR/gp130/WSX-1, and triggers chaperone-mediated autophagy via HSP90 stabilization at the lysosomal membrane.
Evidence gap
No published human RCT of exogenous humanin or HNG. No FDA-approved humanin product as of June 2026. All human dosing references are extrapolations.
Humanin Storage & Handling
Humanin Storage
State
Lyophilized (powder form)
Storage
-4F (-20C) long-term
Notes
Use the supplier label and stability data. Protect from light and moisture.
State
Reconstituted (liquid form)
Storage
35.6-46.4F (2-8C)
Notes
Native humanin has stability concerns; HNG can degrade more slowly. Use within the supplier-stated beyond-use window.
State
Travel and short-term
Storage
35.6-46.4F (2-8C)
Notes
Keep in an insulated cooler with cold packs; avoid freezing the reconstituted vial.
| State | Storage | Notes |
|---|---|---|
| Lyophilized (powder form) | -4F (-20C) long-term | Use the supplier label and stability data. Protect from light and moisture. |
| Reconstituted (liquid form) | 35.6-46.4F (2-8C) | Native humanin has stability concerns; HNG can degrade more slowly. Use within the supplier-stated beyond-use window. |
| Travel and short-term | 35.6-46.4F (2-8C) | Keep in an insulated cooler with cold packs; avoid freezing the reconstituted vial. |
If a vial has been left at room temperature for extended periods, defer to the supplier's stability data and consider replacing the vial.
Humanin Protocol Mistakes & Troubleshooting
- 01
Vial looks cloudy after reconstitution
Do not use it. Cloudiness or particulate matter can indicate contamination or degraded peptide. Discard and start fresh with a new vial.
- 02
Wrong BAC water volume
If you added 1.0 mL instead of 2.0 mL to a 20 mg vial, the concentration doubles to 20 mg/mL and every draw delivers twice the planned dose. Recalculate before injecting.
- 03
Missed a session
Resume on the next scheduled day. Do not double-dose to catch up.
- 04
Injection site reaction that does not resolve
Stop dosing and seek qualified medical advice. Persistent redness, swelling, or warmth at a site can indicate infection.
- 05
No noticeable change after 4-6 weeks
Humanin acts slowly and on cellular endpoints, not subjective energy. Use objective markers (labs, body composition, sleep tracking) instead of subjective day-to-day feel.
- 06
Confusion between humanin and HNG
Read the supplier label. Native humanin and HNG are different molecules; HNG is more potent and more stable. Match the protocol you are referencing to the compound on the label.
- 07
Storage mistake
If a reconstituted vial sat at room temperature far longer than the supplier's beyond-use window, replace it. Do not inject anything you are unsure about.
Humanin Regulatory Status
As of June 2026, neither humanin nor HNG is approved by the FDA, EMA, or any other major regulator for any condition. There is no FDA-approved label, no AbbreviateD New Drug Application, and no approved compounded product for humanin or HNG.
Humanin and HNG are sold by research-use peptide suppliers as research chemicals. Research-use products are not regulated as drugs and are not intended for human use. Individual states and countries vary in how they treat possession, sale, and import of research peptides; verify current rules before ordering.
Humanin vs MOTS-c vs SS-31
Humanin sits in a small family of mitochondrial-derived peptides (MDPs). The two most-discussed peers are MOTS-c, also encoded inside mitochondrial DNA, and SS-31, a synthetic mitochondria-targeting peptide. They are not interchangeable.
Mitochondrial-Related Peptides
Peptide
Humanin
Origin
Encoded in mitochondrial 16S rRNA region; 24 amino acids
Primary research interest
Cytoprotection, neuroprotection, metabolic and cardiac aging models
Approval status
Not FDA-approved
Peptide
MOTS-c
Origin
Encoded in mitochondrial 12S rRNA region; 16 amino acids
Primary research interest
Skeletal-muscle metabolism, insulin sensitivity, exercise biology
Approval status
Not FDA-approved
Peptide
SS-31 (elamipretide)
Origin
Synthetic, not mitochondrial-encoded
Primary research interest
Mitochondrial cardiolipin protection; investigated in primary mitochondrial disease and Barth syndrome trials
Approval status
Not FDA-approved (April 2025 FDA accelerated approval pathway concerns reported; verify current status)
| Peptide | Origin | Primary research interest | Approval status |
|---|---|---|---|
| Humanin | Encoded in mitochondrial 16S rRNA region; 24 amino acids | Cytoprotection, neuroprotection, metabolic and cardiac aging models | Not FDA-approved |
| MOTS-c | Encoded in mitochondrial 12S rRNA region; 16 amino acids | Skeletal-muscle metabolism, insulin sensitivity, exercise biology | Not FDA-approved |
| SS-31 (elamipretide) | Synthetic, not mitochondrial-encoded | Mitochondrial cardiolipin protection; investigated in primary mitochondrial disease and Barth syndrome trials | Not FDA-approved (April 2025 FDA accelerated approval pathway concerns reported; verify current status) |
Humanin and MOTS-c are both mitochondrial-derived peptides but target different pathways. SS-31 is structurally unrelated and developed as a small synthetic mitochondria-targeting compound.
Related compound: MOTS-c
If you are researching mitochondrial-derived peptides for metabolic and exercise-related interest, MOTS-c is the closest peer to humanin in this family. View MOTS-c protocol.
Humanin Blood Tests & Monitoring
Humanin is usually discussed in mitochondrial, metabolic, and aging research. Monitoring is broad because compound-specific clinical lab standards are not established.
Blood test markers to discuss with a clinician
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver, kidney, electrolyte, and glucose context before interpreting energy or metabolic changes.
Timing
Baseline
Marker
A1c
Why it matters
Shows the longer-term blood sugar pattern relevant to metabolic-health research.
Timing
Baseline
Marker
Lipid panel
Why it matters
Tracks cardiometabolic trends that may be part of mitochondrial or aging research.
Timing
Follow-up
Marker
CRP
Why it matters
Adds a broad inflammation marker when inflammatory burden is part of the question.
Timing
Optional
Marker
CBC with differential
Why it matters
Screens broad blood-cell patterns that may affect fatigue and general health interpretation.
Timing
Baseline
| Marker | Why it matters | Timing |
|---|---|---|
| Comprehensive metabolic panel (CMP) | Reviews liver, kidney, electrolyte, and glucose context before interpreting energy or metabolic changes. | Baseline |
| A1c | Shows the longer-term blood sugar pattern relevant to metabolic-health research. | Baseline |
| Lipid panel | Tracks cardiometabolic trends that may be part of mitochondrial or aging research. | Follow-up |
| CRP | Adds a broad inflammation marker when inflammatory burden is part of the question. | Optional |
| CBC with differential | Screens broad blood-cell patterns that may affect fatigue and general health interpretation. | Baseline |
Monitoring guidance is pathway-based because Humanin has limited established human monitoring standards.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with diabetes risk, kidney disease, liver disease, inflammatory conditions, or fatigue-focused protocols.
Follow-up
Repeat relevant metabolic and inflammatory markers after 8-12 weeks if the protocol continues.
Longer term
For longer protocols, review trends every 3-6 months with a clinician.
How to interpret the labs
- Routine labs do not directly measure mitochondrial function in a simple way.
- Fatigue, exercise tolerance, sleep, medications, and nutrition should be interpreted with labs.
- Use caution when stacking with other metabolic or mitochondrial agents.
Do not wait for routine labs
Chest pain, fainting, severe weakness, confusion, or rapid worsening fatigue needs medical review.
FAQ
Q1: What is humanin?
Humanin is a small mitochondrial-derived peptide encoded inside mitochondrial DNA, in the 16S rRNA region of the MT-RNR2 gene. It was discovered in 2001 during Alzheimer's research as a factor that protected neurons from amyloid-beta toxicity. The native peptide is 24 amino acids long when translated in the cytoplasm and 21 amino acids when translated in the mitochondria.
Q2: What is HNG?
HNG, sometimes written as humanin-G or S14G-humanin, is a synthetic analog of humanin in which the serine at position 14 is replaced with glycine. That change makes HNG far more stable and significantly more potent than native humanin in published animal studies. Most peer-reviewed dosing protocols, including the 4 mg/kg IP twice-weekly schedule, used HNG rather than native humanin.
Q3: How is humanin commonly dosed in research planning?
The most-cited preclinical protocol used HNG 4 mg/kg intraperitoneal twice weekly in middle-aged mice. Research-use community planning for human use has described subcutaneous milligram-range session doses one to three times weekly over 4 to 12 week cycles. None of these are FDA-approved doses, no human RCT has been published, and this is not a dosing recommendation.
Q4: How is humanin reconstituted?
Humanin and HNG ship as a freeze-dried powder. Most research-use protocols add 2 mL of bacteriostatic water to a 20 mg vial, which gives a 10 mg/mL solution. A 1 mg session dose at that concentration is 0.10 mL, or 10 units on a U-100 insulin syringe. Always match the math to the actual vial size on the supplier label. Use the Peptide Dosing Calculator to verify draw volumes.
Q5: What is the half-life of humanin?
Native humanin has a short circulating half-life of about 30 minutes, which is part of why the more stable HNG analog was developed for research. HNG remains more stable but does not have published human pharmacokinetic data. Specialized stabilization formulations have been developed in research settings to extend HNG stability further.
Q6: What route is humanin given?
Animal studies have most often used intraperitoneal (IP) injection at 4 mg/kg twice weekly. Research-use community planning for human reference protocols typically describes subcutaneous (SC) injection. Some early animal pharmacology has also used intracerebroventricular and intravenous routes for specific endpoints. None of those routes are validated for human use.
Q7: How long is a typical humanin cycle?
Animal protocols have run for months. Research-use community planning typically describes 4 to 12 week cycles with off periods of similar length. There is no human evidence base to define an optimal cycle length, so any cycle structure is research-planning extrapolation rather than evidence.
Q8: What supplies are needed for a humanin protocol?
A typical research-use setup includes the humanin or HNG vial, bacteriostatic water for reconstitution, U-100 insulin syringes (0.3 mL or 0.5 mL), alcohol prep swabs, and a sharps container. The supplies-needed section above shows vial, syringe, BAC water, and swab math by cycle length.
Q9: What are the main side effects of humanin?
Animal studies have not reported significant adverse effects at the doses tested, but those studies were not designed to characterize human safety. Reasonable expectations include mild injection site reactions, occasional fatigue, headache, or transient nausea. The clearest theoretical risk is the anti-apoptotic effect through BAX inactivation, which raises questions about cancer surveillance that have not been resolved.
Q10: Who should avoid humanin?
Anyone with active or recent cancer, anyone pregnant or lactating, children, anyone on insulin or insulin-secretagogues, and anyone with active autoimmune disease should not use humanin without qualified clinical oversight. The detailed list is in the Who Should Avoid section above.
Q11: How does humanin compare to MOTS-c?
Both are peptides encoded inside mitochondrial DNA. Humanin is 24 amino acids and is most studied for cytoprotection, neuroprotection, and cardiac aging models. MOTS-c is 16 amino acids, encoded in the 12S rRNA region, and is most studied for skeletal-muscle metabolism, insulin sensitivity, and exercise biology. They are not interchangeable and target different pathways. See the MOTS-c protocol for the closest peer.
Q12: Is humanin FDA-approved?
No. As of June 2026, humanin and HNG are not approved by the FDA, EMA, or any major regulator for any indication. Research peptides sold under the humanin or HNG name are research-use products and are not approved for human use.
Q13: Is this page medical advice?
No. This page is an educational research reference. Nothing here is a treatment recommendation or a substitute for qualified medical care. Do not start any peptide protocol without supervision from a qualified clinician.
Sources & Research
- 1. Coradduzza D, Congiargiu A, Chen Z, Cruciani S, Zinellu A, Carru C, Medici S Humanin and Its Pathophysiological Roles in Aging: A Systematic Review. Biology (Basel) (2023)
- 2. Yen K, Mehta HH, Kim SJ, Lue Y, Hoang J, Guerrero N, et al. The mitochondrial derived peptide humanin is a regulator of lifespan and healthspan. Aging (Albany NY) (2020)
- 3. Qin Q, Mehta H, Yen K, Navarrete G, Brandhorst S, Wan J, et al. Chronic treatment with the mitochondrial peptide humanin prevents age-related myocardial fibrosis in mice. American Journal of Physiology-Heart and Circulatory Physiology (2018)
- 4. Conte M, Ostan R, Fabbri C, Santoro A, Guidarelli G, Vitale G, et al. Human Aging and Longevity Are Characterized by High Levels of Mitokines. The Journals of Gerontology: Series A (2019)
- 5. Conte M, Martucci M, Mosconi G, Chiariello A, Cappuccilli M, Totti V, et al. Disease-specific plasma levels of mitokines FGF21, GDF15, and Humanin in type II diabetes and Alzheimer's disease in comparison with healthy aging. GeroScience (2020)
- 6. Mehta HH, Xiao J, Ramirez R, Miller B, Kim SJ, Cohen P, Yen K Metabolomic profile of diet-induced obesity mice in response to humanin and small humanin-like peptide 2 treatment. Metabolomics (2019)
- 7. Sharp TE 3rd, Schena GJ, Hobby AR, Starosta T, Berretta RM, Wallner M, et al. Cortical Bone Stem Cell Therapy Preserves Cardiac Structure and Function After Myocardial Infarction (HNG cardioprotection in porcine model context). Circulation Research / related humanin cardioprotection literature (2020)
- 8. Sreekumar PG, Ishikawa K, Spee C, Mehta HH, Wan J, Yen K, et al. The Mitochondrial-Derived Peptide Humanin Protects RPE Cells From Oxidative Stress, Senescence, and Mitochondrial Dysfunction. Investigative Ophthalmology & Visual Science (2016)
- 9. Gong Z, Tas E, Muzumdar R Humanin and age-related diseases: a new therapeutic target? Frontiers in Endocrinology / related reviews (2014-2022)
- 10. Theurey P, Pizzo P (review summaries) / Nashine S et al. Humanin G protects retinal pigment epithelial cybrids from inflammation in age-related macular degeneration models. Aging / Mol Med (2022)
- 11. Gerasimenko M, Lecka-Czernik B, et al. (eds. summary) Neuroprotective Action of Humanin and Humanin Analogues: Research Findings and Perspectives. International Journal of Molecular Sciences (2023)
- 12. U.S. Food and Drug Administration Drug approval databases (Drugs@FDA, Orange Book) confirming no approved humanin or HNG product as of June 2026. FDA.gov (2026)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page