NAD+ Quick Start
NAD+ (nicotinamide adenine dinucleotide) is a coenzyme found in every living cell. Your body uses it to turn food into cellular energy (ATP), to fuel DNA repair, and to power a family of longevity-related enzymes called sirtuins.
This page is a route-by-route research-context protocol. It covers subcutaneous (SubQ) injection, intravenous (IV) infusion, intramuscular (IM) injection, oral NMN, oral NR, intranasal/sublingual formats, and pre-mixed pen or pharmacy liquid options. Pick the tab that matches the format you are researching.
Is NAD+ a peptide?
No. NAD+ is a coenzyme, not a peptide. It is grouped with peptide protocols because it shares the injectable research-use format and overlaps with peptide research goals around energy, recovery, and longevity. Searches for "NAD peptide" usually mean injectable NAD+, not a true peptide compound.
Routes
SubQ, IV, IM, oral (NMN/NR), intranasal/sublingual, and pre-mixed pen/pharmacy liquid.
Schedule
SubQ research planning is typically 2-3x weekly. IV is weekly to monthly. Oral precursors are daily.
Measure
Use vial concentration to convert mg to mL, then to insulin-syringe units.
Supplies
Match vial count, syringe count, BAC water bottles, and swabs to your cycle length.
Status
Injectable NAD+ is not FDA-approved as a therapeutic. Educational reference only.
Disclaimer
This page is an educational research reference and is not medical advice. NAD+ injection is not FDA-approved. Talk with a licensed clinician before making any health decision.
NAD+ Dosing Protocol & Schedule
Choose the tab that matches the route you are researching. Each tab uses research-context planning numbers, not personal medical instructions. Numbers reflect published research, manufacturer/pharmacy ranges, and community-derived planning patterns.
NAD+ Protocol Formats
Switch tabs to see route-specific NAD+ dose ranges, scheduling notes, and evidence boundaries.
Most practical injectable route for research-use planning at home settings.
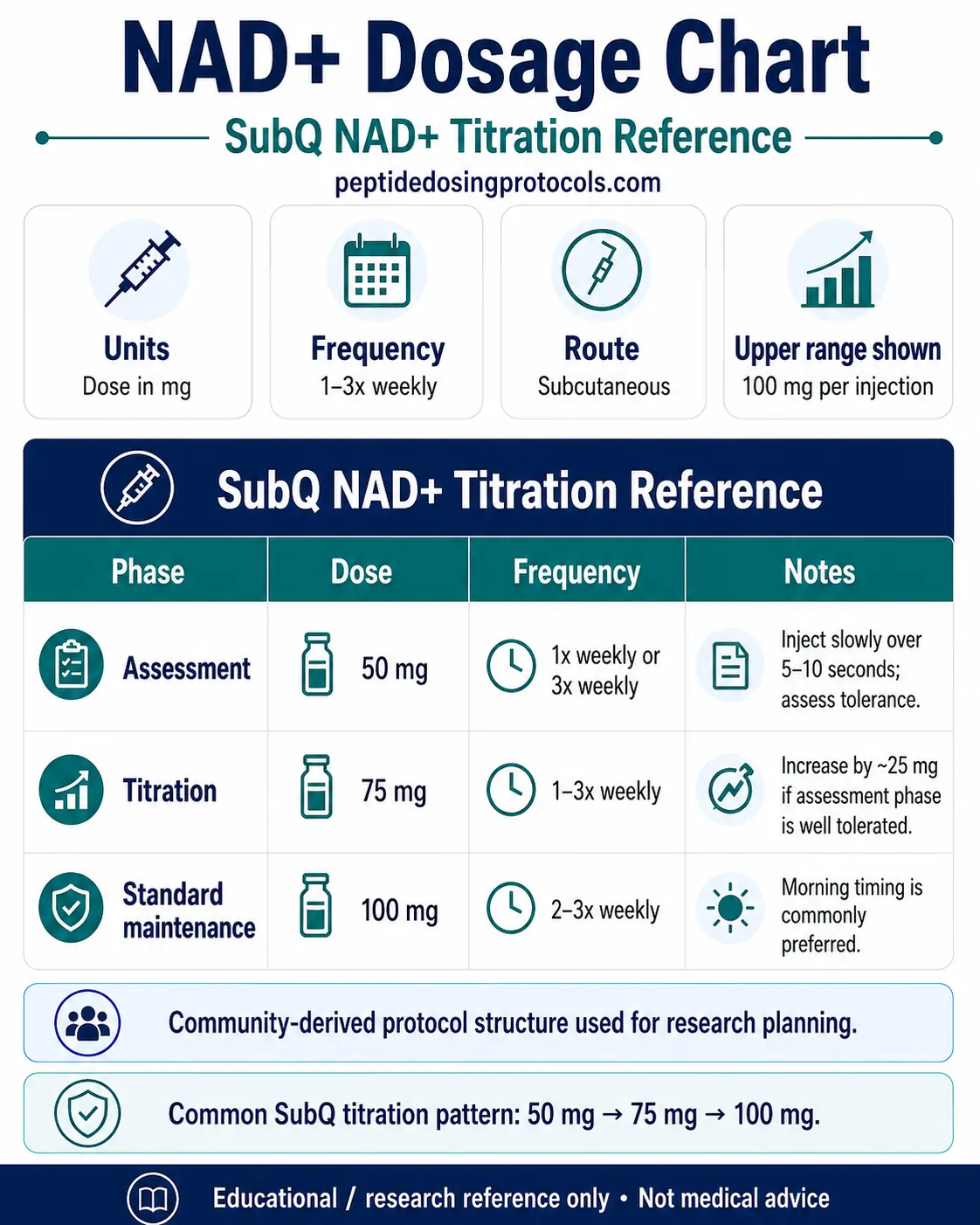
Common research-context range: 50-100 mg per injection, 2-3 times per week. Some titration models start at 50 mg once weekly for 4 weeks, then escalate to 100 mg weekly. Higher daily-loading models (100-200 mg daily for 7-10 days) appear in clinic protocols and are typically reserved for supervised settings.
SubQ NAD+ Titration Reference
Phase
Assessment
Dose
50 mg
Frequency
1x weekly or 3x weekly
Notes
Inject slowly over 5-10 seconds; assess tolerance.
Phase
Titration
Dose
75 mg
Frequency
1-3x weekly
Notes
Increase by ~25 mg if assessment phase is well tolerated.
Phase
Standard maintenance
Dose
100 mg
Frequency
2-3x weekly
Notes
Morning timing is commonly preferred.
Phase
Loading (intensive)
Dose
100-200 mg
Frequency
Daily for 7-10 days
Notes
Higher side-effect potential; supervised settings only.
| Phase | Dose | Frequency | Notes |
|---|---|---|---|
| Assessment | 50 mg | 1x weekly or 3x weekly | Inject slowly over 5-10 seconds; assess tolerance. |
| Titration | 75 mg | 1-3x weekly | Increase by ~25 mg if assessment phase is well tolerated. |
| Standard maintenance | 100 mg | 2-3x weekly | Morning timing is commonly preferred. |
| Loading (intensive) | 100-200 mg | Daily for 7-10 days | Higher side-effect potential; supervised settings only. |
Some research-planning protocols cap weekly SubQ at ~300 mg without further evaluation.
Why slow injection matters: SubQ NAD+ commonly produces brief stinging or burning at the site. Injecting over 5-10 seconds (sometimes longer) usually reduces rate-dependent discomfort. Site rotation across the four abdominal quadrants, the back of the upper arm, and the outer thigh helps prevent nodules and lipohypertrophy.
Highest peak NAD+ levels; typically clinic-administered.
Common research-context range: 250-500 mg per session weekly or bi-weekly; 500-1,000 mg per session in higher-dose clinic protocols. IV NAD+ is delivered slowly over 2-4 hours. Faster infusion rates increase the chance of acute discomfort like flushing, nausea, chest tightness, or headache.
IV NAD+ Reference Ranges
Approach
Maintenance
Per-session dose
250-500 mg
Schedule
Weekly to bi-weekly
Notes
Slow infusion over 2-4 hours.
Approach
Loading
Per-session dose
500-1,000 mg
Schedule
3-5 consecutive days, then weekly/monthly
Notes
Clinic-supervised only.
| Approach | Per-session dose | Schedule | Notes |
|---|---|---|---|
| Maintenance | 250-500 mg | Weekly to bi-weekly | Slow infusion over 2-4 hours. |
| Loading | 500-1,000 mg | 3-5 consecutive days, then weekly/monthly | Clinic-supervised only. |
A 750 mg single 3-hour infusion has been reported to raise blood NAD+ ~398% over baseline in published pilot work.
IV access, pump rate control, and emergency response capacity are typical reasons IV NAD+ is administered in licensed clinic settings rather than home research-use settings.
Faster systemic absorption than SubQ; less common in research planning.
Common research-context range: 50-100 mg per injection, 1-3 times per week. IM injection delivers NAD+ into the gluteal, deltoid, or vastus lateralis muscle. Onset tends to be faster than SubQ because of higher tissue blood flow, but injection-site discomfort can be more pronounced.
Direct head-to-head IM-vs-SubQ NAD+ pharmacokinetic data is limited. Most home research-planning protocols default to SubQ for tolerability, with IM reserved for clinician-led settings.
Daily oral precursor capsules. Strongest published human RCT base.
Oral NAD+ does not survive digestion intact; published research uses precursors that the body converts to NAD+. The two most studied are nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN).
Oral NAD+ Precursor Ranges from Published Trials
Precursor
Nicotinamide Riboside (NR)
Dose
300-1,000 mg
Frequency
Daily
Trial signal
Multiple human RCTs raised blood NAD+ with favorable tolerability.
Precursor
Nicotinamide Mononucleotide (NMN)
Dose
300-900 mg
Frequency
Daily
Trial signal
60-day dose-response RCT showed dose-dependent NAD+ rise; 600 mg gave the largest effect.
| Precursor | Dose | Frequency | Trial signal |
|---|---|---|---|
| Nicotinamide Riboside (NR) | 300-1,000 mg | Daily | Multiple human RCTs raised blood NAD+ with favorable tolerability. |
| Nicotinamide Mononucleotide (NMN) | 300-900 mg | Daily | 60-day dose-response RCT showed dose-dependent NAD+ rise; 600 mg gave the largest effect. |
Oral routes raise blood NAD+ more gradually than injection or IV.
Mucosal absorption formats. Limited published evidence.
Common research-context range: 50-200 mg per dose for intranasal sprays or sublingual troches, dosed daily or several times weekly. Bioavailability is route-dependent and lower than injection or IV. Direct head-to-head pharmacokinetic data versus SubQ NAD+ is limited.
These formats are usually pharmacy-prepared. Confirm pharmacy beyond-use dating and storage instructions before relying on a specific schedule.
Pharmacy-prepared liquid vials or pen devices that skip reconstitution.
Pre-mixed liquid NAD+ is supplied as a sterile, pharmacy-compounded solution at a fixed concentration (commonly 100 mg/mL or 200 mg/mL). Pen devices use the same liquid in a multi-dose cartridge with a click-set delivery volume.
Pen / Pre-mixed Reference
Format
Pre-mixed vial
Concentration
100 mg/mL
Dose example
50 mg
Volume per dose
0.50 mL (50 units)
Format
Pre-mixed vial
Concentration
100 mg/mL
Dose example
100 mg
Volume per dose
1.00 mL (100 units)
Format
Pre-mixed vial (high-conc.)
Concentration
200 mg/mL
Dose example
100 mg
Volume per dose
0.50 mL (50 units)
Format
Pen device
Concentration
Set per device
Dose example
Click-set per dose
Volume per dose
Per device label
| Format | Concentration | Dose example | Volume per dose |
|---|---|---|---|
| Pre-mixed vial | 100 mg/mL | 50 mg | 0.50 mL (50 units) |
| Pre-mixed vial | 100 mg/mL | 100 mg | 1.00 mL (100 units) |
| Pre-mixed vial (high-conc.) | 200 mg/mL | 100 mg | 0.50 mL (50 units) |
| Pen device | Set per device | Click-set per dose | Per device label |
Always verify label concentration and pharmacy beyond-use dating.
Cycle Guidelines
Common NAD+ Cycle Reference
Approach
Standard SubQ
Duration
4-8 weeks
Review point
Week 4
Best for
General research-context cellular-energy planning
Approach
Extended SubQ + oral bridge
Duration
8-12 weeks SubQ, then 4 weeks oral NMN/NR
Review point
End of injectable phase
Best for
Layered approach combining injection and oral precursors
Approach
IV maintenance
Duration
Weekly or bi-weekly, ongoing
Review point
Every 4-8 weeks
Best for
Clinic-supervised research planning
Approach
IV loading + maintenance
Duration
3-5 daily IV sessions, then weekly/monthly
Review point
After loading phase
Best for
Intensive clinic protocol
| Approach | Duration | Review point | Best for |
|---|---|---|---|
| Standard SubQ | 4-8 weeks | Week 4 | General research-context cellular-energy planning |
| Extended SubQ + oral bridge | 8-12 weeks SubQ, then 4 weeks oral NMN/NR | End of injectable phase | Layered approach combining injection and oral precursors |
| IV maintenance | Weekly or bi-weekly, ongoing | Every 4-8 weeks | Clinic-supervised research planning |
| IV loading + maintenance | 3-5 daily IV sessions, then weekly/monthly | After loading phase | Intensive clinic protocol |
Unlike receptor-based peptides, NAD+ is a coenzyme. Strict on/off cycling is less established. Many planning models adjust frequency rather than enforce wash-out periods.
Calculator
For exact mg-to-mL-to-insulin-unit conversions across vial sizes, use the NAD+ peptide calculator.
NAD+ Supplies Needed
Plan supplies based on a 100 mg SubQ dose 3x weekly using a 750 mg vial reconstituted with 7.5 mL BAC water (100 mg/mL). Adjust if you research a different vial size, dose, or route.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

NAD+ Buffered

Compounded NAD+

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials (750 mg, 100 mg dose 3x/week)
Each 750 mg vial gives ~7.5 doses of 100 mg. Adjust for a 1,500 mg kit (~15 doses) or 50 mg dose (~15 doses per 750 mg vial).
| Cycle length | Planning note |
|---|---|
4 weeks 2 vials | 12 injections needed; round up for priming losses. |
8 weeks 4 vials | 24 injections needed. |
12 weeks 5 vials | 36 injections needed. |
4 weeks
2 vials
12 injections needed; round up for priming losses.
8 weeks
4 vials
24 injections needed.
12 weeks
5 vials
36 injections needed.
Insulin Syringes (U-100)
Use one fresh syringe per injection. 0.5 mL barrels are easier to read for sub-100-unit draws.
| Cycle length | Planning note |
|---|---|
4 weeks 12 syringes | 1 per injection at 3x/week. |
8 weeks 24 syringes | Bulk box of 100 lasts multiple cycles. |
12 weeks 36 syringes | Confirm gauge and barrel size match draw volume. |
4 weeks
12 syringes
1 per injection at 3x/week.
8 weeks
24 syringes
Bulk box of 100 lasts multiple cycles.
12 weeks
36 syringes
Confirm gauge and barrel size match draw volume.
Bacteriostatic Water
Use 7.5 mL per 750 mg vial for 100 mg/mL. A 10 mL BAC water bottle reconstitutes one 750 mg vial with margin.
| Cycle length | Planning note |
|---|---|
4 weeks 2 x 10 mL bottles | Reconstitutes ~2 vials with margin. |
8 weeks 4 x 10 mL bottles | Adds margin for losses and spare reconstitution. |
12 weeks 5-6 x 10 mL bottles | Round up for any spilled or expired BAC water. |
4 weeks
2 x 10 mL bottles
Reconstitutes ~2 vials with margin.
8 weeks
4 x 10 mL bottles
Adds margin for losses and spare reconstitution.
12 weeks
5-6 x 10 mL bottles
Round up for any spilled or expired BAC water.
Round up everything for dropped syringes, damaged swabs, priming losses, and protocol adjustments.
Companion Supplies & Routine Support
NAD+ Reconstitution Guide
Reconstitution converts a lyophilized (powder) NAD+ vial into a measured liquid concentration. Pre-mixed liquid vials and pens skip this step entirely.
NAD+ Reconstitution by Vial Size
Vial size
750 mg
BAC water added
7.5 mL
Final concentration
100 mg/mL
Volume per 50 mg
0.50 mL (50 units)
Volume per 100 mg
1.00 mL (100 units)
Vial size
750 mg
BAC water added
4.5 mL
Final concentration
166.7 mg/mL
Volume per 50 mg
0.30 mL (30 units)
Volume per 100 mg
0.60 mL (60 units)
Vial size
1,000 mg
BAC water added
10.0 mL
Final concentration
100 mg/mL
Volume per 50 mg
0.50 mL (50 units)
Volume per 100 mg
1.00 mL (100 units)
Vial size
1,000 mg
BAC water added
5.0 mL
Final concentration
200 mg/mL
Volume per 50 mg
0.25 mL (25 units)
Volume per 100 mg
0.50 mL (50 units)
Vial size
1,500 mg
BAC water added
10.0 mL
Final concentration
150 mg/mL
Volume per 50 mg
0.33 mL (33 units)
Volume per 100 mg
0.67 mL (67 units)
| Vial size | BAC water added | Final concentration | Volume per 50 mg | Volume per 100 mg |
|---|---|---|---|---|
| 750 mg | 7.5 mL | 100 mg/mL | 0.50 mL (50 units) | 1.00 mL (100 units) |
| 750 mg | 4.5 mL | 166.7 mg/mL | 0.30 mL (30 units) | 0.60 mL (60 units) |
| 1,000 mg | 10.0 mL | 100 mg/mL | 0.50 mL (50 units) | 1.00 mL (100 units) |
| 1,000 mg | 5.0 mL | 200 mg/mL | 0.25 mL (25 units) | 0.50 mL (50 units) |
| 1,500 mg | 10.0 mL | 150 mg/mL | 0.33 mL (33 units) | 0.67 mL (67 units) |
Higher-concentration mixes reduce injection volume but require finer measurement on the syringe.
Step-by-Step Reconstitution
- 01
Bring vial to room temperature
Let the lyophilized NAD+ vial sit at room temperature for 5-10 minutes before reconstitution.
- 02
Clean the stoppers
Wipe the NAD+ vial stopper and the BAC water stopper with separate sterile alcohol swabs.
- 03
Draw the BAC water
Use a sterile syringe to draw the planned BAC water volume from the bottle.
- 04
Inject down the vial wall
Aim the BAC water stream down the inside wall of the NAD+ vial, not directly onto the powder. This reduces foaming.
- 05
Swirl gently
Roll or swirl the vial slowly until the powder fully dissolves. Do not shake aggressively.
- 06
Inspect the solution
Confirm the liquid is clear and free of particulates. Discard if it looks discolored or cloudy.
- 07
Label and refrigerate
Mark the vial with the concentration and reconstitution date. Store at 2-8C and use within manufacturer or pharmacy beyond-use guidance.
Calculator
Use the NAD+ peptide calculator for exact syringe units across any vial size and BAC water volume.
NAD+ Dosage Chart
This NAD+ dosage chart summarizes a common SubQ titration reference from 50 mg to 100 mg per injection, with frequency and tolerance notes shown by phase.
How NAD+ Works
NAD+ moves electrons between chemical reactions inside cells. That role makes it a critical part of how mitochondria turn food into ATP, how cells repair DNA, and how a family of regulatory proteins called sirtuins control gene activity.
Energy production
Mitochondria use NAD+ to shuttle electrons through the electron transport chain. When NAD+ levels drop, ATP production becomes less efficient.
DNA repair (PARPs)
PARP enzymes consume NAD+ to repair damaged DNA strands. Chronic DNA damage burns through NAD+ over time, which can compete with energy-production needs.
Sirtuin activation
Sirtuins (SIRT1-7) are NAD+-dependent enzymes that regulate gene expression, mitochondrial biogenesis, inflammation, and stress responses. Sirtuin activity falls when NAD+ falls.
CD38 and inflammaging
CD38, a NAD+-consuming enzyme, becomes more active with age and chronic inflammation. Higher CD38 activity contributes to age-related NAD+ decline.
Tissue NAD+ levels fall progressively across the lifespan. Restoring NAD+ levels in animal models has reversed multiple aging biomarkers; in human research, oral precursors raise blood NAD+ reliably, while injectable NAD+ pharmacokinetics are less fully characterized.
Who NAD+ Is For and Who Should Avoid It
Research-context interest in NAD+ centers on cellular-energy support, recovery research, and longevity research planning. Several groups should not pursue NAD+ injection without licensed clinician oversight.
- Pregnancy and breastfeeding — insufficient safety data.
- Active malignancy — NAD+ supports cellular proliferation, including potentially in cancer cells; oncologist consultation is essential.
- Severe hepatic or renal impairment — high-dose protocols may add metabolic burden.
- Known hypersensitivity to NAD+ formulation components or BAC water preservatives.
- Concurrent high-dose niacin — overlapping NAD+ pathway loads warrant clinician review.
- People on glucose-lowering medications — NAD+ may enhance insulin sensitivity over time; closer glucose monitoring is prudent.
Not medical advice
Eligibility judgments require a licensed clinician who knows your medical history. This list highlights commonly-cited boundaries from the published literature, not a personalized screen.
NAD+ Side Effects & Safety
Commonly reported with SubQ
- Injection-site stinging, burning, redness, or temporary nodules — managed with slow injection and site rotation.
- Nausea, headache, or flushing during early titration — often dose- and rate-dependent.
- Temporary fatigue or paradoxical tiredness in the first few sessions.
- Sleep disruption when injected later in the day.
Commonly reported with IV
- Flushing and warmth, especially with faster infusion rates.
- Chest tightness or shortness of breath at faster infusion rates.
- Mild headache from transient vasodilation.
- Transient increase in heart rate with rapid administration.
Theoretical or longer-horizon concerns
- Long-term human safety data for high-dose injectable NAD+ remains limited.
- Active malignancy is a contraindication because NAD+ supports cellular proliferation.
- Liver and kidney markers are reasonable to track in extended high-dose protocols.
Most acute side effects are dose-dependent and rate-dependent. Slower injection, lower starting doses, and morning timing all reduce reported tolerability issues.
NAD+ Timeline & What to Monitor
What changes when
- Immediate (24-48 hours) — IV NAD+ recipients commonly report energy and mental-clarity changes; SubQ effects may take longer.
- Weeks 1-4 — energy and sleep changes are the most commonly reported subjective endpoints during titration.
- Weeks 4-12 — recovery, exercise capacity, and skin-quality reports emerge anecdotally; large RCT outcome data is lacking for direct injection.
- Beyond 12 weeks — sustained planning typically rotates between SubQ phases and oral precursor bridges.
What is reasonable to monitor
- Sleep quality and timing (NAD+ can feel stimulating if dosed late).
- Subjective energy and recovery from training.
- Liver markers (ALT, AST) in extended high-dose protocols.
- Glucose markers if also using glucose-lowering medications.
- Injection-site appearance — rotation and slow injection should keep sites clean.
Stopping points
If side effects do not resolve with slower injection or dose reduction, the most common research-planning response is to pause, reassess, and consult a clinician before resuming.
NAD+ Clinical Evidence Context
Most published human RCT evidence on NAD+ uses oral precursors (NR and NMN), not direct injectable NAD+. The summary below separates the two.
Oral NR (strongest human RCT base)
Multiple RCTs (Martens 2018, Conze 2019, Dollerup 2018, Brakedal 2022) consistently raised blood NAD+ with favorable tolerability at doses up to 1,000 mg/day.
Oral NMN (growing human RCT base)
Yoshino 2021 showed improved muscle insulin sensitivity at 250 mg/day in postmenopausal women. A 2022 dose-response RCT (Yi et al., Geroscience) at 300/600/900 mg/day raised NAD+ dose-dependently with no safety issues at 60 days.
Direct injectable NAD+ (limited human evidence)
Historical IV case reports (O'Holleran 1961) plus pilot pharmacokinetic comparisons (e.g. ChromaDex 2024 medRxiv) show IV delivery raises NAD+ rapidly. A 2024 systematic review in the American Journal of Physiology found insufficient high-quality evidence for routine subcutaneous NAD+ practice.
Mechanism and biology
Yoshino, Baur, Imai 2018 (Cell Metabolism) and Covarrubias et al. 2021 (Nature Reviews Mol Cell Biol) document age-related NAD+ decline and the biology that drives clinical interest.
Ongoing trials
Trials like NCT07328100 (intravenous coenzyme I for vascular aging, 2026 start) and NCT05243290 (oral NR in Gulf War Illness) continue to expand the human evidence base.
Evidence gap
Large-scale, long-duration RCTs of subcutaneous NAD+ for wellness or longevity endpoints have not been published as of June 2026.
NAD+ Storage & Handling
NAD+ Storage Reference
State
Lyophilized (powder)
Storage
68-77F (20-25C) room temp, dry, dark
Notes
Acceptable for short-term per manufacturer label.
State
Lyophilized (powder)
Storage
35.6-46.4F (2-8C) refrigerated
Notes
Long-term storage option; follow manufacturer guidance.
State
Pre-mixed liquid
Storage
35.6-46.4F (2-8C)
Notes
Use per pharmacy beyond-use date.
State
Reconstituted (from powder)
Storage
35.6-46.4F (2-8C)
Notes
Typical 14-30 day window depending on compounder guidance.
| State | Storage | Notes |
|---|---|---|
| Lyophilized (powder) | 68-77F (20-25C) room temp, dry, dark | Acceptable for short-term per manufacturer label. |
| Lyophilized (powder) | 35.6-46.4F (2-8C) refrigerated | Long-term storage option; follow manufacturer guidance. |
| Pre-mixed liquid | 35.6-46.4F (2-8C) | Use per pharmacy beyond-use date. |
| Reconstituted (from powder) | 35.6-46.4F (2-8C) | Typical 14-30 day window depending on compounder guidance. |
Avoid freezing lyophilized NAD+ unless the manufacturer label allows it. Discard reconstituted solution if it yellows, browns, or shows particulates.
NAD+ Protocol Mistakes & Troubleshooting
- 01
Strong injection-site sting
Inject more slowly (10-15 seconds), reduce per-injection dose, switch to a lower-concentration mix, and rotate sites.
- 02
Cloudy or discolored vial
Discard the vial and reconstitute a fresh one. Cloudy or yellowing solution should not be injected.
- 03
Wrong BAC water volume
Recalculate concentration with the actual volume added; use the calculator to refit dose volume to the new concentration.
- 04
Flushing or chest tightness during IV
Slow the infusion rate. Faster IV NAD+ rates are the most commonly reported driver of acute side effects.
- 05
Sleep disruption
Move the dose to morning and avoid late-day injections. NAD+ can feel stimulating through energy-pathway activation.
- 06
Missed dose
Skip the missed dose and resume at the next scheduled session. Do not double-dose.
- 07
Site nodule or irritation
Rotate to a fresh quadrant for several sessions, inspect the syringe-and-needle technique, and slow the injection. Persistent reactions warrant clinician review.
Seek qualified care
If symptoms include severe shortness of breath, chest pain, or signs of an allergic reaction, stop immediately and seek qualified medical care.
NAD+ Regulatory Status
As of June 2026: Injectable NAD+ is not FDA-approved for any therapeutic indication in the United States. It is available only as a compounded preparation through 503A/503B pharmacies under valid prescription.
Oral precursors have a different regulatory profile. Nicotinamide riboside (NR) holds GRAS and NDI status as a dietary supplement ingredient. Nicotinamide mononucleotide (NMN) was excluded from the dietary supplement definition by FDA in 2022-2023 and remains in regulatory limbo for new dietary supplement marketing in the US.
Internationally, IV NAD+ is offered through licensed clinics in many jurisdictions; rules on compounded injectable products vary. Verify your local regulations and pharmacy licensing before any sourcing decision.
NAD+ vs NMN vs NR (and IV vs SubQ)
NAD+ Delivery Comparison
Feature
Mechanism
NAD+ Injection (SubQ)
Direct coenzyme delivery
NAD+ Infusion (IV)
Direct coenzyme delivery
Oral NMN
NAD+ precursor (converted in vivo)
Oral NR (Niagen)
NAD+ precursor (converted in vivo)
Feature
Typical research-planning dose
NAD+ Injection (SubQ)
50-100 mg, 2-3x/week
NAD+ Infusion (IV)
250-1,000 mg per session
Oral NMN
300-600 mg/day
Oral NR (Niagen)
300-1,000 mg/day
Feature
Speed to systemic NAD+ rise
NAD+ Injection (SubQ)
Hours
NAD+ Infusion (IV)
Minutes to hours
Oral NMN
Days to weeks
Oral NR (Niagen)
Days to weeks
Feature
Strongest human evidence
NAD+ Injection (SubQ)
Limited
NAD+ Infusion (IV)
Pilot PK and historical case reports
Oral NMN
Growing RCT base
Oral NR (Niagen)
Strongest RCT base
Feature
Convenience
NAD+ Injection (SubQ)
At-home injection technique required
NAD+ Infusion (IV)
Clinic visit, 2-4 hour infusion
Oral NMN
Daily oral capsule
Oral NR (Niagen)
Daily oral capsule
Feature
Regulatory status
NAD+ Injection (SubQ)
Not FDA-approved; compounded only
NAD+ Infusion (IV)
Not FDA-approved; compounded only
Oral NMN
Not currently a dietary supplement in the US
Oral NR (Niagen)
GRAS/NDI dietary supplement
Feature
Cost (research-context)
NAD+ Injection (SubQ)
Moderate per cycle
NAD+ Infusion (IV)
High per session
Oral NMN
Moderate monthly
Oral NR (Niagen)
Moderate monthly
| Feature | NAD+ Injection (SubQ) | NAD+ Infusion (IV) | Oral NMN | Oral NR (Niagen) |
|---|---|---|---|---|
| Mechanism | Direct coenzyme delivery | Direct coenzyme delivery | NAD+ precursor (converted in vivo) | NAD+ precursor (converted in vivo) |
| Typical research-planning dose | 50-100 mg, 2-3x/week | 250-1,000 mg per session | 300-600 mg/day | 300-1,000 mg/day |
| Speed to systemic NAD+ rise | Hours | Minutes to hours | Days to weeks | Days to weeks |
| Strongest human evidence | Limited | Pilot PK and historical case reports | Growing RCT base | Strongest RCT base |
| Convenience | At-home injection technique required | Clinic visit, 2-4 hour infusion | Daily oral capsule | Daily oral capsule |
| Regulatory status | Not FDA-approved; compounded only | Not FDA-approved; compounded only | Not currently a dietary supplement in the US | GRAS/NDI dietary supplement |
| Cost (research-context) | Moderate per cycle | High per session | Moderate monthly | Moderate monthly |
NMN and NR are oral precursors; SubQ and IV are direct delivery. Research-context plans sometimes layer one oral precursor with periodic injectable phases.
Many planning models pair an oral precursor for daily baseline support with periodic injectable NAD+ phases. The choice usually depends on tolerance, convenience, regulatory access, and cost — not a clear human-efficacy ranking.
NAD+ Blood Tests & Monitoring
NAD+ protocols are usually discussed in energy, aging, and mitochondrial research. Monitoring focuses on broad health context because routine labs do not directly measure meaningful NAD pathway response.
Blood test markers to discuss with a clinician
Marker
CBC with differential
Why it matters
Screens anemia, infection patterns, and general blood-cell context before interpreting fatigue changes.
Timing
Baseline
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews liver, kidney, electrolyte, and glucose context before interpreting energy changes.
Timing
Baseline
Marker
Vitamin B12 and methylmalonic acid
Why it matters
Helps evaluate B12 status when fatigue, neuropathy, or heavy B-vitamin use is part of the context.
Timing
Optional
Marker
Homocysteine
Why it matters
Adds methylation and cardiovascular context when B-vitamin status is being reviewed.
Timing
Optional
Marker
TSH and free T4
Why it matters
Thyroid imbalance can affect fatigue, weight, mood, and energy.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| CBC with differential | Screens anemia, infection patterns, and general blood-cell context before interpreting fatigue changes. | Baseline |
| Comprehensive metabolic panel (CMP) | Reviews liver, kidney, electrolyte, and glucose context before interpreting energy changes. | Baseline |
| Vitamin B12 and methylmalonic acid | Helps evaluate B12 status when fatigue, neuropathy, or heavy B-vitamin use is part of the context. | Optional |
| Homocysteine | Adds methylation and cardiovascular context when B-vitamin status is being reviewed. | Optional |
| TSH and free T4 | Thyroid imbalance can affect fatigue, weight, mood, and energy. | Optional |
Monitoring guidance is pathway-based and broad because NAD+ protocols do not have established clinical lab-response markers.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline labs before starting, especially with fatigue, liver disease, kidney disease, cardiovascular symptoms, or B-vitamin supplementation.
Follow-up
Repeat broad markers after 8-12 weeks if symptoms change or the protocol continues.
Longer term
For longer protocols, review broad health trends every 3-6 months with a clinician.
How to interpret the labs
- Routine bloodwork does not confirm cellular NAD improvement.
- Fatigue can come from sleep, thyroid status, anemia, mood, medications, nutrition, or chronic disease.
- Supplement stacks can complicate interpretation of B-vitamin and methylation markers.
Do not wait for routine labs
Chest pain, fainting, severe shortness of breath, confusion, or new neurologic symptoms need medical review.
FAQ
Q1: Is NAD+ a peptide?
No. NAD+ is a coenzyme, not a peptide. It is grouped with peptide protocols because it shares the injectable research-use format and overlaps with peptide goals around energy, recovery, and longevity. The phrase "NAD peptide" usually refers to injectable NAD+ rather than a true peptide compound.
Q2: What is a typical starting dose of NAD+ injections?
A common research-planning SubQ start is 50 mg (about 0.50 mL at 100 mg/mL) once weekly or three times weekly, then escalate by ~25 mg as tolerated. Use the PepPal calculator for exact syringe units.
Q3: How do you reconstitute a 750 mg NAD+ vial?
The most common mix is 7.5 mL of bacteriostatic water for a 750 mg vial, giving 100 mg/mL. A higher-concentration option is 4.5 mL of BAC water for 166.7 mg/mL. The calculator handles custom volumes.
Q4: How do you reconstitute a 1,000 mg NAD+ vial?
Add 10 mL of bacteriostatic water for a 100 mg/mL solution. Some research-planning protocols use 5 mL of BAC water for a 200 mg/mL high-concentration option, which reduces injection volume but requires more careful syringe measurement.
Q5: How much NAD+ should you take daily?
There is no universal daily dose. Research-planning SubQ models commonly stay at 50-100 mg per injection 2-3x weekly. Loading models use 100-200 mg daily for 7-10 days under supervision. Daily SubQ NAD+ outside loading periods is not standard.
Q6: What is the maximum dose of NAD+ studied?
Historical IV protocols used 500-1,000 mg per session. Common research-planning SubQ caps sit around ~300 mg weekly without further evaluation. Doses above 200-300 mg/day are typically reserved for supervised therapeutic use.
Q7: What are NAD+ injection side effects?
Common reports include injection-site stinging, nausea, headache, flushing, and short-term fatigue. Most acute effects are dose- and rate-dependent and improve with slower injection and conservative titration.
Q8: Is NAD+ FDA-approved?
Injectable NAD+ is not FDA-approved as a therapeutic. It is available only as a compounded preparation through 503A/503B pharmacies. Oral nicotinamide riboside (NR) holds GRAS/NDI status as a dietary supplement.
Q9: Is there a difference between buffered and unbuffered NAD+?
Both contain the same NAD+ molecule. Buffered NAD+ ships with a pH stabilizer (most commonly Tris) that brings the reconstituted solution closer to physiological pH (~7-8.5), while unbuffered NAD+ reconstitutes acidic (~pH 3-4) and is more often associated with injection-site stinging. The dosing math is identical for both formats. For a full buyer-side comparison, see the NAD+ buffered vs unbuffered guide.
Q10: How does NAD+ compare to NMN and NR?
NAD+ injection delivers the molecule directly. NMN and NR are oral precursors the body converts into NAD+. Oral NR has the strongest human RCT base; NMN evidence is growing. Direct injectable NAD+ has more limited human RCT data but rapid systemic availability.
Q11: How long does NAD+ take to work?
IV NAD+ commonly produces noticeable acute effects within 24-48 hours. SubQ NAD+ effects are usually more gradual over the first 2-4 weeks of consistent dosing. Larger RCT outcome data for direct injectable NAD+ remains limited.
Q12: Can NAD+ be taken on an empty stomach SubQ?
SubQ NAD+ does not depend on stomach contents because it bypasses digestion. Some researchers prefer morning dosing on an empty stomach for energy-pathway timing, but this is preference-driven rather than evidence-driven.
Q13: Where can I buy NAD+ research peptides?
Peptide Dosing Protocols does not directly sell NAD+. Compare COA-verified suppliers in the PepPal supplier directory and verify current vial size, concentration, and lab testing before any sourcing decision.
Q14: Is this NAD+ guide medical advice?
No. This page is an educational research reference. NAD+ injection is not FDA-approved. Consult a licensed clinician for personal medical decisions.
Sources & Research
- 1. Martens CR, Denman BA, Mazzo MR, et al. Chronic nicotinamide riboside supplementation is well-tolerated and elevates NAD+ in healthy middle-aged and older adults. Nature Communications (2018)
- 2. Conze D, Brenner C, Kruger CL. Safety and Metabolism of Long-term Administration of NIAGEN in Healthy Overweight Adults. Scientific Reports (2019)
- 3. Yoshino M, Yoshino J, Kayser BD, et al. Nicotinamide mononucleotide increases muscle insulin sensitivity in prediabetic women. Science (2021)
- 4. Yi L, Maier AB, Tao R, et al. The efficacy and safety of beta-nicotinamide mononucleotide (NMN) supplementation in healthy middle-aged adults: a randomized, multicenter, double-blind, placebo-controlled, parallel-group, dose-dependent clinical trial. GeroScience (2023)
- 5. Brakedal B, Dolle C, Riber F, et al. The NADPARK study: A randomized phase I trial of nicotinamide riboside supplementation in Parkinson's disease. Cell Metabolism (2022)
- 6. Dollerup OL, Christensen B, Svart M, et al. A randomized placebo-controlled clinical trial of nicotinamide riboside in obese men. American Journal of Clinical Nutrition (2018)
- 7. Elhassan YS, Kluckova K, Fletcher RS, et al. Nicotinamide Riboside Augments the Aged Human Skeletal Muscle NAD+ Metabolome and Induces Transcriptomic and Anti-inflammatory Signatures. Cell Reports (2019)
- 8. Yoshino J, Baur JA, Imai SI. NAD+ Intermediates: The Biology and Therapeutic Potential of NMN and NR. Cell Metabolism (2018)
- 9. Covarrubias AJ, Perrone R, Grozio A, Verdin E. NAD+ metabolism and its roles in cellular processes during ageing. Nature Reviews Molecular Cell Biology (2021)
- 10. Trammell SAJ, Schmidt MS, Weidemann BJ, et al. Nicotinamide riboside is uniquely and orally bioavailable in mice and humans. Nature Communications (2016)
- 11. Braidy N, Liu Y. NAD+ therapy in age-related degenerative disorders: A benefit/risk analysis. Experimental Gerontology (2020)
- 12. Hong W, Mo F, Zhang Z, et al. The Safety and Antiaging Effects of Nicotinamide Mononucleotide in Human Clinical Trials: an Update. Advances in Nutrition (2023)
- 13. Evaluation of safety and effectiveness of NAD in different clinical conditions (systematic review). Evaluation of safety and effectiveness of NAD in different clinical conditions: a systematic review. American Journal of Physiology - Endocrinology and Metabolism (2024)
- 14. ClinicalTrials.gov NCT07328100 — Efficacy and Safety of Coenzyme I (NAD) for Injection on Vascular Aging. ClinicalTrials.gov (2026)
- 15. Cleveland Clinic Health Library NAD (Nicotinamide Adenine Dinucleotide) — function, anatomy, conditions and disorders. Cleveland Clinic (2026)
Related Dosing Protocols
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: July 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page