ARA-290 Quick Start
ARA-290, also called cibinetide, is a small 11-amino-acid peptide built from one piece of the erythropoietin (EPO) molecule. It was engineered to keep EPO's tissue-repair and anti-inflammatory signaling while removing the part that makes red blood cells. In research it is given as a subcutaneous injection from a reconstituted vial.
ARA-290 has more human trial data than many research peptides, especially for sarcoidosis- and diabetes-related nerve symptoms. Development later stalled after Phase 2, with no Phase 3 trial or approval.
What it is
An EPO-derived, non-erythropoietic innate-repair-receptor agonist.
Route
Subcutaneous injection; early trials also used IV.
Trial doses
1-8 mg daily subQ in Phase 2; 4 mg was central.
Research status
Not FDA-approved; orphan/fast-track only; development stalled.
Educational research reference only
This page summarizes how ARA-290 was dosed in research and is discussed in the research community. It is not medical advice, a prescription, or a treatment plan. ARA-290 is not FDA-approved for human use. Talk to a qualified clinician before using any peptide.
ARA-290 Dosing Protocol & Schedule
ARA-290 dosing is easier to anchor than many peptides because published trials and common research-community protocols use similar ranges. Human studies used daily subcutaneous injections from 1-8 mg, with 4 mg/day appearing most often.
Doses used in ARA-290 human trials
Study context
Sarcoidosis pilot (2012)
Dose & route
2 mg IV
Schedule
3x/week, 4 weeks
Study context
Sarcoidosis SFN (2013)
Dose & route
Daily subQ
Schedule
28 days
Study context
Type 2 diabetes neuropathy (2014)
Dose & route
4 mg subQ
Schedule
Daily, 28 days
Study context
Phase 2b sarcoidosis (2017)
Dose & route
1, 4, or 8 mg subQ
Schedule
Daily, 28 days
Study context
Diabetic macular edema (2020)
Dose & route
4 mg subQ
Schedule
Daily, 12 weeks
| Study context | Dose & route | Schedule |
|---|---|---|
| Sarcoidosis pilot (2012) | 2 mg IV | 3x/week, 4 weeks |
| Sarcoidosis SFN (2013) | Daily subQ | 28 days |
| Type 2 diabetes neuropathy (2014) | 4 mg subQ | Daily, 28 days |
| Phase 2b sarcoidosis (2017) | 1, 4, or 8 mg subQ | Daily, 28 days |
| Diabetic macular edema (2020) | 4 mg subQ | Daily, 12 weeks |
This is trial reporting, not a dosing recommendation. Most later trials used daily subcutaneous injection; the earliest used IV.
Community-derived subQ structure
Item
Typical range
Commonly reported
1-4 mg/day
Item
Higher range cited
Commonly reported
Up to 8 mg/day (trial ceiling)
Item
Frequency
Commonly reported
Once daily
Item
Cycle length
Commonly reported
About 4 weeks, matching trial blocks
Item
Route
Commonly reported
Subcutaneous injection
| Item | Commonly reported |
|---|---|
| Typical range | 1-4 mg/day |
| Higher range cited | Up to 8 mg/day (trial ceiling) |
| Frequency | Once daily |
| Cycle length | About 4 weeks, matching trial blocks |
| Route | Subcutaneous injection |
Community figures mirror the trial doses. Because trials ran for 28 days, longer-term safety at these doses is not established.
Where it is injected
In trials and community use, ARA-290 is given subcutaneously, typically into the fat of the lower abdomen or thigh with a small insulin syringe. Rotate sites to reduce local irritation.
ARA-290 Supplies Needed
These supply estimates use a 16 mg vial mixed with 2 mL BAC water, giving 8 mg/mL. At 4 mg/day, each vial provides about 4 doses. Lower doses stretch each vial further, but only mix what you can use within about 14 days.
Recommended USA Supply
SAVE10 applies to eligible Peptira checkout links when supported by the supplier.
ARA-290 Supply

SiPhox Health At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials
Based on a 16 mg vial and a representative 4 mg daily dose, one vial gives about 4 doses.
| Cycle length | Planning note |
|---|---|
2 weeks 4 vials | 14 doses needed at 4 mg/day |
4 weeks 7 vials | 28 doses needed at 4 mg/day |
6 weeks 11 vials | 42 doses needed at 4 mg/day |
8 weeks 14 vials | 56 doses needed at 4 mg/day |
2 weeks
4 vials
14 doses needed at 4 mg/day
4 weeks
7 vials
28 doses needed at 4 mg/day
6 weeks
11 vials
42 doses needed at 4 mg/day
8 weeks
14 vials
56 doses needed at 4 mg/day
Insulin Syringes (U-100)
One syringe per daily injection. A 0.5 mL / 50-unit syringe fits a 4 mg draw at 8 mg/mL.
| Cycle length | Planning note |
|---|---|
2 weeks 14 syringes | 1 per day |
4 weeks 28 syringes | 1 per day |
2 weeks
14 syringes
1 per day
4 weeks
28 syringes
1 per day
Bacteriostatic Water
Use 2 mL per 16 mg vial for reconstitution.
| Cycle length | Planning note |
|---|---|
2 weeks 1 x 10 mL bottle | 4 vials use 8 mL |
4 weeks 2 x 10 mL bottles | 7 vials use 14 mL |
2 weeks
1 x 10 mL bottle
4 vials use 8 mL
4 weeks
2 x 10 mL bottles
7 vials use 14 mL
Vial counts shown are for 4 mg/day; at 1-2 mg/day you need far fewer. Round up for priming losses and dropped syringes, and do not mix more than you can use within about 14 days.
Companion Supplies & Routine Support
ARA-290 Reconstitution Guide
Reconstitution turns the dry powder into a measurable liquid. Concentration is vial size divided by BAC water. Draw volume is target dose divided by concentration. U-100 units are milliliters multiplied by 100.
Example: a 16 mg vial plus 2 mL of BAC water gives 8 mg/mL. A 4 mg dose is then 0.5 mL, which is 50 units on a U-100 syringe. A 10 mg vial plus 2 mL gives 5 mg/mL, so 4 mg becomes 0.8 mL, or 80 units.
Draw volume by dose at 8 mg/mL (16 mg vial + 2 mL)
Dose
1 mg
Volume
0.13 mL
U-100 units
~13 units
Dose
2 mg
Volume
0.25 mL
U-100 units
25 units
Dose
4 mg
Volume
0.50 mL
U-100 units
50 units
| Dose | Volume | U-100 units |
|---|---|---|
| 1 mg | 0.13 mL | ~13 units |
| 2 mg | 0.25 mL | 25 units |
| 4 mg | 0.50 mL | 50 units |
For a 10 mg vial with 2 mL water (5 mg/mL): 2 mg = 0.4 mL (40 units) and 4 mg = 0.8 mL (80 units). Use less water for a more concentrated mix and smaller draws.
- 01
Sanitize
Wipe the vial stopper and BAC water stopper with an alcohol swab.
- 02
Draw BAC water
Pull 2 mL of bacteriostatic water into a syringe.
- 03
Add slowly
Let the water run down the inside wall of the vial, not straight onto the powder.
- 04
Dissolve gently
Swirl, do not shake. Wait until the solution is clear.
- 05
Inspect
The solution should look clear and colorless. Discard it if it is cloudy or has particles.
- 06
Store cold
Refrigerate the mixed vial at 2-8C and keep it out of light.
- 07
Use within ~14 days
Use the reconstituted vial within about two weeks; discard leftover solution after that.
Calculator
Use a reconstitution calculator to match your exact vial size, BAC water volume, and target dose to milliliters and U-100 units.
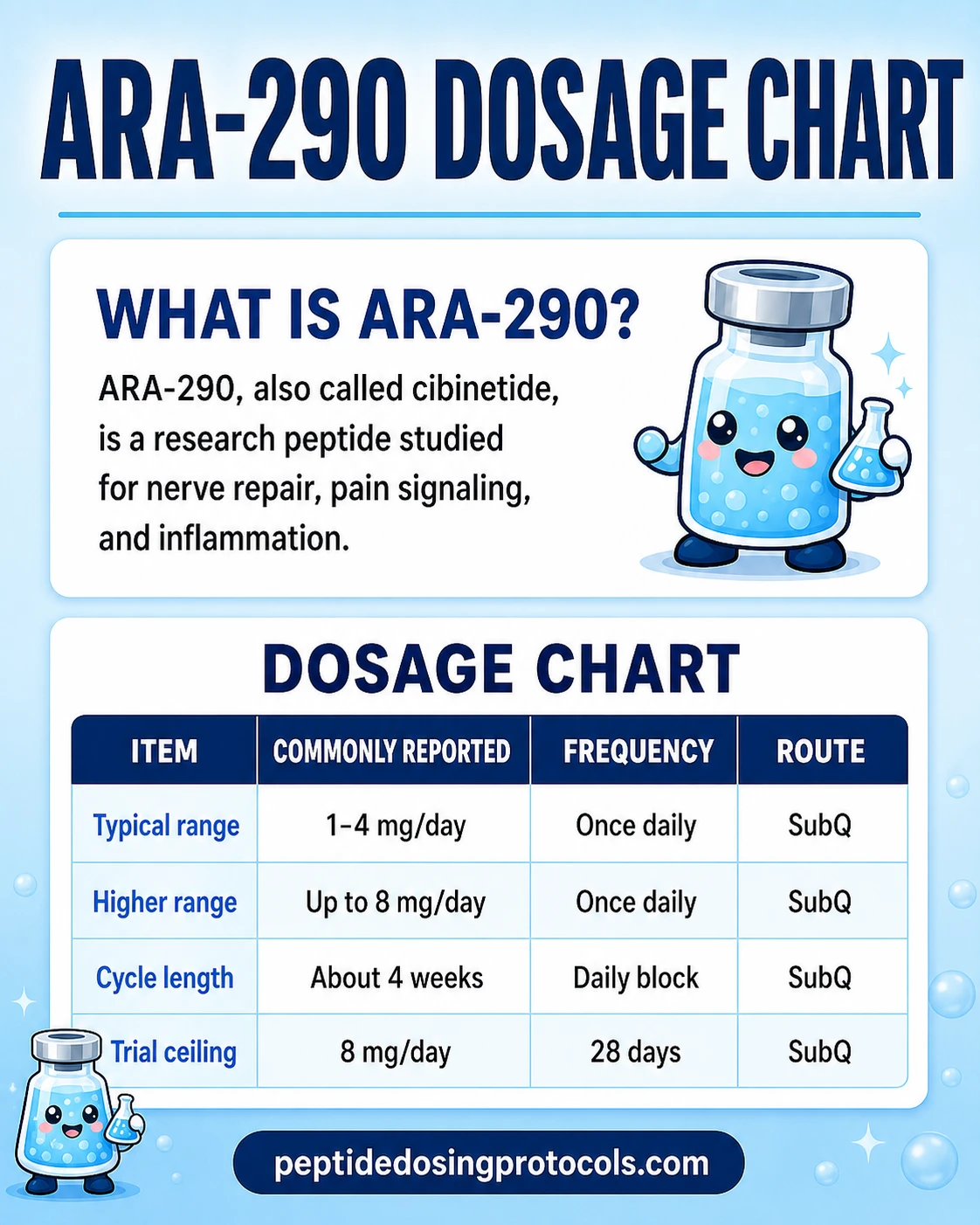
ARA-290 Dosage Chart
This chart summarizes the daily subcutaneous dosing pattern discussed above, including the reported range, cycle length, and route.
How ARA-290 Works
In plain terms, EPO does two separate jobs. One job tells bone marrow to make red blood cells. The other job protects and repairs injured tissue and calms inflammation. ARA-290 was designed to trigger only the second job.
It does this by selectively activating the innate repair receptor (IRR), a receptor complex made of the EPO receptor paired with the beta-common receptor (CD131). This is different from the classic EPO receptor pair that drives red-blood-cell production, which is why ARA-290 does not raise hematocrit. ARA-290 also appears to quiet the TRPV1 pain channel on small nerve fibers, which helps explain its effect on neuropathic pain.
- Selectively activates the innate repair receptor (EPOR + CD131).
- Drives anti-inflammatory, cytoprotective, and tissue-repair signaling.
- Does not stimulate red-blood-cell production (non-erythropoietic).
- Antagonizes the TRPV1 channel, linked to its pain effect.
Who Should Be Cautious With ARA-290
ARA-290 was generally well tolerated in short human trials, but the available safety data is limited to small groups and relatively brief study windows. These cautions are conservative research context, not a medical screening tool.
- Anyone who is pregnant or breastfeeding — there is no safety data.
- People with active cancer or blood disorders such as myeloproliferative conditions, given the EPO-derived design, as a conservative precaution.
- Anyone on other injectable therapies without clinician oversight.
- Anyone with a history of strong reactions to injected peptides.
Talk to a clinician
ARA-290 is not FDA-approved and has no established long-term safety profile. These cautions are drawn from its EPO lineage and general peptide-injection risks, not from a safety label.
ARA-290 Side Effects & Safety
Across the Phase 2 trials, ARA-290 was generally well tolerated. Reported effects were mostly mild and short-lived, and no serious drug-related safety problems were flagged in the published studies.
- Mild, transient injection-site reactions (redness or discomfort).
- Occasional headache reported at low frequency.
- No rise in red blood cells or hematocrit, by design.
- No anti-drug antibodies detected in the diabetic macular edema trial.
The important caveat is scale. Combined trial enrollment was under about 200 people, and treatment lasted weeks, not months. That means long-term safety at any dose is simply not characterized.
ARA-290 Expected Timeline & Monitoring
The trial timelines are short and specific. Most studies ran daily subcutaneous ARA-290 for 28 days. In the Phase 2b sarcoidosis trial, measurable nerve-fiber regrowth on corneal imaging and pain improvement were seen within that 28-day window. In the diabetes trial, some benefits persisted through a 28-day follow-up after dosing stopped.
For research planning, the main things to track are symptom scores, injection-site reactions, and any unexpected side effects. Because the compound is EPO-derived, some researchers also note red-blood-cell parameters as a precaution, even though trials showed no erythropoietic effect.
ARA-290 Clinical Evidence Context
ARA-290 has more human evidence than many peptides covered in research guides, but the evidence base is still small and stops at Phase 2. All the main trials were run or sponsored by the developer, Araim Pharmaceuticals.
Human ARA-290 (cibinetide) trials
Study
Sarcoidosis pilot (2012)
Design
22 patients, IV 2 mg 3x/week, 4 weeks
Key result
Improved neuropathy symptom score; safe
Study
Sarcoidosis SFN (2013)
Design
Daily subQ, 28 days, placebo-controlled
Key result
Better symptoms; increased corneal nerve fiber density
Study
Type 2 diabetes (2014)
Design
4 mg subQ daily, 28 days
Key result
Improved neuropathic symptoms, HbA1c, lipids, nerve density
Study
Phase 2b sarcoidosis (2017)
Design
64 patients, 1/4/8 mg subQ daily, 28 days
Key result
Met primary corneal nerve-regeneration endpoint; less pain
Study
Diabetic macular edema (2020)
Design
4 mg subQ daily, 12 weeks, 9 patients
Key result
No serious adverse events; small uncontrolled pilot
| Study | Design | Key result |
|---|---|---|
| Sarcoidosis pilot (2012) | 22 patients, IV 2 mg 3x/week, 4 weeks | Improved neuropathy symptom score; safe |
| Sarcoidosis SFN (2013) | Daily subQ, 28 days, placebo-controlled | Better symptoms; increased corneal nerve fiber density |
| Type 2 diabetes (2014) | 4 mg subQ daily, 28 days | Improved neuropathic symptoms, HbA1c, lipids, nerve density |
| Phase 2b sarcoidosis (2017) | 64 patients, 1/4/8 mg subQ daily, 28 days | Met primary corneal nerve-regeneration endpoint; less pain |
| Diabetic macular edema (2020) | 4 mg subQ daily, 12 weeks, 9 patients | No serious adverse events; small uncontrolled pilot |
All trials were Phase 2 or smaller, mostly single-institution, and short in duration.
The main limitation is the missing next step: no Phase 3 trial was completed, and the developer reportedly wound down operations with no active US IND as of 2026. That leaves promising Phase 2 signals for nerve pain and regeneration, but no completed approval path. Popular claims about broad anti-aging or bodybuilding benefits are not supported by these trials.
The evidence boundary
Human proof exists at the Phase 2 level for nerve-related endpoints in sarcoidosis and diabetes. It does not extend to Phase 3, to long-term safety, or to general wellness and performance claims.
ARA-290 Storage & Handling
ARA-290 storage
Lyophilized (Powder Form)
ARA-290 (cibinetide)
-4F (-20C) long-term
Reconstituted (Liquid Form)
ARA-290 (cibinetide)
35.6-46.4F (2-8C), use within ~14 days
Light
ARA-290 (cibinetide)
Protect from light
Appearance
ARA-290 (cibinetide)
Clear, colorless when mixed
| ARA-290 (cibinetide) | |
|---|---|
| Lyophilized (Powder Form) | -4F (-20C) long-term |
| Reconstituted (Liquid Form) | 35.6-46.4F (2-8C), use within ~14 days |
| Light | Protect from light |
| Appearance | Clear, colorless when mixed |
Keep reconstituted vials cold and out of light, and discard any solution that turns cloudy or is past its window.
ARA-290 Troubleshooting
- Cloudy or particle-filled solution: discard it; only use a clear, colorless solution.
- Draw looks too large at 4 mg: use less BAC water for a more concentrated vial, so the same dose is a smaller volume.
- Vial will not last the cycle: ARA-290 is milligram-heavy, so plan multiple vials or use a lower dose; do not keep a mixed vial past about 14 days.
- Injection-site irritation: rotate sites and inject slowly.
ARA-290 Regulatory Status
As of July 2026, ARA-290 (cibinetide) is not FDA-approved for any indication. It received FDA Orphan Drug and Fast Track designations for neuropathic pain in sarcoidosis, plus EU orphan designation, but those are development incentives, not approvals. No NDA or BLA was ever submitted.
Multiple industry and reference sources report that the developer, Araim Pharmaceuticals, has wound down, with no active US IND and no Phase 3 program. Reporting attributes the stall to commercial and organizational factors rather than a specific safety problem. ARA-290 sold as a research peptide is a research-use-only product, not an approved medicine, and is not the same as a licensed formulation.
ARA-290 vs BPC-157 and Nearby Peptides
ARA-290 is often compared to BPC-157 because both are discussed for repair. They are quite different. BPC-157 is a broad soft-tissue recovery peptide with mostly animal evidence. ARA-290 is a targeted innate-repair-receptor agonist with actual human Phase 2 data, but focused on nerve and inflammatory endpoints rather than general tissue repair.
Where ARA-290 sits
Peptide
ARA-290
Main research framing
Nerve repair, neuropathic pain, inflammation
Best human evidence
Phase 2 RCTs (sarcoidosis, diabetes)
Peptide
BPC-157
Main research framing
Broad soft-tissue recovery
Best human evidence
Mostly preclinical
Peptide
TB-500
Main research framing
Tissue repair and recovery
Best human evidence
Mostly preclinical
Peptide
KPV
Main research framing
Anti-inflammatory fragment
Best human evidence
Mostly preclinical
| Peptide | Main research framing | Best human evidence |
|---|---|---|
| ARA-290 | Nerve repair, neuropathic pain, inflammation | Phase 2 RCTs (sarcoidosis, diabetes) |
| BPC-157 | Broad soft-tissue recovery | Mostly preclinical |
| TB-500 | Tissue repair and recovery | Mostly preclinical |
| KPV | Anti-inflammatory fragment | Mostly preclinical |
These compounds are not interchangeable and are studied for different reasons.
FAQ
Q1: What is ARA-290 peptide?
ARA-290, also called cibinetide, is an 11-amino-acid peptide taken from one region of the erythropoietin (EPO) molecule. It activates the innate repair receptor to support tissue repair and reduce inflammation, but it does not raise red blood cells the way EPO does.
Q2: What is ARA-290 used for in research?
It has been studied mainly for small-fiber neuropathy in sarcoidosis and for diabetic neuropathy, where trials looked at nerve pain and nerve-fiber regeneration. Broader claims about anti-aging or bodybuilding are not backed by its human trials.
Q3: What is the ARA-290 dosage?
Human trials used daily subcutaneous ARA-290 in the 1-8 mg range, and 4 mg per day was the most-tested amount, usually for 28 days. Community structures mirror that, often 1-4 mg per day. See the dosing section for the trial doses.
Q4: How do you reconstitute ARA-290?
A common setup is a 16 mg vial plus 2 mL of bacteriostatic water, which gives 8 mg/mL. At that strength a 4 mg dose is 0.5 mL, or 50 units on a U-100 syringe. Keep the mixed vial refrigerated and use it within about 14 days.
Q5: Where do you inject ARA-290?
In trials and community use it is given as a subcutaneous injection, usually into the fat of the lower abdomen or thigh with a small insulin syringe. Rotating injection sites helps reduce local irritation.
Q6: What are the side effects of ARA-290?
Trials reported it as generally well tolerated, with mostly mild injection-site reactions and occasional headache. Because it is non-erythropoietic, it did not raise red blood cell counts. Long-term safety is unknown because studies were short and small.
Q7: Is ARA-290 FDA-approved?
No. As of July 2026 ARA-290 is not FDA-approved for any use. It holds FDA Orphan Drug and Fast Track designations for sarcoidosis-related neuropathic pain, but those are not approvals, and no Phase 3 was completed.
Q8: When will ARA-290 be available as a medicine?
There is no clear timeline. Reporting indicates the developer, Araim Pharmaceuticals, wound down and there is no active US clinical program or Phase 3 study, so an approval path would require a new sponsor to restart development.
Q9: ARA-290 vs BPC-157 — how do they differ?
BPC-157 is a broad soft-tissue recovery peptide with mostly animal evidence. ARA-290 is a targeted innate-repair-receptor agonist with actual human Phase 2 data, focused on nerve pain and nerve regeneration. They are not interchangeable.
Q10: Is this page medical advice?
No. This is an educational research reference. ARA-290 is not an approved medicine, and nothing here is a prescription or treatment plan. Talk to a qualified clinician before using any peptide.
Sources & Research
- 1. Heij L, Niesters M, Swartjes M, et al. Safety and efficacy of ARA 290 in sarcoidosis patients with symptoms of small fiber neuropathy: a randomized, double-blind pilot study. Molecular Medicine (2012)
- 2. Dahan A, Dunne A, Swartjes M, et al. ARA 290 improves symptoms in patients with sarcoidosis-associated small nerve fiber loss and increases corneal nerve fiber density. Molecular Medicine (2013)
- 3. Brines M, Dunne AN, van Velzen M, et al. ARA 290, a nonerythropoietic peptide engineered from erythropoietin, improves metabolic control and neuropathic symptoms in patients with type 2 diabetes. Molecular Medicine (2014)
- 4. Culver DA, Dahan A, Bajorunas D, et al. Cibinetide improves corneal nerve fiber abundance in patients with sarcoidosis-associated small nerve fiber loss and neuropathic pain (Phase 2b). Investigative Ophthalmology & Visual Science (IOVS) (2017)
- 5. Lois N, Gardner E, McFarland M, et al. A Phase 2 clinical trial on the use of cibinetide for the treatment of diabetic macular edema. Journal of Clinical Medicine (2020)
- 6. Peng B, Kong G, Yang C, Ming Y Erythropoietin and its derivatives: from tissue protection to immune regulation. Cell Death & Disease (review) (2020)
- 7. Dahan A, Brines M, Niesters M, Cerami A, van Velzen M Targeting the innate repair receptor to treat neuropathy. Pain Reports (review) (2016)
- 8. Wikipedia contributors Cibinetide (developmental code ARA-290) — development status. Wikipedia (secondary status reference) (2025)
- 9. Araim Pharmaceuticals Cibinetide (ARA 290) regenerates small nerve fibers and improves neuropathic clinical symptoms in sarcoidosis (Phase 2b announcement). PR Newswire (developer) (2017)
- 10. AdisInsight / Springer Cibinetide - Araim Pharmaceuticals (drug development record). AdisInsight (regulatory/status) (2022)
Related Dosing Protocols
Educational use only
This guide is an educational research reference, not medical advice or a treatment plan. ARA-290 is not FDA-approved for human use.
Calculate vial math
Use the calculator for custom vial size, BAC-water volume, and syringe-unit math.
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: Jul 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page