Oxytocin Quick Start
Oxytocin is a small peptide hormone made in the brain and released from the pituitary gland. In medicine, it is an FDA-approved drug given by IV or IM injection to start or strengthen labor, control bleeding after delivery, and support milk let-down. Outside of that obstetric use, researchers also study oxytocin given through the nose or as an injection under the skin to look at effects on stress, social behavior, and mood. Those routes are not FDA-approved.
This page is a research reference. It separates what is approved from what is investigational, gives plain reconstitution math for common vial sizes, and is honest about where the evidence is strong versus weak.
Route
Approved IV/IM in obstetrics. Intranasal (10-72 IU) and SubQ (100-500 mcg) are research-context only.
Measure
1 IU of oxytocin is about 2 mcg of pure peptide. A 2 mg vial is about 1,000 IU; a 5 mg vial is about 2,500 IU.
Reconstitute
Common research lab practice: add 2-3 mL bacteriostatic water to a 2 mg or 5 mg lyophilized vial.
Bioavailability
Intranasal bioavailability is about 1-2%. Subcutaneous oxytocin does not cross the blood-brain barrier meaningfully.
Evidence
Strong for obstetric IV use. Mixed and largely negative for autism social outcomes after SOARS-B (NEJM 2021).
Disclaimer
This page is an educational research reference and is not medical advice. Oxytocin labor induction is a hospital-only drug. Intranasal and subcutaneous oxytocin use outside of FDA-approved indications is investigational and should be discussed with a licensed clinician.
Oxytocin Dosing Protocol & Schedule
Oxytocin has very different dosing depending on route, because each route delivers a very different amount of the drug to the bloodstream and brain. The FDA-approved IV protocol for labor is dosed in milliunits per minute under continuous monitoring. The intranasal and subcutaneous routes used in research are dosed in international units (IU) or micrograms (mcg) per session.
Approved IV/IM obstetric label dosing
The FDA-approved oxytocin injection label (Pitocin and synthetic oxytocin USP) describes induction or augmentation of labor by IV infusion only, started at a low rate and titrated to uterine response. The usual starting infusion is around 0.5-1 milliunit per minute, raised gradually under continuous monitoring. This is a hospital-administered drug. This is not a dosing recommendation.
Obstetric oxytocin is hospital-only
Per the FDA label, IV oxytocin can cause uterine hyperstimulation, water intoxication with seizures, and maternal or fetal complications. It is only used under continuous clinical monitoring and is not part of any research-use protocol on this page.
Oxytocin research protocol formats
Choose the format you are researching to see route-specific notes. Intranasal is the only route with reasonable evidence for central nervous system effects in humans.
The most studied non-obstetric research route. Bioavailability is about 1-2%.
Intranasal oxytocin is the route used in most human social-cognition research. Doses in published trials range from about 10 to 72 IU per session, though larger does not always mean stronger. A 2021 dose-response brain imaging study found that smaller doses (around 9-18 IU) sometimes produced larger amygdala signals than 36 IU, consistent with the idea that oxytocin engages opposing intracellular pathways at higher concentrations.
Intranasal oxytocin doses commonly reported in published research
Trial context
Single-dose social-cognition studies
Per-session dose
24 IU
Frequency in trial
1x
Trial context
Dose-response brain imaging
Per-session dose
9, 18, or 36 IU
Frequency in trial
1x
Trial context
SOARS-B autism RCT (Sikich 2021)
Per-session dose
Up to 48 IU/day total
Frequency in trial
Split twice daily
Trial context
Adult ASD trials (Anagnostou 2012, others)
Per-session dose
24-48 IU/day total
Frequency in trial
Split twice daily
| Trial context | Per-session dose | Frequency in trial |
|---|---|---|
| Single-dose social-cognition studies | 24 IU | 1x |
| Dose-response brain imaging | 9, 18, or 36 IU | 1x |
| SOARS-B autism RCT (Sikich 2021) | Up to 48 IU/day total | Split twice daily |
| Adult ASD trials (Anagnostou 2012, others) | 24-48 IU/day total | Split twice daily |
These are study-arm doses pulled from published trials. They are not a dosing recommendation.
Intranasal absorption is sensitive to technique. Sprays should be aimed at the nasal mucosa, not the throat, and active nasal congestion likely reduces uptake. Reported bioavailability is in the 1-2% range, which is one reason that small differences in nasal device, head position, and timing matter in trials.
Used in some research-use peptide protocols but does not deliver oxytocin to the central nervous system in a way that mimics intranasal effects.
Subcutaneous oxytocin produces high plasma concentrations very quickly, but peripheral oxytocin does not cross the blood-brain barrier in meaningful amounts. That means subcutaneous dosing should not be expected to reproduce the behavioral effects seen with intranasal dosing.
Subcutaneous oxytocin ranges seen in research-use protocols
Range
Low
Per-dose amount
100 mcg
Frequency seen in protocols
Once daily
Range
Moderate
Per-dose amount
200-300 mcg
Frequency seen in protocols
Once daily
Range
Upper
Per-dose amount
400-500 mcg
Frequency seen in protocols
Once daily
| Range | Per-dose amount | Frequency seen in protocols |
|---|---|---|
| Low | 100 mcg | Once daily |
| Moderate | 200-300 mcg | Once daily |
| Upper | 400-500 mcg | Once daily |
These ranges come from community and research-use protocols, not from human RCT efficacy data. This is not a dosing recommendation.
Because plasma half-life is short (about 3-6 minutes), repeated daily injection produces brief peripheral spikes rather than steady central exposure. If a research question depends on engaging brain oxytocin receptors, the intranasal route has stronger pharmacologic justification.
Some compounding pharmacies prepare sublingual troches or drops; absorption is slower than intranasal and human evidence is limited.
Sublingual and buccal oxytocin formulations dissolve under the tongue or in the cheek and aim to bypass the gut, where the peptide degrades quickly. Compounded sublingual troches usually carry per-dose amounts in the low-hundreds-of-IU range, but the human pharmacokinetic and efficacy data are limited compared with intranasal use. Effects may take 15-30 minutes to begin and the duration is shorter than intravenous administration.
Evidence boundary
No large randomized trials have tested sublingual oxytocin against intranasal oxytocin for social-cognition endpoints. Treat sublingual protocols as community-derived rather than evidence-based.
Cycle and review pattern seen in research-use protocols
Approach
Single dose
Duration
1 session
Review Point
Same day
Notes
Used in many social-cognition studies; effects measured within 30-90 minutes.
Approach
Short cycle
Duration
1-2 weeks
Review Point
Week 2
Notes
Used in mood, anxiety, and pain research blocks.
Approach
Standard cycle
Duration
4-6 weeks
Review Point
Week 4
Notes
Common research-use planning length; followed by a 1-2 week off period.
Approach
Extended cycle
Duration
24 weeks
Review Point
Week 12
Notes
Mirrors the SOARS-B autism RCT length (which did not show benefit).
| Approach | Duration | Review Point | Notes |
|---|---|---|---|
| Single dose | 1 session | Same day | Used in many social-cognition studies; effects measured within 30-90 minutes. |
| Short cycle | 1-2 weeks | Week 2 | Used in mood, anxiety, and pain research blocks. |
| Standard cycle | 4-6 weeks | Week 4 | Common research-use planning length; followed by a 1-2 week off period. |
| Extended cycle | 24 weeks | Week 12 | Mirrors the SOARS-B autism RCT length (which did not show benefit). |
These are protocol structures used in published research, not personal recommendations.
Oxytocin Supplies Needed
Affiliate disclosure: PDP may earn a commission when you use eligible supplier links, at no extra cost to you. The supplies math below assumes a 5 mg vial reconstituted with 3.0 mL bacteriostatic water for daily subcutaneous research-context dosing at 200 mcg. Intranasal protocols using compounded sprays are typically prepared by pharmacies and will not match these vial counts.
Recommended USA Supply
Use discount code SAVE10 at Peptira checkout. See why we love Peptira.

Oxytocin

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Peptide Vials
Based on 200 mcg/day subcutaneous research planning. A 5 mg vial covers about 25 planned daily doses.
| Cycle length | Planning note |
|---|---|
4-6 weeks 2 vials | 4 weeks: 28 injections; 1 vial covers ~25 doses, second vial gives margin.; 6 weeks: 42 injections; 2 x 5 mg covers ~50 doses. |
8 weeks 3 vials | 56 injections; 2 vials cover ~50, third gives margin. |
12 weeks 4 vials | 84 injections; 4 x 5 mg covers ~100 planned doses. |
4-6 weeks
2 vials
4 weeks: 28 injections; 1 vial covers ~25 doses, second vial gives margin.; 6 weeks: 42 injections; 2 x 5 mg covers ~50 doses.
8 weeks
3 vials
56 injections; 2 vials cover ~50, third gives margin.
12 weeks
4 vials
84 injections; 4 x 5 mg covers ~100 planned doses.
Bacteriostatic Water
3.0 mL per 5 mg vial yields about 1.67 mg/mL (1,670 mcg/mL).
| Cycle length | Planning note |
|---|---|
4-8 weeks 1 x 10 mL bottle | 4 weeks: Two vials use 6 mL; one bottle gives margin.; 6 weeks: Two vials use 6 mL; one bottle covers it.; 8 weeks: Three vials use 9 mL; one bottle still covers it. |
12 weeks 2 x 10 mL bottles | Four vials use 12 mL; second bottle gives margin. |
4-8 weeks
1 x 10 mL bottle
4 weeks: Two vials use 6 mL; one bottle gives margin.; 6 weeks: Two vials use 6 mL; one bottle covers it.; 8 weeks: Three vials use 9 mL; one bottle still covers it.
12 weeks
2 x 10 mL bottles
Four vials use 12 mL; second bottle gives margin.
Insulin Syringes (U-100)
Daily subcutaneous draws. 1 unit on a U-100 syringe equals 0.01 mL, which at 1.67 mg/mL is about 16.7 mcg.
| Cycle length | Planning note |
|---|---|
4 weeks 28 syringes | 1 syringe per day; recommend 30 to allow for damaged draws. |
6 weeks 42 syringes | 1 syringe per day; recommend a 50-count pack. |
8 weeks 56 syringes | 1 syringe per day; one 100-count box covers it. |
12 weeks 84 syringes | 1 syringe per day; one 100-count box covers it. |
4 weeks
28 syringes
1 syringe per day; recommend 30 to allow for damaged draws.
6 weeks
42 syringes
1 syringe per day; recommend a 50-count pack.
8 weeks
56 syringes
1 syringe per day; one 100-count box covers it.
12 weeks
84 syringes
1 syringe per day; one 100-count box covers it.
Round up for priming losses, damaged syringes, and protocol adjustments. Intranasal-only protocols typically use a pharmacy-prepared spray and will not need this syringe and swab supply.
Companion Supplies & Routine Support
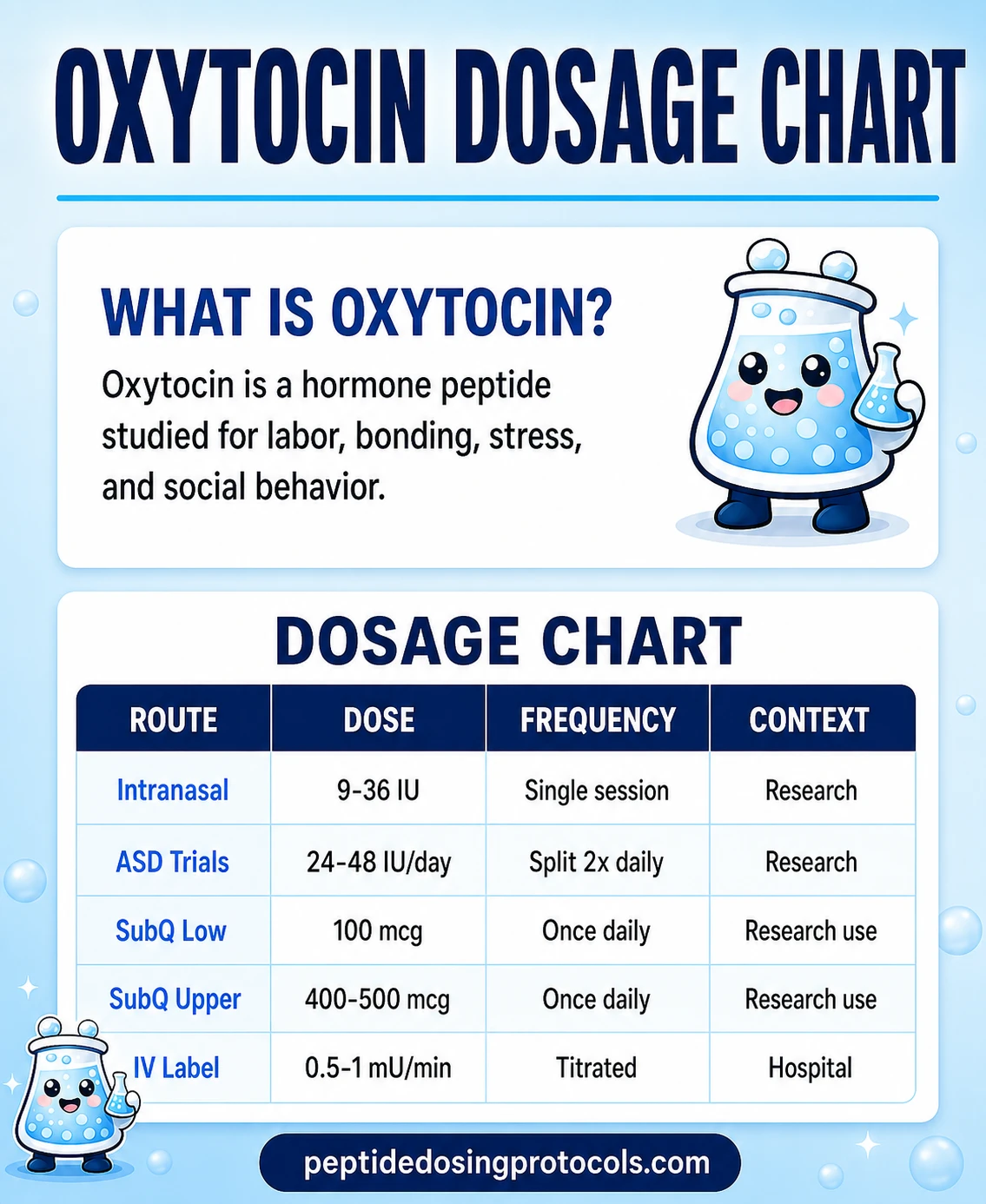
Oxytocin Dosage Chart
This Oxytocin dosage chart summarizes the intranasal, SubQ, and IV label dose contexts shown in the dosing section above.
Oxytocin Reconstitution Guide
Lyophilized research-use oxytocin is sold as a freeze-dried powder in 2 mg, 5 mg, or 10 mg vials. To use it in a research protocol, the powder must be reconstituted with bacteriostatic water (sterile water with 0.9% benzyl alcohol) so it can be drawn into a syringe.
IU to mcg conversion (oxytocin specific)
One international unit (IU) of oxytocin is approximately 2 micrograms of pure peptide. That means a 2 mg vial contains roughly 1,000 IU, a 5 mg vial contains roughly 2,500 IU, and a 10 mg vial contains roughly 5,000 IU.
Common oxytocin reconstitution math (research-context)
Vial size
2 mg (~1,000 IU)
BAC water
2.0 mL
Concentration
~1.0 mg/mL (~500 IU/mL)
Per 10-unit draw (U-100)
~100 mcg / ~50 IU
Vial size
2 mg (~1,000 IU)
BAC water
3.0 mL
Concentration
~0.67 mg/mL (~333 IU/mL)
Per 10-unit draw (U-100)
~67 mcg / ~33 IU
Vial size
5 mg (~2,500 IU)
BAC water
3.0 mL
Concentration
~1.67 mg/mL (~833 IU/mL)
Per 10-unit draw (U-100)
~167 mcg / ~83 IU
Vial size
5 mg (~2,500 IU)
BAC water
5.0 mL
Concentration
~1.0 mg/mL (~500 IU/mL)
Per 10-unit draw (U-100)
~100 mcg / ~50 IU
Vial size
10 mg (~5,000 IU)
BAC water
5.0 mL
Concentration
~2.0 mg/mL (~1,000 IU/mL)
Per 10-unit draw (U-100)
~200 mcg / ~100 IU
| Vial size | BAC water | Concentration | Per 10-unit draw (U-100) |
|---|---|---|---|
| 2 mg (~1,000 IU) | 2.0 mL | ~1.0 mg/mL (~500 IU/mL) | ~100 mcg / ~50 IU |
| 2 mg (~1,000 IU) | 3.0 mL | ~0.67 mg/mL (~333 IU/mL) | ~67 mcg / ~33 IU |
| 5 mg (~2,500 IU) | 3.0 mL | ~1.67 mg/mL (~833 IU/mL) | ~167 mcg / ~83 IU |
| 5 mg (~2,500 IU) | 5.0 mL | ~1.0 mg/mL (~500 IU/mL) | ~100 mcg / ~50 IU |
| 10 mg (~5,000 IU) | 5.0 mL | ~2.0 mg/mL (~1,000 IU/mL) | ~200 mcg / ~100 IU |
All values rounded for readability. Use a reconstitution calculator for exact draws.
- 01
Inspect the vial
Check the label for compound name, vial size, lot number, and expiry. Confirm the lyophilized cake looks intact.
- 02
Choose your BAC volume
Match BAC water volume to the dosing math you want. 3.0 mL into a 5 mg vial is a common starting point.
- 03
Wipe the stoppers
Swab the BAC water vial stopper and the peptide vial stopper with separate sterile alcohol pads.
- 04
Draw the BAC water
Draw your chosen volume into a sterile syringe. Use one syringe for reconstitution and a separate sterile syringe for drawing daily doses.
- 05
Inject slowly down the vial wall
Angle the needle so the bacteriostatic water runs down the inside wall of the peptide vial rather than directly onto the powder.
- 06
Swirl gently
Roll or swirl until the cake fully dissolves. Do not shake hard; mechanical foaming can damage peptides.
- 07
Inspect and refrigerate
The solution should be clear and free of particulates. Store at 2-8 degrees Celsius (35.6-46.4 degrees Fahrenheit) between uses.
Need exact math?
Use the reconstitution calculator to plug in vial size, BAC water volume, and target dose for a syringe-units answer.
How Oxytocin Works
Oxytocin is a cyclic 9-amino-acid peptide (Cys-Tyr-Ile-Gln-Asn-Cys-Pro-Leu-Gly-NH2, molecular formula C43H66N12O12S2, ~1,007 daltons). The two cysteine residues form a sulfur bridge that gives the molecule a small ring plus a short tail.
It is made in the paraventricular and supraoptic nuclei of the hypothalamus and released two ways. Released into the bloodstream from the posterior pituitary, it acts on uterine smooth muscle to drive labor contractions and on mammary myoepithelial cells to trigger milk let-down. Released centrally from oxytocin neurons that project to other brain regions, it acts on the oxytocin receptor (a G-protein-coupled receptor) in places like the amygdala, nucleus accumbens, and brainstem.
The behavioral effects studied in human research - changes in social attention, trust, and emotional response to faces - depend on central oxytocin activity. That is the main reason peripheral routes like subcutaneous injection are not expected to reproduce intranasal effects: the molecule does not cross the blood-brain barrier easily, and only a small fraction of intranasally administered oxytocin (about 1-2%) reaches the bloodstream, with a smaller fraction reaching the brain through nose-to-brain pathways.
- Cyclic nonapeptide with a disulfide bridge between Cys1 and Cys6.
- Binds the oxytocin receptor (OTR), a class A GPCR with shared homology to vasopressin receptors.
- Plasma half-life is short: 3-6 minutes by IV. Central half-life after intranasal dosing is longer (estimated ~20 minutes).
- Engages both excitatory (Gq) and inhibitory (Gi) intracellular pathways, which is one reason dose-response curves can be non-linear.
Who Oxytocin Is For and Who Should Avoid It
Approved oxytocin (IV/IM Pitocin) is used in obstetric settings under direct clinical supervision. Research-use intranasal or subcutaneous oxytocin is studied in healthy adult volunteers and in trials of conditions such as autism spectrum disorder, anxiety, and pain. It should not be used outside of those settings without clinical oversight.
- Pregnancy: oxytocin should never be used during pregnancy outside of approved medical induction in a hospital. Inappropriate use can cause uterine rupture, fetal distress, or worse.
- Cardiovascular conditions: the FDA label notes risks of arrhythmia and water intoxication; people with cardiovascular disease, hyponatremia, or severe cardiac conditions need clinician oversight before any oxytocin exposure.
- Hyponatremia or fluid-restricted conditions: oxytocin has antidiuretic activity that can cause water intoxication and seizures, especially with prolonged IV infusion.
- Hypersensitivity to oxytocin or chlorobutanol (the preservative in some IV formulations).
- Children and adolescents: studied in the SOARS-B autism trial, but ongoing dosing outside research settings is not supported by efficacy data.
- Anyone on lithium, prostaglandin analogues, or other agents with uterotonic or fluid-balance interactions should not combine those with oxytocin without clinician oversight.
Clinician oversight matters
Anyone considering research-use intranasal or subcutaneous oxytocin should discuss it with a licensed clinician first, especially with a history of cardiovascular disease, hyponatremia, pregnancy, or psychiatric medication use.
Oxytocin Side Effects & Safety
Oxytocin's safety profile depends a lot on the route. The IV obstetric label carries a strong warning list. Intranasal oxytocin used in short-term research has generally been well tolerated, though the longest large trial in autism (SOARS-B, NEJM 2021) reported no serious safety signal but also no benefit.
IV / IM obstetric label safety (FDA)
- Uterine hyperstimulation, uterine rupture, postpartum hemorrhage.
- Water intoxication with seizures and coma, linked to oxytocin's antidiuretic effect during long infusions.
- Maternal arrhythmias, premature ventricular contractions, hypertension or hypotension.
- Fetal bradycardia, arrhythmia, hypoxia, and neonatal complications.
Intranasal route (research context)
- Mild nasal irritation, sneezing, runny nose.
- Transient headache or fatigue.
- Occasional reports of irritability or mood changes, particularly at higher doses.
- SOARS-B (24-week, N=290) reported no oxytocin-vs-placebo difference in serious adverse events.
Subcutaneous route (research context)
- Injection-site redness, bruising, or soreness.
- Short peripheral plasma spikes; no clear central nervous system effects.
- Quality control risk: research-use peptide vials vary in purity and require batch COA review.
Water intoxication is dose-related
The water-intoxication risk in the FDA label is tied to long, high-rate IV infusion. Single low-IU intranasal research doses do not carry the same risk profile, but it is still a documented oxytocin effect and a reason high-dose intranasal regimens deserve clinician oversight.
Oxytocin Timeline & What to Monitor
Oxytocin's plasma half-life is short: roughly 3-6 minutes after IV administration in non-pregnant adults. Central effects from intranasal dosing are believed to last longer, around 20 minutes to a few hours depending on the endpoint and dose. Most acute social-cognition trials measure outcomes within 30-90 minutes of administration.
Reported timing in published research
Endpoint
Plasma peak after IV
Study type
PK study
Timing
Within minutes
Endpoint
Plasma peak after intranasal
Study type
PK study
Timing
~15-30 minutes
Endpoint
CSF detection after intranasal
Study type
Primate / human PK
Timing
Within 30-75 minutes (limited data)
Endpoint
Social-cognition behavioral endpoints
Study type
Acute RCT
Timing
30-90 minutes post-dose
Endpoint
Longer-term symptom endpoints (autism)
Study type
Phase 2 RCT (SOARS-B)
Timing
12-24 weeks of treatment
| Endpoint | Study type | Timing |
|---|---|---|
| Plasma peak after IV | PK study | Within minutes |
| Plasma peak after intranasal | PK study | ~15-30 minutes |
| CSF detection after intranasal | Primate / human PK | Within 30-75 minutes (limited data) |
| Social-cognition behavioral endpoints | Acute RCT | 30-90 minutes post-dose |
| Longer-term symptom endpoints (autism) | Phase 2 RCT (SOARS-B) | 12-24 weeks of treatment |
These reflect study timing, not personal use timelines.
Reasonable things to track in a research planning context are nasal tolerance (for intranasal), injection-site response (for subcutaneous), sleep, mood, and any objective endpoint the protocol is built around. Subjective "effect" reports from short-term oxytocin are notoriously variable between people, partly because of OXTR receptor genotype differences.
When effects do not show up
Lack of subjective effect from oxytocin is common, especially with subcutaneous-only protocols. That is consistent with the pharmacology: peripheral routes do not deliver enough peptide to the brain to mimic intranasal effects.
Oxytocin Clinical Evidence Context
Oxytocin's evidence base splits into approved obstetric use, where evidence is strong and decades old, and investigational research use, where the picture is mixed and often disappointing.
Approved IV obstetric use
Oxytocin injection USP is FDA-approved for labor induction, augmentation of dysfunctional labor, control of postpartum bleeding, and adjunctive therapy for management of incomplete or inevitable abortion. The drug has been used clinically since the 1950s after Vincent du Vigneaud synthesized it (1953 Nobel Prize). The current FDA label describes specific milliunit-per-minute infusion protocols under continuous monitoring.
Autism spectrum disorder
The largest randomized trial of intranasal oxytocin in autism is the SOARS-B trial (Sikich et al., NEJM 2021). It enrolled 290 children and adolescents (ages 3-17) with autism spectrum disorder, randomized 1:1 to intranasal oxytocin (up to 48 IU/day) or placebo, with a 24-week treatment period. The primary endpoint (change in the Aberrant Behavior Checklist modified Social Withdrawal subscale) showed no significant difference between groups, and no secondary social or cognitive endpoint reached significance either. Adverse events were similar between groups. The trial's lead author called the result "a major setback" for the autism oxytocin hypothesis.
Social cognition in healthy adults
The Kosfeld et al. trust-game study (Nature, 2005) is the most-cited early human social-cognition trial and reported increased trust behavior after 24 IU intranasal oxytocin. Many smaller follow-ups have produced inconsistent results. A 2018 meta-analysis (Keech, Crowe, Hocking) across neurodevelopmental disorders described intranasal oxytocin's social-cognition effects as "inconclusive." A 2024 multilevel meta-analysis of 28 ASD studies (N=726) found small beneficial effects on social functioning but not on non-social autism symptoms.
Other research areas
Anxiety and PTSD
Small RCTs and reviews suggest possible reductions in amygdala reactivity, but no large Phase 3 evidence supports clinical use.
Pain and migraine
Small human trials of intranasal oxytocin for migraine and chronic pain have produced mixed signals; not a standard treatment.
Obesity and metabolism
Early human trials of intranasal oxytocin and body weight have shown modest signals in some studies but inconsistent results overall.
Sleep apnea
Mechanistic work shows oxytocin's role in cardiac vagal neurons and breathing; early clinical signals for obstructive sleep apnea exist but are preliminary.
Oxytocin Storage & Handling
Storage matters because oxytocin is a small peptide that degrades with heat, freeze-thaw cycles, and microbial contamination. Approved injectable oxytocin labels list refrigerated storage. Research-use lyophilized vials are typically stored frozen until reconstitution and refrigerated afterward.
Oxytocin storage at a glance
Temperature
Lyophilized (powder)
-4 degrees F (-20 degrees C) long-term
Reconstituted (liquid)
35.6 to 46.4 degrees F (2 to 8 degrees C)
Practical shelf life
Lyophilized (powder)
Until labeled expiry
Reconstituted (liquid)
About 2-4 weeks once reconstituted with BAC water
Appearance
Lyophilized (powder)
White lyophilized cake
Reconstituted (liquid)
Clear, colorless solution
Avoid
Lyophilized (powder)
Repeated freeze-thaw cycles, direct sunlight
Reconstituted (liquid)
Freezing the reconstituted solution
| Lyophilized (powder) | Reconstituted (liquid) | |
|---|---|---|
| Temperature | -4 degrees F (-20 degrees C) long-term | 35.6 to 46.4 degrees F (2 to 8 degrees C) |
| Practical shelf life | Until labeled expiry | About 2-4 weeks once reconstituted with BAC water |
| Appearance | White lyophilized cake | Clear, colorless solution |
| Avoid | Repeated freeze-thaw cycles, direct sunlight | Freezing the reconstituted solution |
Approved Pitocin / oxytocin USP injectable solutions are stored per their individual FDA labels.
- Protect from light. Some manufacturer instructions recommend opaque storage.
- Do not freeze reconstituted solution. Refrigerate.
- Discard if the solution becomes cloudy or develops particulates.
Oxytocin Protocol Mistakes & Troubleshooting
- Spraying intranasal oxytocin into the throat instead of the nasal mucosa: most likely the single biggest cause of "no effect." Re-check head position and device technique.
- Using subcutaneous oxytocin and expecting central nervous system effects: peripheral plasma rises but the blood-brain barrier blocks most of it.
- Reconstituting with regular sterile water for a multi-dose vial: without bacteriostatic preservative, the open vial becomes a contamination risk within hours.
- Skipping the IU-to-mcg conversion: 1 IU is about 2 mcg; mis-converting can lead to 10x dosing errors.
- Storing reconstituted vials in the freezer: freezing can damage the peptide and is not the recommended storage for reconstituted oxytocin.
- Assuming a single dose during the day is enough for a 24-week trial: SOARS-B used twice-daily intranasal dosing and still found no benefit.
- Treating compounded sublingual troches as equivalent to intranasal: absorption and pharmacokinetics differ.
If side effects appear
Stop, document the dose and route, and consult a clinician. Headache, prolonged nausea, mood changes, or unexpected fluid retention warrant cessation and review.
Oxytocin Regulatory Status
As of June 2026, oxytocin's regulatory status depends entirely on route and formulation.
- FDA-approved (United States): IV and IM oxytocin injection USP (e.g., Pitocin) is approved for labor induction, labor augmentation, postpartum hemorrhage control, and milk let-down support. Current Pitocin labeling has been updated through 2021-2022 in the FDA Drugs@FDA database.
- Not FDA-approved: intranasal oxytocin, subcutaneous oxytocin for behavioral or research uses, sublingual troches, and any over-the-counter "oxytocin" nasal mist sold as a supplement.
- Compounded (503A pharmacies): compounded intranasal sprays, sublingual troches, and injections exist with a prescription. These are compounded products, not FDA-approved drugs.
- Research-use lyophilized peptide vials: sold for research use only, not for human consumption. These vials carry no FDA approval as a drug.
- European Medicines Agency: Syntocinon (oxytocin) is approved for obstetric use. Intranasal Syntocinon was historically marketed for milk let-down in some EU countries but has been discontinued in several markets.
Compounded versus research-use
Compounded oxytocin from a 503A pharmacy is a different category than research-use lyophilized peptide vials, and the two should not be treated as interchangeable.
Oxytocin vs Pitocin vs Syntocinon vs Kisspeptin
A few nearby names cause confusion in search results. "Pitocin" and "Syntocinon" are brand names for the same synthetic oxytocin. They are not different peptides. Kisspeptin is a separate hypothalamic peptide that is sometimes researched alongside oxytocin in reproductive and behavioral neuroscience.
Names and nearby compounds
Name
Oxytocin
What it is
Endogenous peptide hormone; synthesized for clinical use
Notes
FDA-approved (IV/IM) obstetric drug; investigational for other routes.
Name
Pitocin
What it is
US brand name for synthetic oxytocin injection
Notes
Same molecule as oxytocin USP.
Name
Syntocinon
What it is
International brand name for synthetic oxytocin
Notes
Was marketed as intranasal milk let-down spray; mostly discontinued.
Name
Carbetocin
What it is
Long-acting oxytocin analog (Duratocin/Pabal)
Notes
Approved in many countries for postpartum hemorrhage; not FDA-approved in the US.
Name
Vasopressin (AVP)
What it is
Sister neurohypophysial peptide, differs from oxytocin by 2 amino acids
Notes
Different receptor (V1a/V1b/V2); fluid balance and stress role, not labor or social cognition.
Name
Kisspeptin
What it is
Separate hypothalamic peptide
Notes
Linked to GnRH/reproductive axis; sometimes studied in behavioral neuroscience but a different system.
Name
PT-141 (bremelanotide)
What it is
Melanocortin receptor agonist
Notes
Not an oxytocin analog; sometimes paired with oxytocin in community sexual-function research but pharmacologically distinct.
| Name | What it is | Notes |
|---|---|---|
| Oxytocin | Endogenous peptide hormone; synthesized for clinical use | FDA-approved (IV/IM) obstetric drug; investigational for other routes. |
| Pitocin | US brand name for synthetic oxytocin injection | Same molecule as oxytocin USP. |
| Syntocinon | International brand name for synthetic oxytocin | Was marketed as intranasal milk let-down spray; mostly discontinued. |
| Carbetocin | Long-acting oxytocin analog (Duratocin/Pabal) | Approved in many countries for postpartum hemorrhage; not FDA-approved in the US. |
| Vasopressin (AVP) | Sister neurohypophysial peptide, differs from oxytocin by 2 amino acids | Different receptor (V1a/V1b/V2); fluid balance and stress role, not labor or social cognition. |
| Kisspeptin | Separate hypothalamic peptide | Linked to GnRH/reproductive axis; sometimes studied in behavioral neuroscience but a different system. |
| PT-141 (bremelanotide) | Melanocortin receptor agonist | Not an oxytocin analog; sometimes paired with oxytocin in community sexual-function research but pharmacologically distinct. |
These are not interchangeable substances. Each has its own evidence and regulatory profile.
Oxytocin Blood Tests & Monitoring
Oxytocin is usually discussed in social, bonding, sexual-function, and neuroendocrine contexts. Routine labs do not measure its behavioral response, so monitoring focuses on pregnancy context, medications, and broad health review.
Blood test markers to discuss with a clinician
Marker
Pregnancy test
Why it matters
Pregnancy status is important because oxytocin has reproductive and uterine relevance.
Timing
Baseline
Marker
Comprehensive metabolic panel (CMP)
Why it matters
Reviews electrolytes, kidney markers, liver enzymes, and glucose in one broad screen.
Timing
Baseline
Marker
Blood pressure and resting heart rate
Why it matters
Adds cardiovascular context when symptoms such as dizziness, flushing, or palpitations occur.
Timing
Baseline
Marker
TSH and free T4
Why it matters
Thyroid status can affect mood, energy, and reproductive symptoms.
Timing
Optional
| Marker | Why it matters | Timing |
|---|---|---|
| Pregnancy test | Pregnancy status is important because oxytocin has reproductive and uterine relevance. | Baseline |
| Comprehensive metabolic panel (CMP) | Reviews electrolytes, kidney markers, liver enzymes, and glucose in one broad screen. | Baseline |
| Blood pressure and resting heart rate | Adds cardiovascular context when symptoms such as dizziness, flushing, or palpitations occur. | Baseline |
| TSH and free T4 | Thyroid status can affect mood, energy, and reproductive symptoms. | Optional |
Monitoring guidance is neuroendocrine and reproductive-context based rather than based on routine oxytocin lab tracking.
At-home blood test option
Easy at home option to monitor core metrics during research cycles.
Partner link: PDP may earn a commission at no cost to you.
Simple timing framework
Baseline
Discuss baseline review before use, especially with pregnancy potential, psychiatric history, blood pressure issues, sodium balance concerns, or medication use.
Follow-up
Review symptoms and relevant markers after early exposure or dose changes if the protocol continues.
Longer term
For repeated protocols, review medication changes, mood symptoms, and broad health context periodically.
How to interpret the labs
- Behavioral and social effects are not reliably captured by routine labs.
- Psychiatric history, relationship context, medications, and pregnancy status matter during interpretation.
- Electrolyte and fluid-balance context may matter when symptoms suggest it.
Do not wait for routine labs
Severe mood changes, fainting, chest pain, severe headache, allergic symptoms, or pregnancy-related symptoms need medical review.
FAQ
Q1: Is oxytocin FDA approved?
Yes for one set of uses, no for others. IV and IM oxytocin injection USP is FDA-approved for labor induction, labor augmentation, postpartum hemorrhage control, and milk let-down support. Intranasal oxytocin, subcutaneous oxytocin, and sublingual oxytocin are not FDA-approved as of June 2026. They are investigational or research-use only.
Q2: How much oxytocin is in 1 IU?
Approximately 2 micrograms of pure peptide. That conversion is consistent across labels and PubChem chemistry data. So a 2 mg vial holds roughly 1,000 IU and a 5 mg vial holds roughly 2,500 IU.
Q3: What is the typical intranasal oxytocin dose used in research?
Most human social-cognition trials use somewhere between 10 and 72 IU per session, with 24 IU being the most cited single-session dose since the Kosfeld 2005 Nature trust-game study. The SOARS-B autism trial used up to 48 IU per day split twice daily. These are research-arm doses, not personal recommendations.
Q4: Does subcutaneous oxytocin work like intranasal oxytocin?
Not for central nervous system effects. Subcutaneous oxytocin produces a quick rise in plasma levels but does not cross the blood-brain barrier in meaningful amounts. That is why research targeting brain oxytocin receptors (for example, social cognition) uses the intranasal route rather than subcutaneous.
Q5: How long does oxytocin last after reconstitution?
Reconstituted research-use oxytocin in bacteriostatic water is typically considered usable for about 2-4 weeks when stored at 2-8 degrees Celsius (35.6 to 46.4 degrees Fahrenheit). Discard if it becomes cloudy or develops particulates. Approved injectable oxytocin solutions follow their own FDA-labeled storage instructions.
Q6: How do I reconstitute a 5 mg oxytocin vial?
A common research-lab approach is to add 3.0 mL of bacteriostatic water, which gives about 1.67 mg/mL (roughly 833 IU/mL). On a U-100 insulin syringe, 10 units (0.10 mL) is then about 167 mcg or 83 IU. Use the reconstitution calculator to match BAC water volume to your target dose.
Q7: Does the largest oxytocin trial in autism show it works?
No. The SOARS-B trial (Sikich et al., NEJM 2021), with 290 children and adolescents over 24 weeks, found no significant difference between intranasal oxytocin and placebo on its primary or secondary social and cognitive endpoints. Smaller earlier studies had been more positive, but this larger trial is the strongest evidence to date.
Q8: Can oxytocin be used for anxiety, depression, or PTSD?
There are small human studies suggesting oxytocin may reduce amygdala reactivity or change some anxiety-related measures, but it is not FDA-approved for any psychiatric condition and large trials have generally not supported clinical use. People considering this should talk to a licensed clinician rather than self-administer.
Q9: What are the most important oxytocin side effects?
For IV obstetric use, the most important effects are uterine hyperstimulation, water intoxication with seizures, and maternal or fetal complications - which is why it is hospital-administered. For intranasal research-context use, side effects are usually mild (nasal irritation, transient headache, occasional irritability). Subcutaneous research-context use can cause injection-site reactions.
Q10: Is this page medical advice?
No. This is an educational research summary, not personal medical advice. Approved oxytocin (Pitocin) is a hospital drug. Intranasal, subcutaneous, and sublingual oxytocin are investigational or research-use only. Anyone considering oxytocin in any form should talk with a licensed clinician.
Sources & Research
- 1. U.S. Food and Drug Administration Oxytocin Injection, USP (synthetic) - Current FDA label (NDA 018261 / 018248). FDA Drugs@FDA (2022)
- 2. U.S. Food and Drug Administration Pitocin (oxytocin injection, USP) - Prescribing information (NDA 018261). FDA Drugs@FDA (2021)
- 3. Sikich L, Kolevzon A, King BH, McDougle CJ, et al. Intranasal Oxytocin in Children and Adolescents with Autism Spectrum Disorder. New England Journal of Medicine (2021)
- 4. Kosfeld M, Heinrichs M, Zak PJ, Fischbacher U, Fehr E. Oxytocin increases trust in humans. Nature (2005)
- 5. Quintana DS, Westlye LT, et al. Advances in the field of intranasal oxytocin research: lessons learned and future directions for clinical research. Molecular Psychiatry / PMC (2021)
- 6. Martins D, Brodmann K, Veronese M, et al. "Less is more": a dose-response account of intranasal oxytocin pharmacodynamics in the human brain. bioRxiv (preprint, Imperial College London team) (2021)
- 7. Higgins DT, Sutton MM, et al. Plasma pharmacokinetics of intravenous and intranasal oxytocin in nonpregnant adults. Peptides / PubMed (2025)
- 8. Audunsdottir K, Sartorius AM, Kang H, et al. The effects of oxytocin administration on social and routinized behaviors in autism: a preregistered systematic review and meta-analysis. Psychoneuroendocrinology (2024)
- 9. Ooi YP, Weng SJ, Kossowsky J, Gerger H, Sung M. Oxytocin and Autism Spectrum Disorders: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pharmacopsychiatry (2017)
- 10. Keech B, Crowe S, Hocking DR. Intranasal oxytocin, social cognition and neurodevelopmental disorders: A meta-analysis. Psychoneuroendocrinology (2018)
- 11. National Center for Biotechnology Information Oxytocin (Compound CID 439302) - structure and properties. PubChem (2026)
- 12. Waltenspuhl Y, Schoppe J, Ehrenmann J, et al. Crystal structure of the human oxytocin receptor. Science Advances / bioRxiv preprint (2020)
- 13. ClinicalTrials.gov (NICHD) SOARS-B: Study of Oxytocin in Autism to improve Reciprocal Social Behaviors (NCT01944046). ClinicalTrials.gov (2021)
Related Dosing Protocols
Educational use only
This guide is an educational research reference, not medical advice or a treatment plan. Approved oxytocin (Pitocin) is a hospital-administered drug. Intranasal, subcutaneous, and sublingual oxytocin remain investigational or research-use only as of June 2026.
Calculate vial math
Use the calculator for custom vial size, BAC-water volume, IU-to-mcg conversion, and syringe-unit math.
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: June 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page