Glutathione Quick Start
Glutathione (often written GSH) is the most abundant antioxidant your body makes on its own. It is a small protein-like molecule called a tripeptide, built from three amino acids: cysteine, glycine, and glutamate. Almost every cell makes it, and the liver makes the most.
People take glutathione for very different reasons, and the route matters a lot. The four routes studied in humans are oral capsules, liposomal or sublingual forms (designed to survive digestion), intranasal spray (studied in Parkinson's research), and intravenous (IV) infusions (used in clinics, often for skin lightening). These are not interchangeable, and the evidence behind each is different.
What it is
A built-in antioxidant tripeptide (cysteine + glycine + glutamate).
Routes studied
Oral, liposomal/sublingual, intranasal, and IV. Each behaves differently.
Oral dosing context
Human trials have used 250-1,000 mg/day orally. Whether it raises body stores is debated.
IV is different
IV is not FDA-approved for skin lightening and carries real safety risks.
Research status
Oral = dietary supplement. Not an FDA-approved drug for these uses.
Educational research reference
This page summarizes how glutathione has been studied and dosed in research and clinical settings. It is not medical advice, not a treatment plan, and not a recommendation to inject anything. Talk to a qualified clinician before using glutathione, especially by injection or IV.
Glutathione Dosing Protocol & Context
There is no single official glutathione dose, because it is not an FDA-approved drug for the uses people search for. What follows is dosing context from published human studies, not a recommendation. The numbers below are what researchers actually used so you can understand the research landscape.
The single most important thing to understand before any dose talk: studies disagree on whether standard oral glutathione even reaches your bloodstream in a useful way. In a 2015 six-month RCT, Richie and colleagues reported that 250 mg/day and 1,000 mg/day raised glutathione in blood, red cells, and other tissues. But a 2011 RCT by Allen and Bradley gave 500 mg twice daily for four weeks and found no change in glutathione status or oxidative-stress markers. A 1992 study gave a single 3 g dose to seven people and saw no rise in blood levels. This is why liposomal and sublingual forms exist.
Glutathione Dosing Context by Route
Choose the route to see the dosing context reported in human studies. None of this is a personal dosing recommendation.
The most common at-home route. Standard capsules, liposomal, or sublingual.
Oral human trials have most often used 250 mg to 1,000 mg per day, sometimes split into two doses. Skin-lightening RCTs frequently used 500 mg/day for 4-12 weeks. The 2015 body-store RCT used 250 mg/day and 1,000 mg/day for six months.
Liposomal and sublingual forms are designed to protect glutathione from being broken down in the gut by the enzyme gamma-glutamyltransferase. Small studies suggest these formats raise whole-blood glutathione better than plain capsules, but sample sizes are small and many studies are funded by the formulation makers. Treat big bioavailability multipliers ("64x," "3-5x") as marketing-adjacent until larger independent trials confirm them.
Timing note
Many supplement labels suggest taking glutathione on an empty stomach. This is convention, not a proven requirement. Effects on skin pigmentation in trials took 4 weeks or longer to appear and faded after stopping.
Studied specifically in Parkinson's disease research, not for skin.
Intranasal glutathione has been studied almost entirely in Parkinson's disease. In Mischley and colleagues' trials, participants used 100-200 mg three times daily (300-600 mg/day total) as a nasal spray for three months.
Important honesty point: in the 2017 Phase IIb trial, the high-dose group improved on the Parkinson's rating scale versus their own baseline, but neither dose beat placebo — the placebo group also improved. So intranasal glutathione looked safe and tolerable, but it did not clearly outperform a saline spray over three months. This is not a proven Parkinson's treatment.
Clinic-administered. Highest risk. Not FDA-approved cosmetically.
IV glutathione is given in clinics, not at home, and is the route tied to the most safety problems. Cosmetic skin-lightening clinics have used roughly 600-1,200 mg per session, once or twice weekly, sometimes with vitamin C. In one IV skin-lightening RCT (Zubair), 1,200 mg twice weekly for six weeks produced modest short-term lightening that faded within six months.
This is not a how-to
IV and injectable glutathione for skin lightening is not FDA-approved. The US FDA issued a June 2019 alert after seven patients had adverse reactions from a compounded glutathione injection contaminated with endotoxins. The FDA Philippines warned of liver, kidney, and nervous-system toxicity and Stevens-Johnson Syndrome risk. Do not attempt self-injection. See the Side Effects section.
Glutathione dosing context by route (from human studies, not a recommendation)
Route
Oral capsule
Studied range
250-1,000 mg/day
Typical study length
4 weeks - 6 months
Evidence note
RCTs conflict on whether it raises body stores
Route
Liposomal / sublingual
Studied range
~300-500 mg/day
Typical study length
1-4 weeks (PK studies)
Evidence note
Small studies suggest better absorption
Route
Intranasal
Studied range
300-600 mg/day split x3
Typical study length
3 months
Evidence note
Safe in PD trials; did not beat placebo
Route
IV (clinic)
Studied range
600-1,200 mg/session
Typical study length
Weekly x6 weeks
Evidence note
Not FDA-approved cosmetically; safety concerns
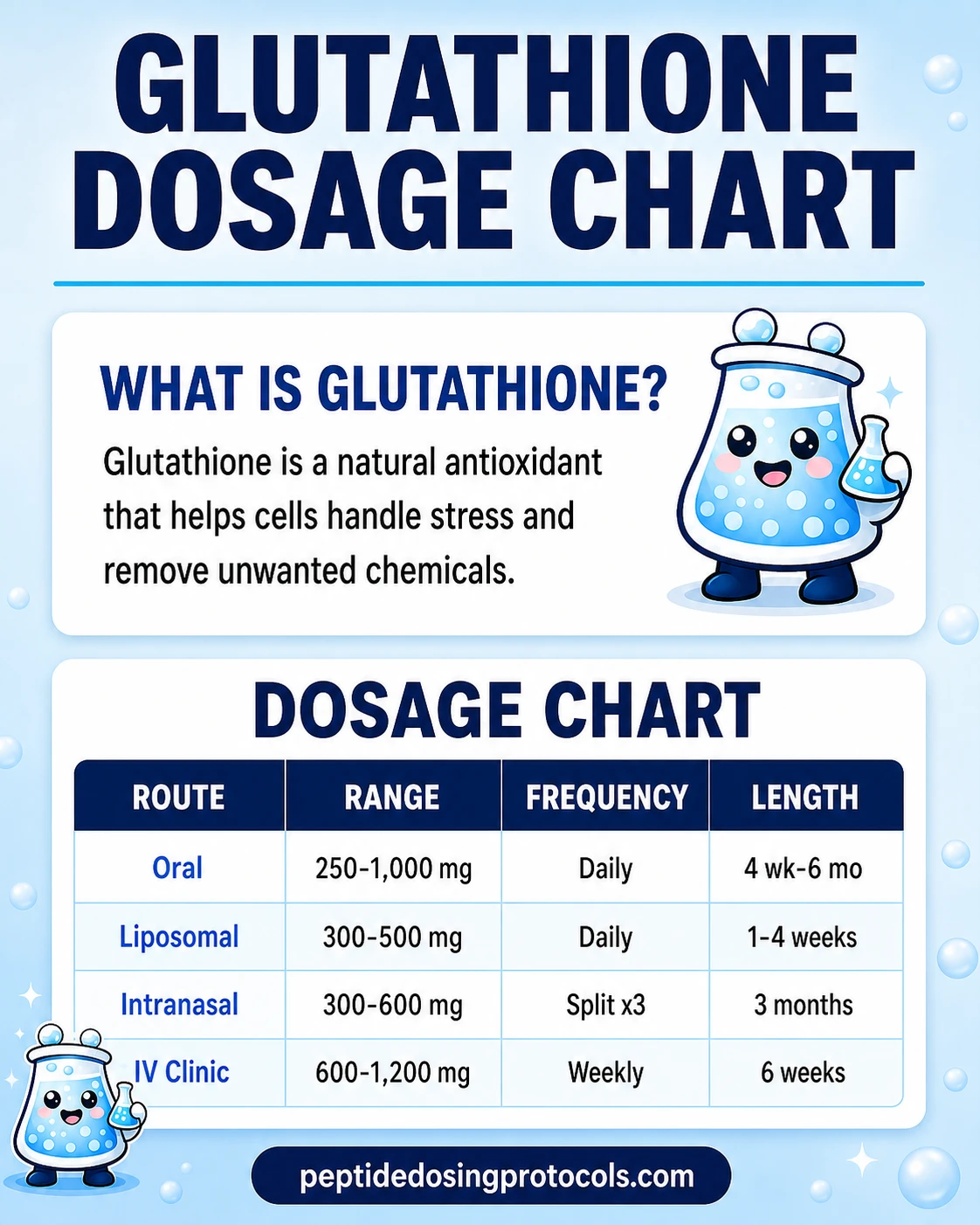
| Route | Studied range | Typical study length | Evidence note |
|---|---|---|---|
| Oral capsule | 250-1,000 mg/day | 4 weeks - 6 months | RCTs conflict on whether it raises body stores |
| Liposomal / sublingual | ~300-500 mg/day | 1-4 weeks (PK studies) | Small studies suggest better absorption |
| Intranasal | 300-600 mg/day split x3 | 3 months | Safe in PD trials; did not beat placebo |
| IV (clinic) | 600-1,200 mg/session | Weekly x6 weeks | Not FDA-approved cosmetically; safety concerns |
Ranges describe what researchers used. They are not dosing instructions. This is not a dosing recommendation.
Evidence boundary
Most glutathione dosing in the wild is community-derived or clinic-marketing-derived, not standardized by regulators. Whether oral glutathione meaningfully changes health outcomes (beyond pigmentation in some trials) remains unproven in large studies.
Glutathione Supplies Needed
Supplies depend entirely on route. Oral and liposomal users need no injection supplies at all. The injectable/reconstitution math below applies only to research-context lyophilized (powder) glutathione that must be reconstituted, and is included for completeness — not as encouragement to self-inject. IV glutathione should be handled by a licensed clinician.
Recommended USA Supply
Use discount code SAVE10 at Orbitrex Peptides checkout. See why we love Orbitrex Peptides.

Glutathione

Compounded Glutathione Injection

At-Home Blood Test
Injection Supplies
Disclosure: supply links may earn PDP a commission at no cost to you.
Oral / Liposomal users
No injection supplies needed. This is the most common route.
| Cycle length | Planning note |
|---|---|
Any 0 syringes | Capsules, liposomal liquid, or sublingual only. |
Any
0 syringes
Capsules, liposomal liquid, or sublingual only.
Research Vials (injectable context only)
Example math for a 600 mg/day research-context plan from a 1,200 mg vial. Illustrative only.
| Cycle length | Planning note |
|---|---|
4 weeks 14 vials | ~28 x 600 mg doses; 2 doses per 1,200 mg vial |
6 weeks 21 vials | ~42 doses needed |
4 weeks
14 vials
~28 x 600 mg doses; 2 doses per 1,200 mg vial
6 weeks
21 vials
~42 doses needed
Bacteriostatic Water
Only if reconstituting a lyophilized research vial.
| Cycle length | Planning note |
|---|---|
4 weeks 1 x 30 mL bottle | Volume depends on vial size and target concentration |
4 weeks
1 x 30 mL bottle
Volume depends on vial size and target concentration
Round up for priming losses and handling. For IV use, supplies and administration belong with a licensed clinician, not a home shopping list. Use the calculator for exact vial math.
Companion Supplies & Routine Support
Glutathione Dosage Chart
This Glutathione dosage chart summarizes the oral, liposomal, intranasal, and clinic IV research-context ranges shown in the dosing section above.
Glutathione Reconstitution Guide
Most people who take glutathione never reconstitute anything — they swallow a capsule or liposomal liquid. Reconstitution only applies to lyophilized (freeze-dried powder) research glutathione intended for injection, which is the highest-risk route and should involve a clinician.
If you are working with a powdered research vial, the math works like every other peptide. Example: a 1,200 mg vial reconstituted with 3.0 mL of bacteriostatic water gives 400 mg/mL. A 0.10 mL draw (10 units on a U-100 syringe) would then deliver 40 mg. Always confirm the actual vial label rather than assuming.
- Let the vial and bacteriostatic water reach room temperature.
- Wipe both rubber stoppers with a fresh alcohol swab.
- Draw your chosen volume of bacteriostatic water into the syringe.
- Inject the water slowly down the inside wall of the vial, not directly onto the powder.
- Swirl gently — do not shake — until fully dissolved and clear.
- Glutathione solutions can look faintly tinted; confirm there are no particles.
- Label with date and concentration, then refrigerate.
Use the calculator
For exact vial size, BAC-water volume, concentration, and syringe-unit math, use the calculator instead of guessing.
How Glutathione Works
In plain English: glutathione is your cells' main cleanup molecule. It grabs onto unstable molecules called free radicals and neutralizes them before they damage cell parts. It also helps the liver tag and remove certain toxins so they can leave the body.
The technical version: glutathione donates an electron from its cysteine sulfur group to neutralize reactive oxygen species. In doing so it becomes oxidized (GSSG), then an enzyme called glutathione reductase recycles it back to the active reduced form (GSH). The ratio of GSH to GSSG is a common lab marker of how much oxidative stress a cell is under.
For skin specifically, glutathione blocks an enzyme called tyrosinase and nudges pigment cells toward making lighter pheomelanin instead of darker eumelanin. That is the mechanism behind the skin-lightening research — and also why regulators worry that lightening could reduce the skin's natural UV protection over time.
One well-established clinical fact anchors all of this: when someone overdoses on acetaminophen (Tylenol), the liver burns through its glutathione detoxifying the drug. The antidote, N-acetylcysteine (NAC), works by refilling the cysteine your liver needs to rebuild glutathione. That is real, FDA-recognized pharmacology, and it explains why cysteine supply is the rate-limiting step for making glutathione.
Who Should Be Cautious With Glutathione
- Pregnant or breastfeeding people: safety has not been established in trials; avoid unless a clinician advises otherwise.
- People with asthma: inhaled/nebulized glutathione has triggered bronchospasm in some reports; the nasal route in Parkinson's trials was separate and monitored.
- Anyone considering IV/injectable glutathione: highest risk group. Sterility, dosing, and product purity problems have caused serious harm.
- People on medications metabolized by the liver: glutathione is part of liver detox pathways; discuss interactions with a clinician.
- G6PD deficiency: relevant when IV glutathione is paired with high-dose IV vitamin C, which the FDA Philippines flagged.
Talk to a clinician first
This list is not complete. Anyone with a chronic condition or who takes prescription medication should talk to a qualified clinician before starting glutathione.
Glutathione Side Effects & Safety
Oral and liposomal
Oral glutathione is generally well tolerated in trials. Reported effects are usually mild: bloating, loose stools, or cramping. In the long oral skin-lightening and body-store trials, lab markers (liver enzymes, kidney values) stayed normal. Some reviews note theoretical concern that lightening skin could lower natural UV protection.
IV and injectable
This is where the serious risks live. In one IV skin-lightening study, about 40% of participants reported abdominal cramps, 32% had deranged liver function tests, and 16% had diarrhea or tingling. Case reports describe anaphylaxis, severe systemic inflammation, acute liver injury, and one report of cardiomyopathy in a glutathione trial participant.
Quality and sterility risk
The biggest injectable danger is not the molecule — it is the product. In January 2019, seven patients at one clinic had reactions within minutes of an IV glutathione infusion that the FDA linked to high endotoxin levels in the powder used to compound it. Unregulated injections also carry infection risks (HIV, hepatitis) when needles or facilities are not sterile.
Regulatory status
As of June 2026, no injectable glutathione product is FDA-approved for skin lightening or general wellness in the United States. The FDA has warned against compounded IV glutathione, and the FDA Philippines issued a public advisory against IV glutathione for skin lightening.
Sensitive-topic note: skin-lightening practices intersect with serious health, cultural, and self-image issues. If skin tone is causing distress, a dermatologist is a safer first stop than a clinic offering IV drips. This is a sensitive area; the safest information here is the information that keeps you away from unregulated injections.
Glutathione Expected Timeline & Monitoring
Timelines depend on the goal. In oral skin-lightening RCTs, measurable melanin-index changes took about 2-4 weeks to appear and continued over 4-12 weeks. Crucially, the lightening faded after people stopped — it was not permanent.
For body-store changes, the 2015 oral RCT saw blood glutathione rise at 1, 3, and 6 months, then return to baseline within one month of stopping. So any effect appears tied to ongoing use.
- Skin pigmentation: weeks to months, reverses after stopping.
- Body glutathione stores: measurable over months, fades on washout.
- Liver markers (NAFLD pilot context): ALT changes seen over ~4 months.
- Monitoring: liver and kidney labs are reasonable for anyone using higher doses or any injectable route, under clinician guidance.
Glutathione Clinical Evidence Context
Here is the honest state of the evidence, strongest to weakest. I read each of these trials directly rather than relying on supplement-brand summaries.
Skin lightening (oral) — most consistent human signal
A 2025 systematic review found five RCTs plus one open-label study where oral glutathione at 250-500 mg/day produced a statistically significant drop in melanin index versus placebo. The effects were modest and reversible. This is the area with the most repeatable human data — and it is cosmetic, not a health cure.
Liver / NAFLD — promising pilot data
A 2017 open-label pilot gave 300 mg/day oral glutathione for four months to NAFLD patients and saw ALT (a liver enzyme) drop. A 2025 review pooled three small trials (109 people total) and found consistent ALT and oxidative-stress improvements. But these are small and uncontrolled or underpowered — not proof.
Parkinson's disease — safe but unproven
Intranasal glutathione was safe and tolerable in Mischley's trials, and the high-dose group improved over baseline. But it did not beat placebo, so it cannot be called an effective treatment.
The oral bioavailability fight
The Richie 2015 RCT said oral works; the Allen 2011 RCT and a 1992 single-dose study said it does not. This unresolved disagreement is the reason liposomal and sublingual products exist, and the reason you should be skeptical of any product promising guaranteed results.
Glutathione Storage & Handling
Storage guidance
Temperature
Oral capsule/liposomal
Room temp, dry
Lyophilized research vial
-4F (-20C) long-term
Reconstituted solution
35.6-46.4F (2-8C)
Light
Oral capsule/liposomal
Keep sealed, away from light
Lyophilized research vial
Away from light
Reconstituted solution
Away from light
Appearance
Oral capsule/liposomal
N/A
Lyophilized research vial
White/off-white powder
Reconstituted solution
Clear; discard if cloudy or particulate
| Oral capsule/liposomal | Lyophilized research vial | Reconstituted solution | |
|---|---|---|---|
| Temperature | Room temp, dry | -4F (-20C) long-term | 35.6-46.4F (2-8C) |
| Light | Keep sealed, away from light | Away from light | Away from light |
| Appearance | N/A | White/off-white powder | Clear; discard if cloudy or particulate |
Liposomal liquids often require refrigeration after opening — follow the label.
Glutathione Troubleshooting
- "My capsules aren't doing anything." Standard oral glutathione may not raise body levels much; this is documented, not a defect. Liposomal/sublingual forms exist for this reason.
- Cloudy reconstituted vial: discard it. Glutathione solution should be clear.
- Skin lightening faded after stopping: expected — trial effects reversed on washout.
- Stomach upset: common with oral; taking with a little food may help, though empty-stomach dosing is the usual convention.
- Considering IV because oral "isn't working": this is the highest-risk route and not FDA-approved cosmetically. Discuss with a clinician instead of switching to injections.
Glutathione Regulatory Status
As of June 2026: oral glutathione is sold in the United States as a dietary supplement, which means it is not reviewed or approved by the FDA as a drug for treating, curing, or preventing disease. Quality and label accuracy vary by brand, so third-party testing matters.
Injectable and IV glutathione is a different story. No injectable glutathione product is FDA-approved for skin lightening or wellness in the US. The FDA issued a June 2019 compounding alert after endotoxin-related adverse events, and the FDA Philippines issued advisory 2019-182 warning against IV glutathione for skin lightening. In some countries injectable glutathione is approved only as an add-on in cisplatin chemotherapy, not for cosmetics.
Glutathione vs NAC vs IV: How the Options Compare
Glutathione options compared
Option
Oral GSH
How it works
Direct glutathione (may be poorly absorbed)
Best-studied use
Skin pigmentation
Main caveat
Bioavailability debated
Option
Liposomal/sublingual GSH
How it works
Protected delivery for better absorption
Best-studied use
Raising blood GSH (small studies)
Main caveat
Mostly maker-funded data
Option
NAC
How it works
Precursor — gives cysteine to build GSH
Best-studied use
Acetaminophen overdose (FDA use)
Main caveat
Indirect; not the same as GSH
Option
IV GSH
How it works
Bypasses the gut entirely
Best-studied use
Clinic cosmetic use (unapproved)
Main caveat
Serious safety + sterility risk
| Option | How it works | Best-studied use | Main caveat |
|---|---|---|---|
| Oral GSH | Direct glutathione (may be poorly absorbed) | Skin pigmentation | Bioavailability debated |
| Liposomal/sublingual GSH | Protected delivery for better absorption | Raising blood GSH (small studies) | Mostly maker-funded data |
| NAC | Precursor — gives cysteine to build GSH | Acetaminophen overdose (FDA use) | Indirect; not the same as GSH |
| IV GSH | Bypasses the gut entirely | Clinic cosmetic use (unapproved) | Serious safety + sterility risk |
These are not interchangeable. NAC is a building block, not glutathione itself.
A common question is glutathione versus NAC. NAC is not glutathione — it is a cheap, well-studied precursor that supplies the cysteine your body needs to build its own glutathione. For raising glutathione indirectly, NAC has stronger pharmacology behind it (it is the hospital antidote for Tylenol overdose). For direct cosmetic pigmentation effects, oral glutathione has the dedicated skin RCTs.
FAQ
Q1: What is glutathione and what does it do?
Glutathione is the most abundant antioxidant your body makes on its own. It is a tripeptide built from cysteine, glycine, and glutamate. It neutralizes free radicals, helps the liver remove certain toxins, and supports the recycling of other antioxidants. Cells measure stress partly by the ratio of active (GSH) to spent (GSSG) glutathione.
Q2: How much glutathione per day do studies use?
Human oral trials have most often used 250 mg to 1,000 mg per day, with skin-lightening RCTs frequently using 500 mg/day for 4 to 12 weeks. These are study amounts, not a personal recommendation, and glutathione is not an FDA-approved drug for these uses. Talk to a clinician about what is appropriate for you.
Q3: Does oral glutathione actually work, or is it broken down in the stomach?
This is genuinely debated. A 2015 six-month RCT found oral glutathione raised body stores at 250 and 1,000 mg/day. But a 2011 RCT at 500 mg twice daily found no change, and a 1992 single 3 g dose did nothing. The gut enzyme gamma-glutamyltransferase breaks glutathione down, which is why liposomal and sublingual forms were created.
Q4: Does liposomal glutathione work better than regular capsules?
Small studies suggest liposomal and sublingual forms raise whole-blood glutathione more than plain capsules, because the lipid coating helps it survive digestion. However, many of these studies are small and funded by the formulation makers, and dramatic claims like "64x more bioavailable" should be treated cautiously until larger independent trials confirm them.
Q5: Is glutathione safe?
Oral glutathione is generally well tolerated in trials, with mild effects like bloating or loose stools. IV and injectable glutathione is a different risk category: it is not FDA-approved for cosmetic use, and the FDA issued a 2019 alert after seven patients reacted to a contaminated compounded injection. Reactions have included anaphylaxis and liver injury.
Q6: Does glutathione lighten skin?
In several oral RCTs at 250-500 mg/day, glutathione produced a modest, statistically significant drop in melanin index versus placebo, with effects appearing in 2-4 weeks. The lightening was temporary and reversed after stopping. It works by inhibiting tyrosinase and shifting pigment toward lighter pheomelanin. This is a cosmetic effect, not a health benefit, and regulators have raised UV-protection concerns.
Q7: Where do clinics inject glutathione, and can I do it myself?
Glutathione for skin lightening is given by clinics intravenously, not by patients at home. Self-injection is strongly discouraged: IV glutathione is not FDA-approved for cosmetic use, and unregulated or contaminated products have caused serious harm including endotoxin reactions and infections. If you are considering it, talk to a licensed clinician rather than attempting it yourself.
Q8: Does Tylenol (acetaminophen) deplete glutathione?
Yes. When the liver processes acetaminophen, it uses up glutathione, and an overdose can deplete it dangerously. That is exactly why the hospital antidote for acetaminophen overdose is N-acetylcysteine (NAC), which refills the cysteine your liver needs to rebuild glutathione. This is well-established, FDA-recognized pharmacology.
Q9: Is glutathione good for the liver?
Early human data is encouraging but limited. A 2017 pilot study gave 300 mg/day oral glutathione to NAFLD patients for four months and saw liver enzyme (ALT) levels fall, and a 2025 review of three small trials found similar improvements. These studies are small and not definitive, so glutathione is not a proven liver treatment.
Q10: Can you take glutathione while pregnant?
There is not enough safety data to recommend glutathione supplements during pregnancy or breastfeeding. Most trials excluded pregnant participants. The safest course is to avoid it unless a qualified clinician specifically advises otherwise.
Q11: When is the best time to take glutathione?
Many labels suggest an empty stomach, often in the morning, but this is convention rather than a proven requirement. Consistency over weeks matters more than time of day, since skin-pigmentation effects in trials took at least 4 weeks to appear and faded after stopping.
Q12: Is this page medical advice?
No. This is an educational research reference summarizing how glutathione has been studied and dosed. It is not medical advice, a treatment plan, or a recommendation to inject anything. Talk to a qualified clinician before using glutathione, especially by any injectable route.
Sources & Research
- 1. Richie JP Jr, Nichenametla S, Neidig W, et al. Randomized controlled trial of oral glutathione supplementation on body stores of glutathione. European Journal of Nutrition (2015)
- 2. Allen J, Bradley RD. Effects of oral glutathione supplementation on systemic oxidative stress biomarkers in human volunteers. Journal of Alternative and Complementary Medicine (2011)
- 3. Arjinpathana N, Asawanonda P. Glutathione as an oral whitening agent: a randomized, double-blind, placebo-controlled study. Journal of Dermatological Treatment (2012)
- 4. Handog EB, Datuin MS, Singzon IA. An open-label, single-arm trial of a glutathione lozenge as a skin-lightening agent in Filipino women. International Journal of Dermatology (2016)
- 5. Sarkar R, et al. Glutathione as a skin-lightening agent and in melasma: a systematic review. International Journal of Dermatology (2025)
- 6. Weschawalit S, Thongthip S, Phutrakool P, Asawanonda P. Glutathione and its antiaging and antimelanogenic effects. Clinical, Cosmetic and Investigational Dermatology (2017)
- 7. U.S. Food and Drug Administration. FDA highlights concerns with using dietary ingredient glutathione to compound sterile injectables (Compounding Alert). FDA Human Drug Compounding (2019)
- 8. Food and Drug Administration (Philippines). FDA Advisory No. 2019-182: Unsafe use of glutathione as skin-lightening agent. FDA Philippines (2019)
- 9. Honda Y, Kessoku T, Sumida Y, et al. Efficacy of glutathione for the treatment of nonalcoholic fatty liver disease: an open-label, single-arm, multicenter, pilot study. BMC Gastroenterology (2017)
- 10. Mischley LK, Lau RC, Shankland EG, Wilbur TK, Padowski JM. Phase IIb study of intranasal glutathione in Parkinson's disease. Journal of Parkinson's Disease (2017)
- 11. Mischley LK, Leverenz JB, Lau RC, et al. A randomized, double-blind phase I/IIa study of intranasal glutathione in Parkinson's disease. Movement Disorders (2015)
- 12. Schmitt B, et al. A targeted metabolomic assessment of oral glutathione bioavailability and safety in humans: a randomized crossover clinical trial. Antioxidants (2026)
- 13. Pedre B, et al. Existing and potential therapeutic uses for N-acetylcysteine: the need for conversion to intracellular glutathione. Pharmacology & Therapeutics (2013)
Related Dosing Protocols
Educational use only
This guide is an educational research reference, not medical advice or a treatment plan. Glutathione is not an FDA-approved drug for the uses discussed here, and injectable glutathione is not FDA-approved for cosmetic use.
Calculate vial math
Use the calculator for custom vial size, BAC-water volume, and syringe-unit math.
Written by Garret Grant
Founder & Lead Researcher · B.S. Civil Engineering, UCLA
Last updated: July 2026
Human-researched and AI-assisted with full editorial review. I verify sources, protocol interpretation, and final judgments personally. See methodology.
Share this page